Herpes zoster: improving protection in older people

Immunisation
Although antivirals can help reduce the severity and duration of acute herpes zoster (HZ), the best protection against the disease is to boost an individual’s immunity by vaccination with the live attenuated HZ vaccine. A new recombinant HZ subunit vaccine holds promise to further reduce the burden of HZ and its complications.
- Herpes zoster (HZ) is common and associated with a considerable burden of morbidity.
- Vaccination against HZ is the most effective strategy to provide increased protection against both acute zoster and postherpetic neuralgia.
- A recommendation from the GP to receive the zoster vaccination is the most effective strategy to increase HZ vaccine coverage.
Herpes zoster (HZ), or shingles, is a neurocutaneous disease that occurs when varicella-zoster virus (VZV) latent in sensory ganglia reactivates and replicates to cause dermatomal pain and a vesicular rash.1,2 These events occur when VZV-specific cell-mediated immunity (CMI) falls below a critical level, which typically happens when it is compromised by disease, medical treatment or ageing.3 The exact triggers for reactivation of the virus in an individual are unknown.
Exogenous, circulating wild-type virus episodically boosts adult T cell immunity (e.g. through exposure to children with chickenpox) so that reactivation usually occurs as a result of naturally waning CMI with age or induced immunosuppression.4
Up to one-third of the population is at risk of developing HZ during their lifetime, and two-thirds of people with the disease are aged 50 years or older.5 In the Australian context, HZ affects 120,000 people every year.6
Risk factors
The increased incidence of HZ is most marked after 50 years of age and continues to rise with age. This is likely to be related to decline in CMI in older people.3 Other risk factors for HZ include: female sex, being immunocompromised and having a family history of HZ.7,8
Reactivation of VZV leads to a localised inflammatory response, with nerve-cell damage and subsequent ganglionitis. The degree of inflammation correlates with both the disease severity and the risk of complications.9
The risk and severity of HZ is considerably higher in immunosuppressed individuals and proportional to the severity of immunosuppression. Therefore, it is recommended that individuals consider, in conjunction with specialist advice, having HZ vaccination before starting immunosuppressive therapy.
Guidance on the use of the HZ vaccine in patients who are immunocompromised, developed by the National Centre for Immunisation Research and Surveillance (NCIRS),10 is summarised below in the section on Prevention. Discussions between GPs and specialists (e.g. a haematologist) on whether the HZ vaccine can be used in a particular patient who is immunocompromised is recommended.
Clinical manifestations
HZ arises from the reactivation of the VZV after latent infection in the trigeminal and dorsal root ganglia and results in the virus being transferred along nerves to the skin. The exact mechanisms for reactivation are unknown but correlate with a reduction in controlling T cell immunity. A prodromal period of dermatomal pain often precedes the acute eruption by several days, occasionally longer. The character of the acute pain (neuritis) in the affected dermatome has been variously described as burning, deep aching, tingling, itching or stabbing.
Patients not uncommonly experience neuropathic pain. Depending on the degree of neuritis/ganglionitis, this includes:
- paraesthesia (burning and tingling)
- anaesthesia/dysaesthesia (reduced or altered sensation)
- debilitating allodynia (pain induced by nonpainful stimuli such as touch)
- hyperaesthesia (exaggerated or prolonged response to pain).
Although such symptoms usually start during the acute phase, they may also be associated with ongoing pain (for 30 to 90 days after onset) or chronic pain (beyond 90 days after onset). Moderate- to-severe pain persisting for more than 90 days is known as postherpetic neuralgia (PHN).
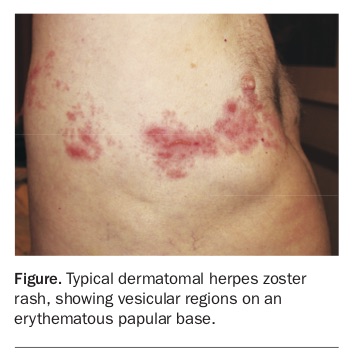
The acute rash of HZ is often pruritic as well as tender, and spreads throughout the affected dermatome (Figure). It evolves through a papular stage to a vesicular stage (lasting three to five days) and then crusts over five to seven days. Acute HZ takes two to four weeks to heal.
