Dulaglutide: a once-weekly GLP-1 receptor agonist for type 2 diabetes

Diabetes type 2
Diabetes medicines
The recent PBS listing of dulaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist that is injected weekly, makes it a realistic choice for the treatment of selected patients with type 2 diabetes. What do clinicians need to know about dulaglutide?
Dulaglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist that requires only once-weekly administration and has been shown to be an effective glucose-lowering agent for patients with type 2 diabetes. Its recent PBS listing makes it a realistic therapeutic choice for many patients. This article summarises what clinicians need to know about dulaglutide and its use in patients with type 2 diabetes.
Type 2 diabetes and the GLP-1 receptor agonists
Type 2 diabetes is a complex medical problem in which hyperglycaemia is often associated with other metabolic issues, including obesity, hypertension and dyslipidaemia. Medical management can be complicated, particularly in light of the expanding number of treatment options. Avoiding hypoglycaemia and weight gain, a consequence of some treatments, is increasingly driving the choice of agent. Importantly, agents that avoid these problems can allow patients to achieve lower glycated haemoglobin (HbA1c) targets, when clinically appropriate.
More recently, a consideration in treatment choice has been the cardiovascular benefit shown with some agents in high-risk patients. This potential benefit is likely to be highlighted in future versions of Australian guidelines on treatment choice for patients with type 2 diabetes, as it is in international guidelines.
In this context, the GLP-1 receptor agonists have been an important addition to the medical management of patients with type 2 diabetes. These medications mimic the action of GLP-1 (i.e. they increase insulin and decrease glucagon secretion in a glucose-dependent manner, decrease appetite and increase satiety) and thereby lower glucose levels, while avoiding hypoglycaemia, and produce weight loss. Although endogenous GLP-1 is usually degraded within minutes by the dipeptidyl peptidase-4 (DPP-4) enzyme, the GLP-1 receptor agonists are designed to resist such enzymatic activity and thus remain active for a prolonged period. On average, when a GLP-1 receptor agonist is added to diet and exercise for longer than six months, a lowering of HbA1c by about 1% (11mmol/mol) has been demonstrated, along with weight loss of 1 to 3 kg.1
Until recently, exenatide and liraglutide were the only GLP-1 receptor agonists available in Australia (lixisenatide is TGA-approved but not available). Compared with exenatide, liraglutide is more effective at glucose-lowering, and it has been approved by the TGA for the management of type 2 diabetes and, at a higher dosage (3mg daily), for the management of obesity.2 Liraglutide at a dosage up to 1.8mg daily has also been shown to reduce major adverse cardiovascular outcomes in some patients with type 2 diabetes at high cardiovascular risk.3
This favourable metabolic profile means that the GLP-1 receptor agonists are increasingly used as an adjunct to oral glucose-lowering therapy and/or insulin. Limitations to their use include the possible adverse effects of nausea and diarrhoea (in more than 10% of patients), vomiting, constipation and abdominal pain, which can lead some patients to discontinue therapy.1-8 Furthermore, the need to inject the GLP-1 receptor agonists (liraglutide once daily and exenatide twice daily) can limit their acceptability, although usually only transiently. The development of once-weekly modified-release exenatide was welcomed.4 Dulaglutide, which is also injected once weekly, provides an additional treatment option.
What is dulaglutide?
Dulaglutide is a long-acting GLP-1 receptor agonist that can be administered weekly, at any time of the day, because of its long half-life of about five days. Maximum blood concentrations are seen 24 to 72 hours after dosing, and steady-state levels after about two to four weeks with once-weekly administration. Dulaglutide can be administered at the same subcutaneous sites as used for insulin (i.e. abdomen, thigh and upper arm), with the choice of site not affecting its pharmacokinetic properties. It is not necessary to adjust the dose based on renal or hepatic dysfunction, although dulaglutide is not recommended when the estimated glomerular filtration rate (eGFR) is less than 30mL/min.
