New medications for diabetes: when to use what?

The prevalence of type 2 diabetes mellitus continues to increase and, with newer medications available, it is important to tailor therapy to the individual. We have learnt from the cardiovascular outcome trials that there are now diabetes medications that can potentially modulate cardiac and renal outcomes irrespective of their glycaemic effects.
The focus of this article is to explore the use of newer diabetes medications: sodium-glucose cotransporter-2 (SGLT-2) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists and dipeptidyl-peptidase-4 (DPP-4) inhibitors. Lifestyle optimisation with adequate exercise and healthy food choices remains a mainstay of management of diabetes and should be discussed at each appointment. Intensive weight management intervention has been shown to be effective and, in some cases, can lead to diabetes remission.1,2 Guidelines for the management of type 2 diabetes by Diabetes Australia and the Royal Australian College of General Practitioners are available online.3,4 This article contains general discussion about the TGA and PBS approvals; however, more information can be found at their respective websites.5,6
Metformin is an effective, generally well-tolerated and cost-effective first-line therapy.7 The decision regarding the preferred second- and third-line therapy must now consider more than glucose-lowering potential. The following case studies highlight different patient factors that may impact the choice of diabetes medication. Unless contraindicated, such as by renal impairment, any agent can be chosen; however, we provide a suggested class of agent and explain the rationale. Guidelines from the American Diabetes Association, the European Association for the study of Diabetes and the Living Evidence for Diabetes Consortium indicate that, where possible, use of an SGLT-2 inhibitor or a GLP-1 receptor agonist should be considered.8,9
Case 1
A 65-year-old man presents for follow up after a recent admission to hospital for a myocardial infarction, with a new diagnosis of congestive cardiac failure. He has a history of type 2 diabetes mellitus, diagnosed five years ago. His body mass index (BMI) is 27 kg/m2, and blood pressure 135/85 mmHg. In hospital, his glycated haemoglobin (HbA1c) level was 7.8% (62 mmol/mol), estimated glomerular filtration rate (eGFR) was 63 mL/min/1.73 m2 and he had an albumin-creatinine ratio (ACR) of 3.5 mg/mmol. His treatment for diabetes before hospitalisation was metformin 1 g twice daily and gliclazide modified release 60 mg mane.
What would the most appropriate next therapy be?
The guidelines suggest either a DPP-4 inhibitor, SGLT-2 inhibitor or GLP-1 receptor agonist. The preferred agent in this particular case would be an SGLT-2 inhibitor as discussed below.
Sodium-glucose cotransporter-2 inhibitors
SGLT-2 inhibitors are oral medications that increase urinary excretion of glucose by inhibiting reabsorption from the renal proximal tubules.10 In Australia, the available SGLT-2 inhibitors are empagliflozin, dapagliflozin and ertugliflozin; canagliflozin is no longer available in Australia. Of note, in addition to its glycaemic benefit, dapagliflozin is TGA-indicated for the prevention of hospitalisation for heart failure in patients with type 2 diabetes, the treatment of symptomatic heart failure and to reduce the risk of kidney function decline in patients with proteinuria. Empagliflozin is also TGA-indicated for the prevention of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease, as well as for treatment of symptomatic heart failure with reduced ejection fraction, as an adjunct to standard of care, in addition to its blood glucose-lowering effects. Dapagliflozin and empagliflozin are PBS-subsidised for the treatment of symptomatic congestive cardiac failure with a reduced left ventricular ejection fraction, in addition to standard care with a beta-blocker and either an angiotensin converting enzyme (ACE)-inhibitor or angiotensin II antagonist, with or without a neprilysin inhibitor.