{kind=link}
Acute HZ has a significant impact on patients’ quality of life. In one recent study, three-quarters of the patients were experiencing significant pain within the first two weeks of onset, more than half had problems with their usual activities, 36% had issues with either mobility or anxiety and almost one in five had problems with self-care. The patients’ doctors were more likely to underestimate rather than overestimate the patients’ pain.11
Diagnosis
HZ is usually diagnosed clinically. Laboratory diagnosis (involving the detection of VZV antigens or nucleic acid from swabs of lesions, or by VZV-specific immunogloblin [Ig] M antibody tests) is recommended when the clinical picture is atypical or complicated. Examples include when there is persistent or recurrent rash, atypical rash such as a single lesion, central nervous system (CNS) involvement or disseminated rash with immunosuppression.12,13
Complications
Postherpetic neuralgia
The most frequent and important complication of VZV reactivation is PHN. One in five patients aged over 50 years with HZ will still report pain six months after HZ onset despite adequate antiviral therapy, and the incidence rises with age.14,15
The pathogenesis of PHN in the CNS is still being defined. It often leads to impairment of quality of life and prolonged hospitalisation, particularly in older people,16 and treatment is difficult. Although oral aciclovir given within 72 hours of the onset of HZ rash does reduce the severity and duration of acute HZ, it does not reduce significantly the incidence of PHN.17 Thirty to fifty percent of patients who have pain three months after the onset of zoster still have pain four years later.14
Risk factors for PHN include:
- older age
- greater prodromal pain
- severe pain and rash
- ophthalmic involvement.18
Severe immunosuppression and diabetes have also been shown to be significantly associated with PHN.18
Severity of disease at presentation and depression are the major correlates of pain burden in patients with acute HZ and PHN.19
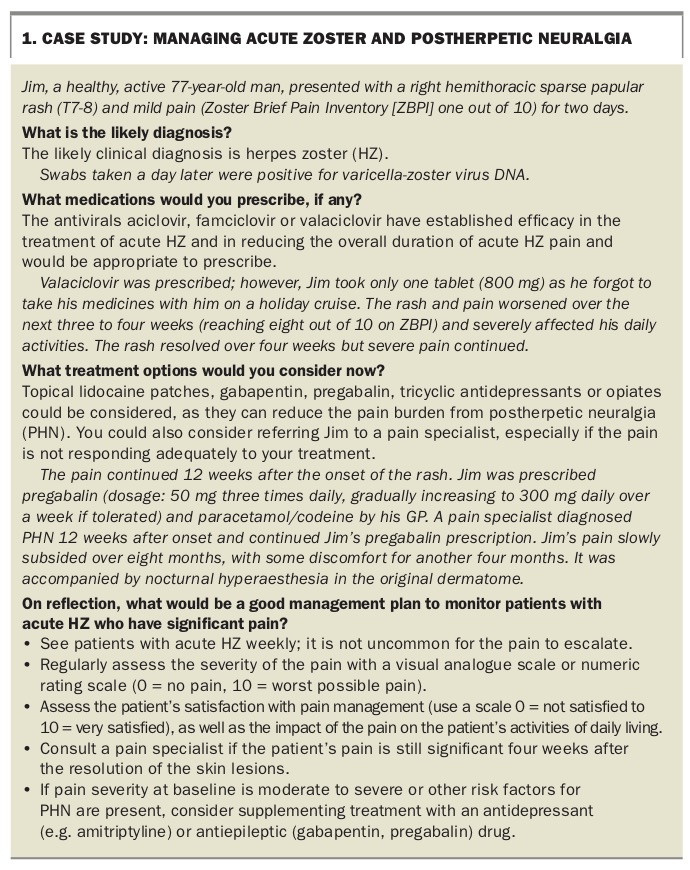
The case study in Box 1 illustrates some of the issues in the management of patients with acute HZ and significant pain.