When can dulaglutide be used?
Dulaglutide is TGA-approved for the treatment of patients with type 2 diabetes mellitus and can be used as an adjunct to oral hypoglycaemic agents and/or prandial insulin. Specifically, dulaglutide is approved as an adjunct to diet and exercise to improve glycaemic control in adults with type 2 diabetes:
- as monotherapy
- combined with the following oral glucose-lowering therapies – metformin, metformin and sulfonylurea, or metformin and thiazolidinedione
- combined with insulin, with or without metformin.
The use of dulaglutide in children has not been studied, and it is therefore not recommended in people under the age of 18 years. Therapeutic experience is limited in people aged 75 years or older, but dose adjustment is not necessary.
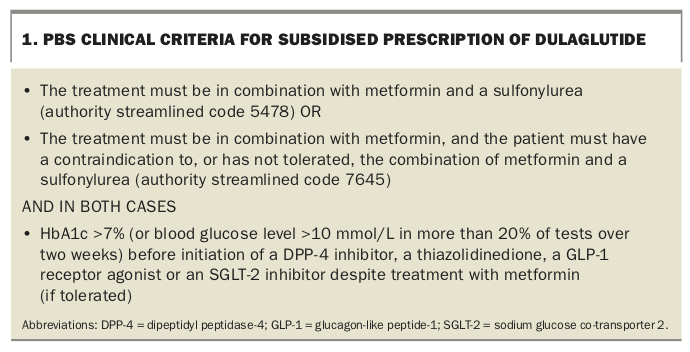
Dulaglutide is PBS-listed for use in patients with uncontrolled type 2 diabetes:
- in combination with metformin (dual therapy), or
- in combination with metformin and a sulfonylurea (triple therapy; Box 1).
{kind=link}
It is important to note that dulaglutide is not PBS-subsidised for use as monotherapy or in combination with a DPP-4 inhibitor (gliptin), a thiazolidinedione (glitazone), a sodium-glucose cotransporter 2 (SGLT-2) inhibitor, a sulfonylurea alone or insulin.
What is the evidence?
The efficacy of dulaglutide has been established in six head-to-head phase 3 trials that involved more than 5000 patients: the AWARD study series 1 to 6.5-10 In these studies, dulaglutide was compared with other GLP-1 receptor agonists, with oral glucose-lowering agents or with insulin. Dulaglutide and the comparator were given either as monotherapy or in combination with other glucose-lowering therapy.
Dulaglutide was as effective as, if not superior to, all compared treatments in lowering HbA1c and produced clinically significant weight loss.5-10 However, dulaglutide was accompanied by a higher incidence of nausea, vomiting and diarrhoea (up to 21%) compared with placebo (less than 7%).
It is important to note that the AWARD studies contained relatively few patients aged over 75 years or under 18 years, patients with a creatinine clearance less than 30mL/min or pregnant or breastfeeding women.5-10
Dulaglutide as second-line therapy combined with metformin
Most often when a sulfonylurea is not tolerated or not considered appropriate as second-line therapy after metformin, the choice is between a DPP-4 inhibitor, an SGLT-2 inhibitor or a GLP-1 receptor agonist. In general, the GLP-1 receptor agonists are considered to have greater glucose-lowering efficacy than DPP-4 inhibitors. For example, in the AWARD-5 study (dulaglutide vs sitagliptin as add-on in metformin-treated patients), dulaglutide significantly reduced HbA1c by -1.1% (-12mmol/mol) versus -0.4% (-0.4mmol/mol) with sitagliptin.9 In people with obesity (body mass index, 31kg/m2), weight loss after 12 months was also greater with dulaglutide (-3kg vs -1.5kg), but gastrointestinal upset (nausea, diarrhoea and vomiting) was more frequent. Discontinuation rates at one year were similar (11% for dulaglutide vs 10% for sitagliptin), and similar to those for other diabetic treatments.9
Exenatide twice daily is the only GLP-1 receptor agonist available on the PBS that has been compared with dulaglutide. The AWARD-1 study showed that dulaglutide had slightly greater efficacy for HbA1c reduction than twice-daily exenatide (-1.5% [-17mmol/mol] vs -1% [-11mmol/mol]), but led to similar weight loss (about 1 to 2 kg).5 Dulaglutide weekly was compared with liraglutide daily in the AWARD-6 study, which found a similar reduction in HbA1c but greater weight loss with liraglutide (-3.6kg vs -2.9kg).10 Fewer patients discontinued dulaglutide compared with the comparator GLP-1 receptor agonists.