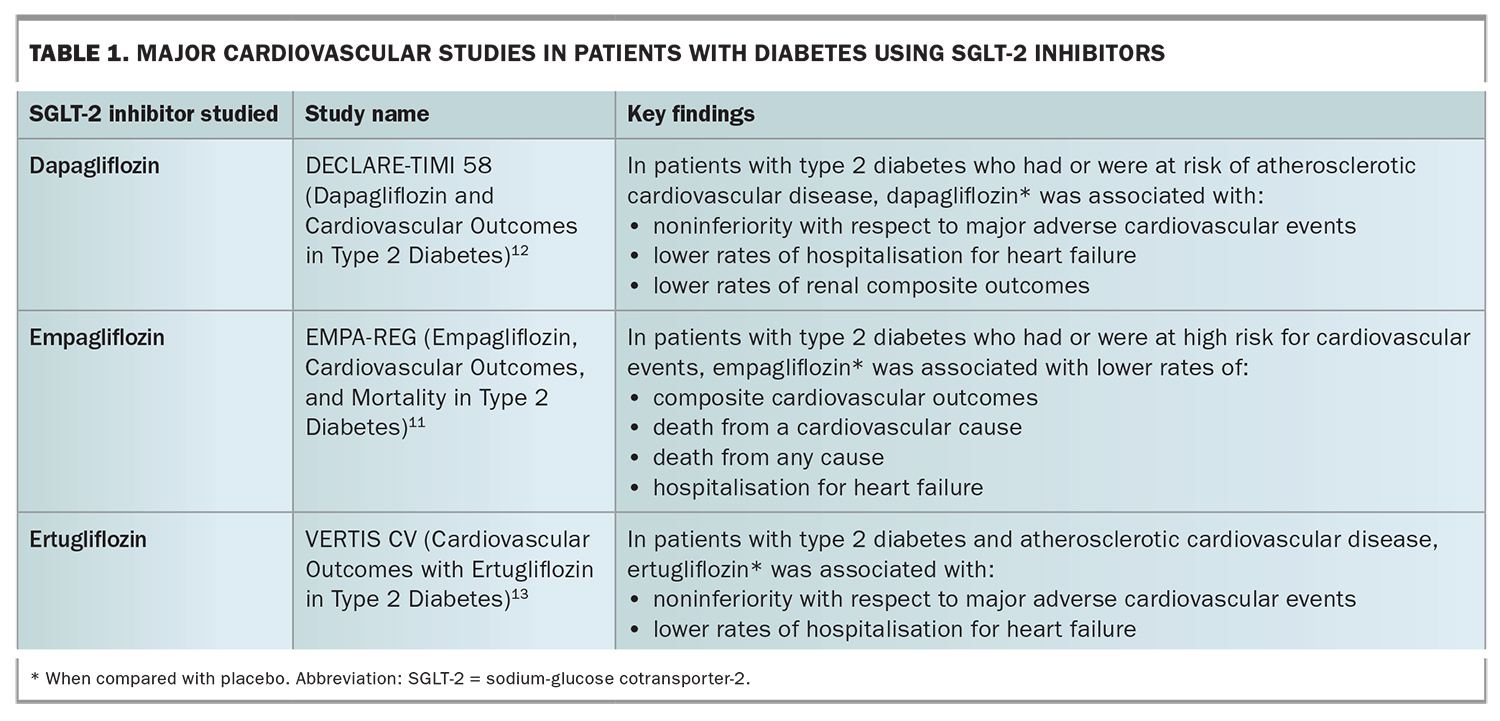
In the Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes (EMPA-REG) and Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes (DECLARE-TIMI 58) trials, the use of either empagliflozin or dapagliflozin in patients with type 2 diabetes improved composite cardiovascular and renal outcomes.11,12 In the Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes (VERTIS CV) study, the use of ertugliflozin was associated with noninferiority of cardiac events compared with placebo.13 The cardiovascular and renal benefits of dapagliflozin and empagliflozin appear to be independent of glycaemic benefit, with improved outcomes regardless of diabetes status.14-17 When reviewing data from the clinical trials, the most consistent benefit from dapagliflozin and empagliflozin appears to be in reducing hospitalisation for heart failure.11,12 In the DECLARE-TIMI 58 trial, those allocated to dapagliflozin group showed reduced hospitalisation for heart failure irrespective of a history of cardiovascular disease.12 Although not available in Australia, in the Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes (CANVAS) and Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy (CREDENCE) trials, canagliflozin was associated with a lower risk of cardiovascular events and renal disease.18,19
Table 1 outlines the major cardiovascular studies in patients with diabetes using SGLT-2 inhibitors. SGLT-2 inhibitors dapagliflozin and empagliflozin have been shown to improve cardiovascular outcomes, particularly a decrease in hospitalisation for heart failure.11,12 Therefore, in a patient with established cardiovascular disease and congestive cardiac failure, the addition of an SGLT-2 inhibitor would be an appropriate next step. A GLP-1 receptor agonist would be considered if the SGLT-2 inhibitor was contraindicated or not tolerated.