{kind=link}
Other complications
VZV reactivation may also cause ophthalmic disease (1.5%), dissemination (1.3%), a wide variety of neurological symptoms (0.6%) including motor neuropathy, and vasculitis (0.2%).20
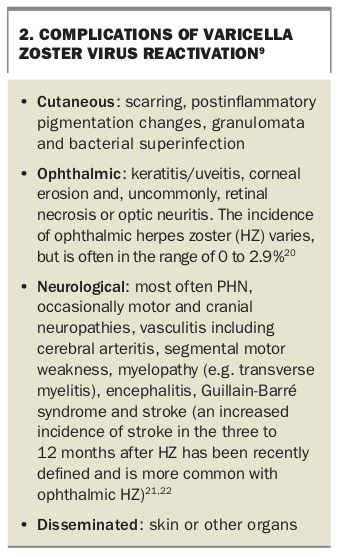
Box 2 lists the complications of VZV reactivation.9,20-22
{kind=link}
Treatment
Acute zoster
Pain relief
Analgesic treatment of acute HZ should follow the three-step WHO pain ladder, based on pain severity, and individual considerations:
- mild pain intensity – NSAIDs or other nonopioids
- moderate pain – nonopioids in combination with weak opioid analgesics
- severe pain – nonopioids combined with strong opioids, if needed.23
If a patient’s pain severity at baseline is moderate to severe or other risk factors for PHN are present, it is worth considering supplementing with an antidepressant (e.g. amitriptyline, nortriptyline; not a licensed indication) or antiepileptic (gabapentin, pregabalin) drug.23
Herpes zoster antiviral therapy
Three antiviral drugs (aciclovir, valaciclovir and famciclovir) have established efficacy in the treatment of acute HZ by accelerating the resolution of lesions, reducing viral shedding and decreasing the severity of acute pain. They also reduce the overall duration of acute HZ pain. Valaciclovir and famciclovir are usually preferred because of their better oral absorption, higher blood levels and easier dosing.24 Oral aciclovir does not reduce the incidence of PHN significantly and there is insufficient evidence to determine the effect of other antiviral treatments on PHN.17
Corticosteroids
Controlled trials of prednisone (in doses of 40 mg daily for seven days, tapering by 5 mg daily over the subsequent two weeks) have shown benefit, particularly for acute HZ pain and quality of life.25,26 In contrast, there is no evidence that corticosteroids reduce the incidence of PHN,25 nor the total duration of pain.27 Corticosteroids should not be used for acute HZ without concomitant administration of antiviral drugs, as they are immunosuppressive.
Postherpetic neuralgia
There is reasonable evidence that pharmacotherapy such as topical lidocaine patches, gabapentin, pregabalin, tricyclic antidepressants or opiates can reduce the pain burden from PHN.28-33 Opioids should not be considered for first-line therapy, given the uncertainty regarding long-term efficacy and concern about safety.34
PHN remains difficult to treat. Fewer than half the patients with PHN in clinical trials of available therapies have had a 50% or greater reduction in pain.14 In addition, adverse effects are common, particularly in older patients.14
Prevention
The best protection against HZ is to boost an individual’s immunity by vaccinating with the HZ vaccine. The live attenuated HZ vaccine is currently the only vaccination available in Australia to prevent HZ. This vaccine is effective in preventing HZ and PHN. It is licensed in Australia for adults 50 years and over. It is recommended for immunocompetent adults aged 60 years and older and is funded under the National Immunisation Program (NIP) for those aged between 70 and 79 years. As 95% of young adults have had varicella infection it is not necessary to check immunity.
The efficacy of this vaccine was examined in the Shingles Prevention Study, a double-blind randomised-controlled trial conducted with more than 38,000 people over the age of 60 years.35 Subjects received a concentrated (14-fold) form of the live attenuated varicella (Oka strain) vaccine and were followed for a median of 3.1 years. This vaccine was shown to be both safe and efficacious, preventing HZ in 51% of subjects, preventing PHN in 66% of subjects and reducing the burden of illness (a measure of severity and duration of pain) by 61%.
Although the efficacy of the live attenuated HZ vaccine in preventing shingles was found to be reduced in people over the age of 70 years and waned further with increasing age, the beneficial effect of the vaccine on the severity of illness and the incidence of PHN was similar among older subjects.35,36
Subsequent follow-up studies suggested efficacy may wane, probably over five to eight years.36 This has led to suggestions that a booster may be necessary at 10 years, although there are no current international recommendations for this.