Dulaglutide versus basal insulin for patients on maximum tolerated doses of oral agents
In clinical practice, when a patient requires maximum doses of two oral glucose-lowering agents, the addition of a basal insulin is a common clinical choice. This advice is resisted by many patients, often because of concerns about hypoglycaemia and weight gain. Both of these concerns can be allayed by choosing dulaglutide, which also has the advantage of requiring less frequent injection than insulin.
In the AWARD-2 study, dulaglutide was compared with insulin glargine as add-on therapy to metformin plus a sulfonylurea.6 Dulaglutide 1.5 mg led to a decrease of -1.0% (-11mol/mol) in HbA1c compared with a decrease of -0.6% (-7mol/mol) in those taking insulin glargine. Dulaglutide provided sustained HbA1c reduction for up to two years, and 53% of participants achieved an HbA1c goal of less than 7% (53mol/mol) compared with 31% of those taking insulin glargine. Participants taking dulaglutide 1.5mg had lower rates of hypoglycaemia (1.7%) than those taking insulin glargine (3%). The dulaglutide group had an average weight loss of about 2kg, compared with an average weight gain of 1.4kg in the insulin group.
Dulaglutide versus metformin as monotherapy
The lack of PBS reimbursement for dulaglutide monotherapy means that currently its use in this manner will probably be minimal. In fact, although statistically significant differences in HbA1c lowering were seen between dulaglutide and metformin, these differences would not be considered clinically relevant.7 At one year, dulaglutide showed superior reduction in HbA1c (-0.8% [-9mol/mol]) compared with metformin (-0.6% [-7mol/mol]), and 62% of patients achieved the goal of HbA1c less than 7% (53mol/mol) on dulaglutide compared with 54% on metformin. Weight loss of about 2kg was similar in the two groups. No severe hypoglycaemia was observed.7
How is dulaglutide used?
Dulaglutide is presented as a single-dose (1.5mg), once-weekly injectable therapy. The dose is contained in a ready-to-use subcutaneous injectable pen. It is easier to handle and administer than modified-release exenatide, the other weekly GLP-1 receptor agonist available in Australia, which requires reconstitution and priming and has specific temperature requirements.
Dulaglutide can be given independently of food, other medications and time of day, and may be left unrefrigerated for up to 14 days. In injection-naïve patients, 99% found administration easy and were successfully injecting after three weeks, and 97% were willing to continue after three injections.4
If a patient misses a dose of dulaglutide then they should take it when they remember, as long as it is administered at least three days before the next dose. If less than three days remain before the next dose is due then the missed dose should be skipped, and the next dose administered on the usual scheduled day.