{kind=link}
The possible side effects that should be discussed include genital and urinary tract infections, because of increased urinary glucose excretion, as well as polyuria and possible postural hypotension (caused by volume depletion). Genitourinary hygiene, including in men who are not circumcised, should be discussed and adequate oral fluids encouraged where appropriate. In patients with significant congestive cardiac failure, the initiation of SGLT-2 inhibitors should be discussed with the treating cardiologist and endocrinologist as diuretic medications may need to be reduced when SGLT-2 inhibitors are introduced. An initial decrease in eGFR in the first four weeks after initiation of an SGLT-2 inhibitor may be likely. However, long-term data show stabilisation of eGFR with overall preservation of renal function.16,20
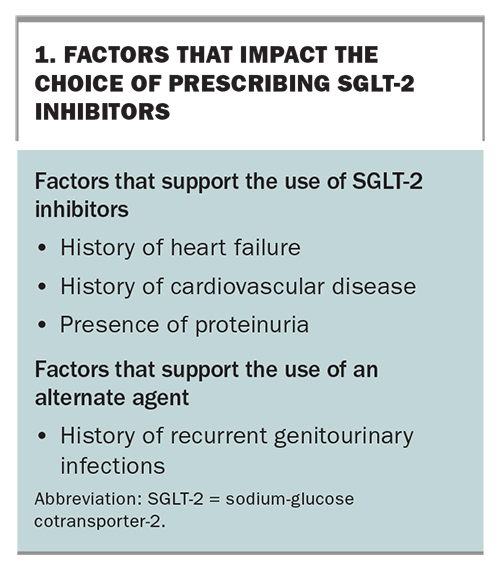
A rare but serious adverse effect of SGLT-2 inhibitors is euglycaemic ketoacidosis.21,22 Precipitating factors for SGLT-2 inhibitor-induced euglycaemic ketoacidosis are fasting states (e.g. before surgery or with low carbohydrate diets) and acute illness.23 The Australian Diabetes Society has recommended withholding SGLT-2 inhibitors in the event of acute illness, and preoperatively for two days before surgery or three days before colonoscopy (plus omiton the day of each procedure), with carbohydrate restriction, and to restart the medication when the patient is eating and drinking again.24 Rarer side effects include Fournier’s Gangrene. Box 1 outlines the factors that impact the choice of prescribing SGLT-2 inhibitors.
{kind=link}
Case 2
A 50-year-old woman presents for routine follow up. She has a seven-year history of type 2 diabetes. Other medical history includes ischaemic heart disease, for which she had coronary artery stenting two years ago, and a BMI of 32 kg/m2. Her blood pressure is 130/80 mmHg and HbA1c level is 8.2% (66 mmol/mol), with an eGFR of 68 mL/min/1.73m2 and ACR 2.7 mg/mmol. Current treatment for diabetes includes metformin 1 g twice daily and basal insulin (glargine) 20 units nocte.
What would the most appropriate next therapy be?
Again, a number of agents could be used, including intensification of the insulin regimen, or the addition of a DPP-4 inhibitor, SGLT-2 inhibitor or a GLP-1 receptor agonist. The use of a potentially cardioprotective agent should be considered.