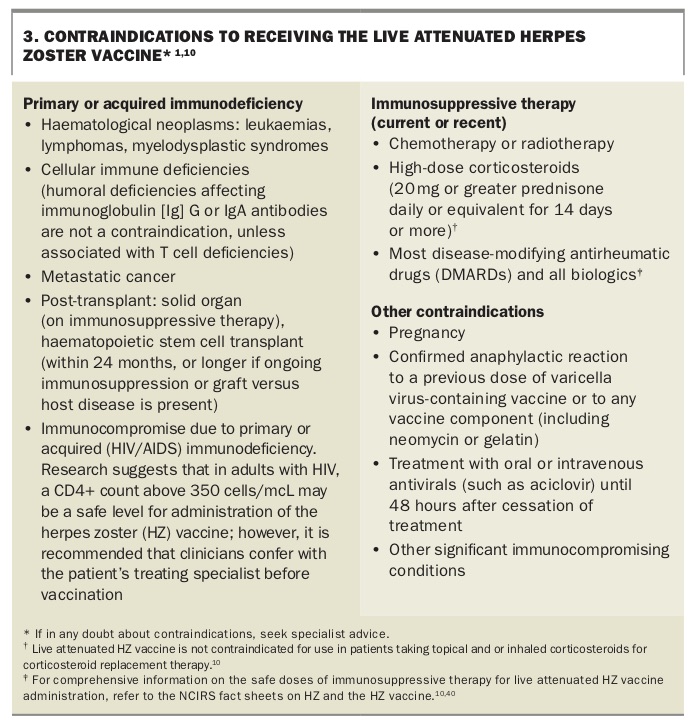
The HZ vaccine contains live, attenuated VZV and is therefore contraindicated in patients who are significantly immunocompromised. Disseminated HZ and death have occurred postvaccination in patients with malignant haematological disorders.37,38
Although anti-tumour necrosis factor biologics are listed as a contraindication to the live attenuated HZ vaccine, it appears safe in patients receiving these drugs.39 However, more studies are needed to define vaccine safety with other biologics and in moderately immunocompromised patients.
Contraindications to the live attenuated HZ vaccine, including specific immunocompromising conditions, are listed in Box 3.1,10 Comprehensive information on the safe doses of immunosuppressive therapy and timing restrictions for administering HZ vaccine in patients taking these medications are provided in the NCIRS fact sheets on HZ and the HZ vaccine.10,40 In addition, it is suggested that all healthcare providers use the prevaccination checklist, a screening tool that highlights the various contraindications to the live attenuated HZ vaccine (https://beta.health.gov.au/search/pre-vaccination).41
{kind=link}
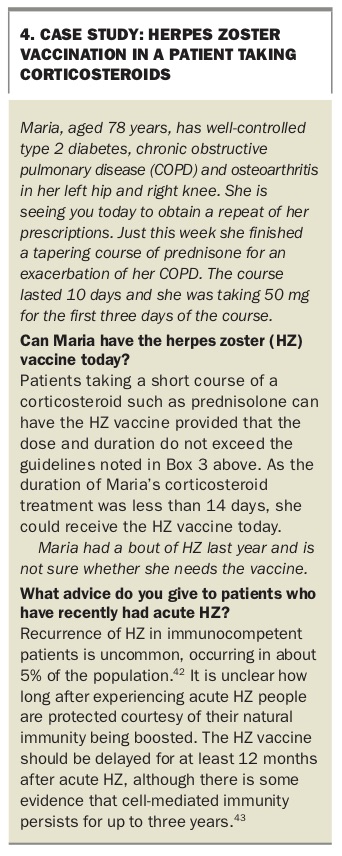
HZ vaccination in a patient with past HZ who has recently taken a course of corticosteroid is discussed in the case study in Box 4.42,43
{kind=link}
Improving protection against herpes zoster
Increasing vaccine uptake
Since the HZ vaccine was launched on the Australian NIP in November 2016, its uptake has been strong in the 70- to 79-year-old age group, with estimated vaccine coverage levels now above 60% of the target group (personal communication, Jim Malamatinas, 5 December 2018). This estimate is based on doses of HZ vaccine delivered to GP practices and is not a formal estimate of coverage. The latter should be available in the next few months. Nevertheless, a significant proportion of the target group remain unvaccinated.
Several factors have been shown to affect the uptake of the HZ vaccine. One of the most important influences in patients having HZ vaccination is a recommendation from their GP. Some tips on discussing HZ vaccine with older patients appear on page 31 of this Supplement.
Patient concerns and beliefs that may decrease HZ vaccine uptake include:
- Concerns about:44-49
– the vaccine’s efficacy
– adverse effects from, and allergic reaction to, the vaccine - beliefs that:44-46,48,50
– there is no need for vaccine as they rarely get sick
– they already have good immunity to HZ
– they are at low risk of getting HZ
– vaccines weaken the immune system and natural immunity is more important
– the vaccine can cause HZ.
Difficulty in attending their GP and their GP not discussing the HZ vaccine have also been shown to reduce patients’ HZ vaccine uptake.44,46,49,51,52
The following factors have been shown to increase the uptake of HZ vaccine:44-54
- GP recommending to have the vaccine
- older age
- female sex
- higher level of education
- friends or relatives affected by HZ or PHN
- belief that HZ can be severe
- higher awareness about HZ and the HZ vaccine
- regular user of influenza or pneumococcal vaccines
- having a regular GP
- availability of the vaccine.