Adverse effects and safety profile
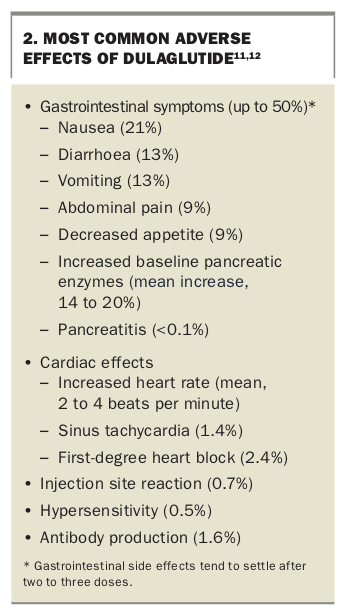
The safety profile of dulaglutide is similar to that of other long-acting GLP-1 receptor agonists in regard to gastrointestinal adverse effects, and considerably better than the profiles of the short-acting GLP-1 receptor agonists. The main adverse effects of dulaglutide are mild-to-moderate gastrointestinal effects: nausea, diarrhoea, vomiting, abdominal pain and decreased appetite (Box 2).11,12 These symptoms seem to peak in the first two weeks of treatment and rapidly improve over the next four weeks.
{kind=link}
Dulaglutide was also associated with a small mean increase in heart rate of 2 to 4 beats per minute, a 1.4% incidence of sinus tachycardia and a 2.4% incidence of first-degree heart block. A 14 to 20% mean increase in baseline pancreatic enzyme levels was seen, but this does not seem to be correlated with the development of clinically significant pancreatitis. Rats given a supratherapeutic dose of dulaglutide (more than seven times the recommended human dose) had an increased incidence of thyroid C-cell tumours.13 No similar finding has been shown in human studies.
Across four phase 2 and five phase 3 clinical trials, 1.6% of patients developed anti-drug antibodies to dulaglutide, but the effect of antibodies on efficacy is unclear; 0.5% of patients had hypersensitivity reactions, none of whom had positive antibodies.12 There was no increase in cardiovascular events for those taking dulaglutide compared with those taking other antidiabetic medications.5-10
Contraindications and precautions
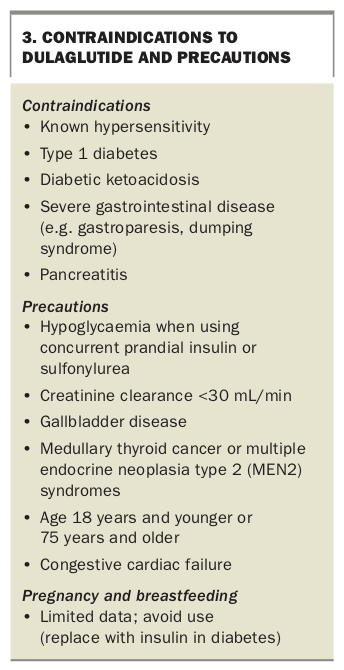
Dulaglutide is contraindicated in patients with known hypersensitivity to this drug (Box 3). It should also not be used in patients with type 1 diabetes or diabetic ketoacidosis. It should be avoided in patients with severe gastrointestinal disease (e.g. gastroparesis, dumping syndrome) and pancreatitis, and all patients should be warned of the symptoms of pancreatitis.
{kind=link}
There is an increased risk of hypoglycaemia in patients using concurrent hypoglycaemic agents (e.g. insulin or sulfonylurea), and it is prudent to consider lowering the dose of these and to increase the frequency of blood glucose monitoring. GLP-1 receptor agonists may increase the risk of gallbladder disease and the need for cholecystectomy. They should not be used in patients with a creatinine clearance less than 30mL/min. No dose adjustment is required in patients with hepatic disease.
Dulaglutide should not be used in pregnant or breastfeeding women. It is not recommended in patients with thyroid C-cell tumours such as multiple endocrine neoplasia type 2 (MEN2) syndromes.
Conclusion
Once-weekly dulaglutide is an injectable therapy for patients with type 2 diabetes who have suboptimal glycaemic control. Additional benefits include weight loss and a lower risk of hypoglycaemia than with insulin. Dulaglutide is provided in a ready-to-use pen, making it more user friendly than the other weekly GLP-1 receptor agonist on the market, but has a similar adverse effect profile. Adverse effects include nausea, vomiting and diarrhoea, which can limit its use in some patients; however, these symptoms may improve after a few doses. MT