Glucagon-like peptide-1 receptor agonists
GLP-1 receptor agonists are injectable medications that augment glucose-dependent beta cell insulin release, inhibit glucagon secretion, act centrally to reduce appetite and slow gastric emptying.25 In Australia, the available GLP-1 receptor agonists are dulaglutide, exenatide (immediate release), liraglutide and semaglutide. Lixisenatide and weekly exenatide are no longer available. Of note, liraglutide is listed under two different brand names on the TGA; one brand (Saxenda) is TGA-indicated for weight management at a higher dose, although neither of the liraglutide brands are currently PBS-subsidised.
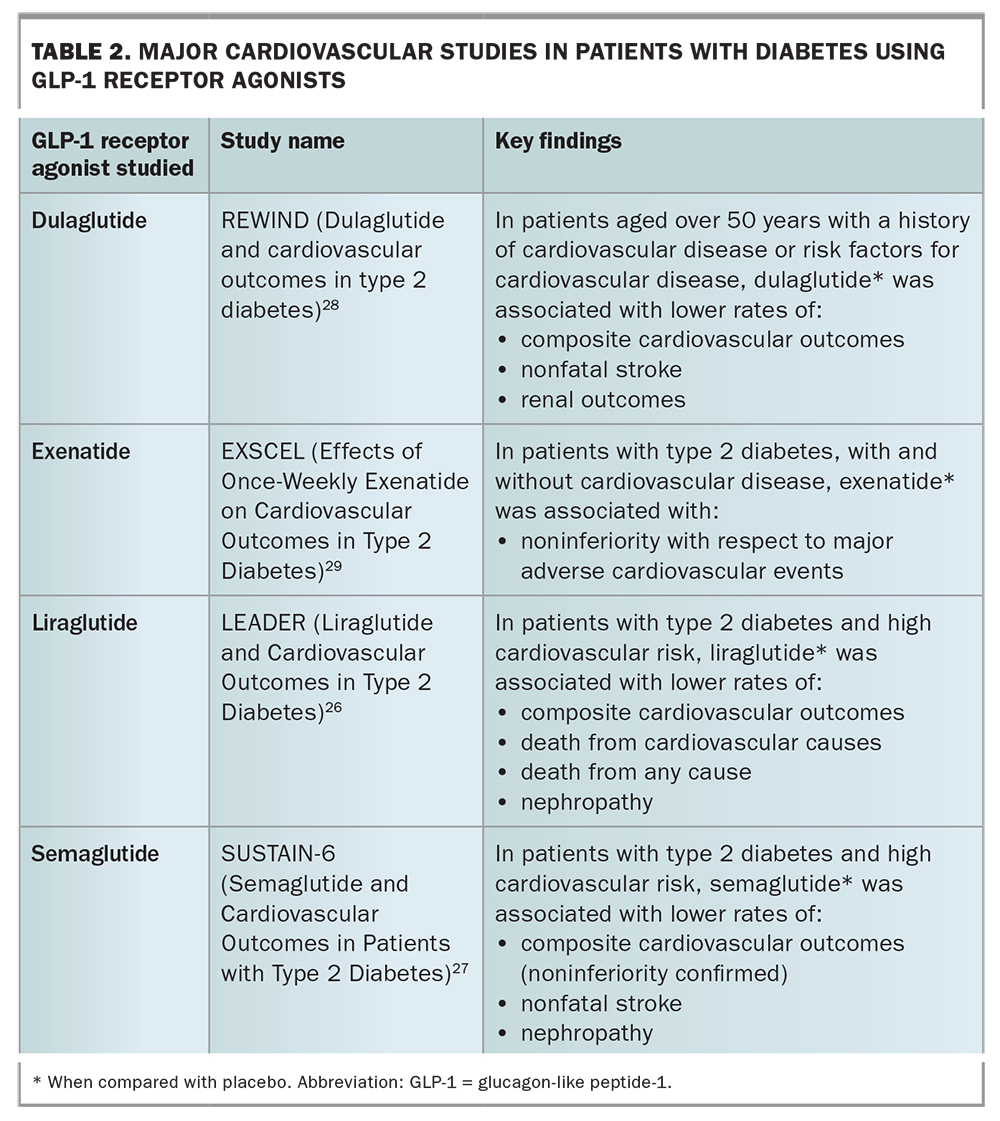
In addition to an indication for glycaemic control, dulaglutide and liraglutide (Victoza) are TGA-indicated for the reduction in risk of major adverse cardiovascular events and prevention of cardiovascular events, respectively, in patients with type 2 diabetes. GLP-1 receptor agonists are associated with weight loss.26-28 GLP-1 receptor agonists are also associated with a reduction in systolic blood pressure and a mild increase in pulse rate.26-29 In the cardiovascular outcome trials, the use of either liraglutide, semaglutide or dulaglutide was superior in reducing composite cardiovascular outcomes compared with placebo.26-28 However, there was no significant reduction in hospitalisation for heart failure, unlike with SGLT-2 inhibitors, even if meta-analyses suggest a modest beneficial effect of the class.30 The use of exenatide once weekly was associated with noninferiority versus placebo in reducing cardiovascular events.29
Therefore, in a patient who may be overweight or obese, with or without cardiovascular disease, the use of a GLP-1 receptor agonist is appropriate. An SGLT-2 inhibitor can be considered, particularly if there is a history of congestive cardiac failure. The choice of which GLP-1 receptor agonist to use should be guided by patient factors, such as a patient’s ability to learn device technique. Exenatide (immediate release) is a twice daily injection with two dose options (5 mcg and 10 mcg), with the recommendation to commence at the lower dose and up-titrate as tolerated after one month. Semaglutide is a once weekly injection and has three available doses (0.25 mg, 0.5 mg and 1 mg) with two pen devices. Dulaglutide is a weekly injection available in one dose (1.5 mg) with a unique administration device.