A number of other factors, including the presence of chronic disease, such as diabetes, being a smoker, infrequent GP attendance and patient health status, have shown mixed or unclear effects on vaccine uptake.46,55-59
Improved zoster vaccines
The declining efficacy of live attenuated HZ vaccine with age, especially in those over the age of 70 years, has left a substantial unmet medical need in this growing population. Furthermore, this vaccine is contraindicated in severely immunocompromised patients, in whom HZ is common and often severe.
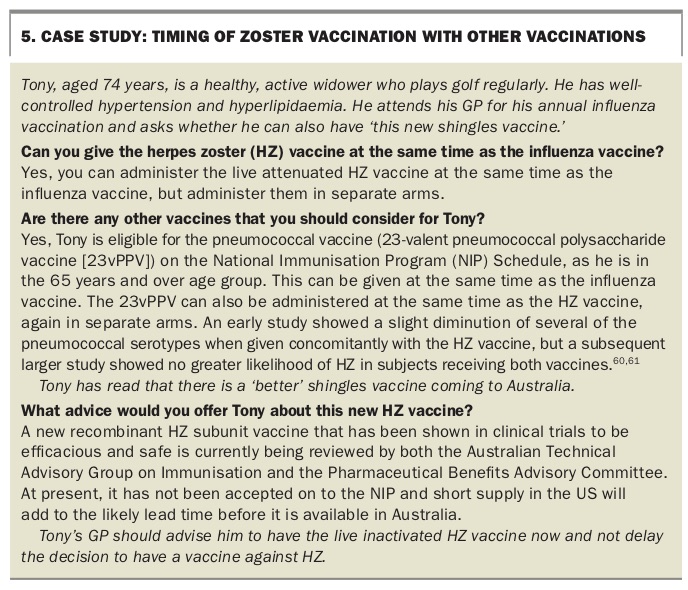
A new recombinant herpes zoster subunit vaccine HZ/su is available in the US and is also licensed in Canada, Europe and Japan. The new vaccine has been registered by the TGA but is not yet available in Australia (see the case study in Box 5).60,61
{kind=link}
The HZ/su vaccine has several advantages over the live attenuated HZ vaccine:3
- its adjuvant system stimulates strong cellular and humoral responses
- it achieves higher levels of effectiveness against acute HZ and PHN (about 90%)
- it can be used in patients who are immunocompromised
- no significant decline in efficacy has been observed between years one and four postimmunisation, and immune responses plateau for up to nine years. Duration of efficacy beyond four years is currently being studied.3,62,63
Furthermore, in a recent systematic review of the two zoster vaccines, the HZ/su vaccine, was statistically superior to both the live attenuated vaccine (vaccine efficacy, 85%; 95% credible interval, 31 to 98%) and placebo (vaccine efficacy, 94%; 95% credible interval, 79 to 98%).64
Nevertheless, the HZ/su vaccine had a much higher incidence of both local and systemic adverse reactions. It was associated with statistically more adverse events at injection sites than the live attenuated vaccine (relative risk, 1.79; 95% credible interval, 1.05 to 2.34; risk difference, 30%; 95% credible interval, 2 to 51%) and placebo (relative risk, 5.63; 95% credible interval, 3.57 to 7.29; risk difference, 53%; 95% credible interval, 30 to 73%). There were also statistically more systemic adverse events in subjects receiving HZ/su than in the placebo and the live attenuated HZ vaccine groups (relative risk, 2.28; 95% credible interval, 1.45 to 3.65; risk difference, 20%; 95% credible interval, 6 to 40%).64
The immunogenicity and efficacy of HZ/su vaccine depends on a two-dose regimen. In the phase III trials, 96% of subjects returned for a second dose.62,63 The compliance with a second dose in field conditions will become apparent soon from the US experience.
Conclusion
HZ is a common and often disabling condition in the older population. Although antivirals help to reduce the severity and duration of the acute phase, the main intervention available to reduce the incidence of PHN is vaccination with the live attenuated HZ vaccine.
A newer and more effective subunit recombinant HZ/su vaccine will become available to prevent HZ and will help to extend this protection to immunocompromised subjects.
GPs are key in achieving higher levels of vaccine coverage, as a recommendation to the patient to receive the HZ vaccine significantly increases the likelihood of the patient being vaccinated. MT