When starting a GLP-1 receptor agonist in a patient who is already taking insulin, there may be a reduction in the patient’s insulin requirement. We recommend frequent blood glucose monitoring and consideration of reducing insulin dose if glucose levels are not significantly elevated.
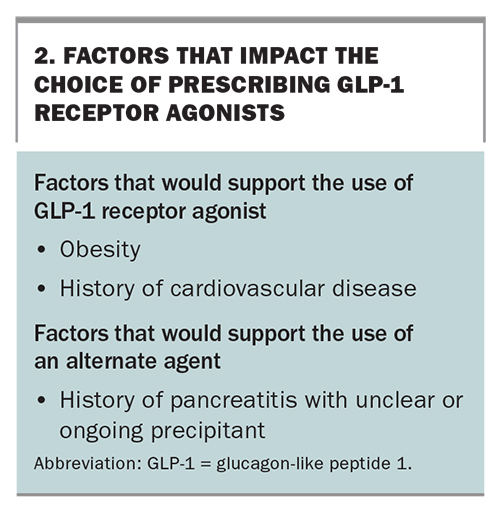
The most common side effects of GLP-1 receptor agonists are nausea, vomiting and other gastrointestinal symptoms; these are usually self-limiting. In the Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes (SUSTAIN-6) study, semaglutide was associated with an increased rate of retinopathy, which was likely due to a rapid improvement in glycaemic control in those who had underlying retinopathy.27 It is important that patients have regular retinal screening. There have been historical concerns about an association between GLP-1 receptor agonists and pancreatitis, pancreatic cancer and medullary thyroid cancer. However, large cardiovascular outcome studies have shown that the incidence rates of these events were similar to placebo and active therapy groups (Table 2). 26-29 Despite this reassuring finding, use of these medications is often avoided in the conservative management of patients with a history of pancreatitis if there is no clear precipitant. Box 2 outlines factors that impact the choice of prescribing GLP-1 receptor agonists.
{kind=link}
{kind=link}
Case 3
An 85-year-old woman presents for routine review. She has a history of type 2 diabetes, diagnosed 10 years ago, and is treated with metformin 500 mg once daily and gliclazide modified release 60 mg once daily. She has a history of hypertension, treated with perindopril 4 mg daily. She has no known history of cardiovascular disease or retinopathy. She has a BMI of 25 kg/m2 and her blood pressure is 125/80 mmHg. The most recent HbA1c level is 8.9% (74 mmol/mol), and her eGFR is 28 mL/min/1.73 m2, with an ACR of 2.7 mg/mmol.
What would the most appropriate next therapy be?
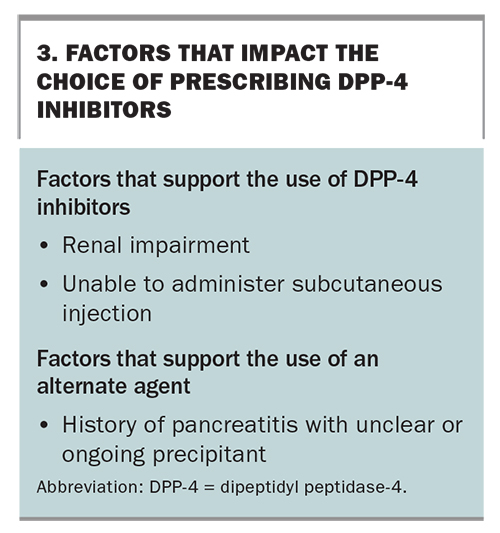
In this case, based on the patient’s renal function, age and normal weight, a DPP-4 inhibitor may be appropriate. Given her current renal function (eGFR between 15 and 30 mL/min/1.73 m2), the patient is on the maximum recommended dose of metformin, and potentially may need to stop. A sulfonylurea should be used with caution because of the risk of hypoglycaemia. Although SGLT-2 inhibitors have benefits in preventing the progression of renal impairment and proteinuria, they are contraindicated when a patient’s eGFR is below 30mL/min/1.73 m2. A DPP-4 inhibitor will improve glycaemic control with potentially limited side effects.
Dipeptidyl-peptidase-4 inhibitors
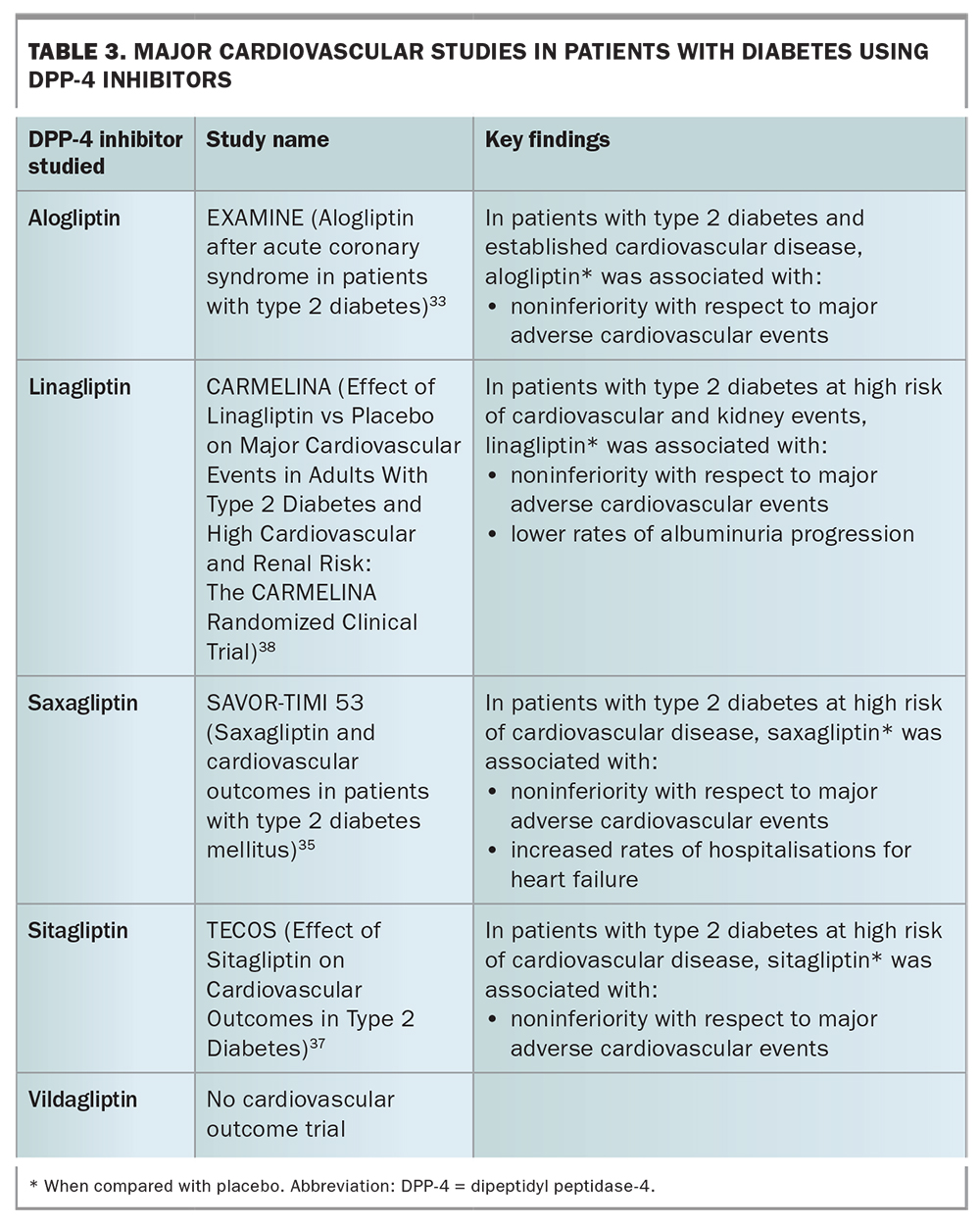
DPP-4 inhibitors are oral medications that inhibit the degradation of endogenous GLP-1.31 In Australia, the available DPP-4 inhibitors are alogliptin, linagliptin, saxagliptin, sitagliptin and vildagliptin. Linagliptin, saxagliptin and sitagliptin are PBS-funded for use with SGLT-2 inhibitors and are available as fixed combination tablets with SGLT-2 inhibitors. The glycaemic effect of DPP-4 inhibitors is modest compared with GLP-1 receptor agonists; however, the oral formulation may be preferred in certain patient groups. All DPP-4 inhibitors can be used in the setting of renal impairment. However, alogliptin, sitagliptin, saxagliptin and vildaglipitin are renally excreted and require dose reductions based on a patient’s eGFR, whereas linagliptin is hepatically cleared so does not require any dose change.32 All DPP-4 inhibitors were noninferior to placebo for composite cardiovascular outcomes in large-scale trials; however, saxagliptin was associated with an increase in hospitalisations for heart failure in high-risk patients (Table 3).33-38
{kind=link}
In general, DPP-4 inhibitors are well tolerated. As with GLP-1 receptor agonists, an association between DPP-4 inhibitors and pancreatitis has been suggested. However, when the data from each of the clinical trials were pooled, no significant effect on pancreatitis was seen.39 Results from early trials raised concerns of an association between DPP-4 inhibitors and an increased risk of infection; however, no such association was seen in the phase IV trials.35,37 Rare side effects of hypersensitivity and rash have been reported; however, there was no statistically significant difference in these events when compared with placebo.33,35,38 Factors that impact the choice of prescribing a DPP-4 inhibitor are outlined in Box 3.
{kind=link}
Conclusion
The cases presented show how patient factors affect the choice of medication for type 2 diabetes. In each case, a specific medication class is preferred; however, an alternative therapy could be prescribed and varying patient factors may tip the balance between the preferred option. For example, in Case 1, a patient history of recurrent genitourinary infections would support the use of an alternative therapy, such as a GLP-1 receptor agonist. However, the benefits of lower rates of hospitalisation for heart failure support the use of an SGLT-2 inhibitor over a GLP-1 receptor agonist. The patient may also have a preference for a noninjectable agent. Each type of medication should be considered and a patient-centred approach taken.
An increasing range of treatment options for type 2 diabetes are available and the decision on which medication to prescribe must take into account individual patient factors. A review of the patient’s comorbidities should guide the appropriate therapy and patient preference should be taken into account after discussion of possible side effects. Important factors for consideration are outlined in the Practice Points. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.