More than just reflux – The era of eosinophilic oesophagitis

Food Allergy
Oesophagus disorders
The incidence of eosinophilic oesophagitis (EoE) is increasing in concert with other forms of food allergy. It is helpful to consider EoE as a cause of food bolus obstruction and dysphagia, particularly in young adults.
Remember
- Eosinophilic oesophagitis (EoE) is a unique form of nonimmunoglobulin E (IgE) mediated food allergy. More than 90% of patients will respond to an elemental diet, although this is an impractical treatment for most patients.1
- Adults with EoE typically present with food bolus impaction and/or dysphagia to solid foods.
- Children can have a more varied presentation, such as heartburn, failure to thrive, persistent vomiting or chronic abdominal pain.
- Allergy tests have no role in determining dietary triggers, and do not form part of routine management.1,2
- First-line management options include proton pump inhibitors (PPIs; off-label use), topical corticosteroids (e.g. swallowed budesonide slurry; off-label use) or dietary management.
- Response to PPIs and resolution of eosinophilia will occur in many patients with EoE and does not signify a need to relabel the diagnosis as gastro-oesophageal reflux disease (GORD).
Background
- EoE is a chronic inflammatory condition characterised by an eosinophil-rich infiltrate in the oesophagus, which results is oesophageal oedema, narrowing and stenosis, with clinical sequelae of dysphagia and food bolus impaction.
- First characterised in 1993, the incidence of EoE is increasing (independent of increased diagnostic awareness and endoscopy) in concert with other forms of food allergy and is a leading cause of food bolus impaction in adults.
- EoE affects mainly Caucasian males, with a male-to-female ratio of about three to one.
Assessment
- Think of EoE in patients with dysphagia, a history of food bolus impaction (either aborted or with emergency attendance and endoscopic removal) or with heartburn or dyspepsia.
- Younger children may present with chronic abdominal pain, vomiting, failure to gain weight, poor oral intake or dietary regression (no longer taking food they would previously have eaten). EoE may be misdiagnosed as GORD in children who are fussy eaters.
- Many patients with EoE are atopic. Coexistent asthma, rhinitis, food allergies or atopic dermatitis should heighten suspicion of this diagnosis.
- Currently, the only way to diagnose and monitor EoE is by endoscopy with biopsies of the upper and lower oesophagus. A level of more than 15 eosinophils per high-power field (HPF) on histopathological assessment is required to make the diagnosis (the oesophagus is usually devoid of eosinophils).
- EoE is a unique form of food allergy, and most patients will respond to elimination diets. Allergy tests are not predictive of food triggers. Therefore, although assessment of comorbid atopic conditions by an allergist is advised (when present), typical tests for IgE-mediated food allergy such as skin prick tests and serum food-specific IgE level are not useful.
Management
Overview
- Many patients with EoE will respond to more than one treatment. Finding the treatment that is both able to achieve histological remission (less than five eosinophils per HPF) and is well tolerated is the challenge.
- All changes to treatment require follow up with an endoscopy and biopsy to determine efficacy of the intervention (Flowchart).
Reason to treat
- Food bolus impactions are inconvenient, frightening and dangerous.3 Complications related to food bolus impaction include pain, aspiration of gastric contents at time of emergency endoscopy and (rarely) perforation (spontaneous or at time of endoscopy).
- In young children, failure to thrive secondary to EoE requires treatment given the obvious deleterious consequences for growth and development.
- Failure to treat may lead to a fibrostenotic phenotype, characterised clinically by recurrent food bolus impaction and/or the need for dilatation.
Methods of treatment
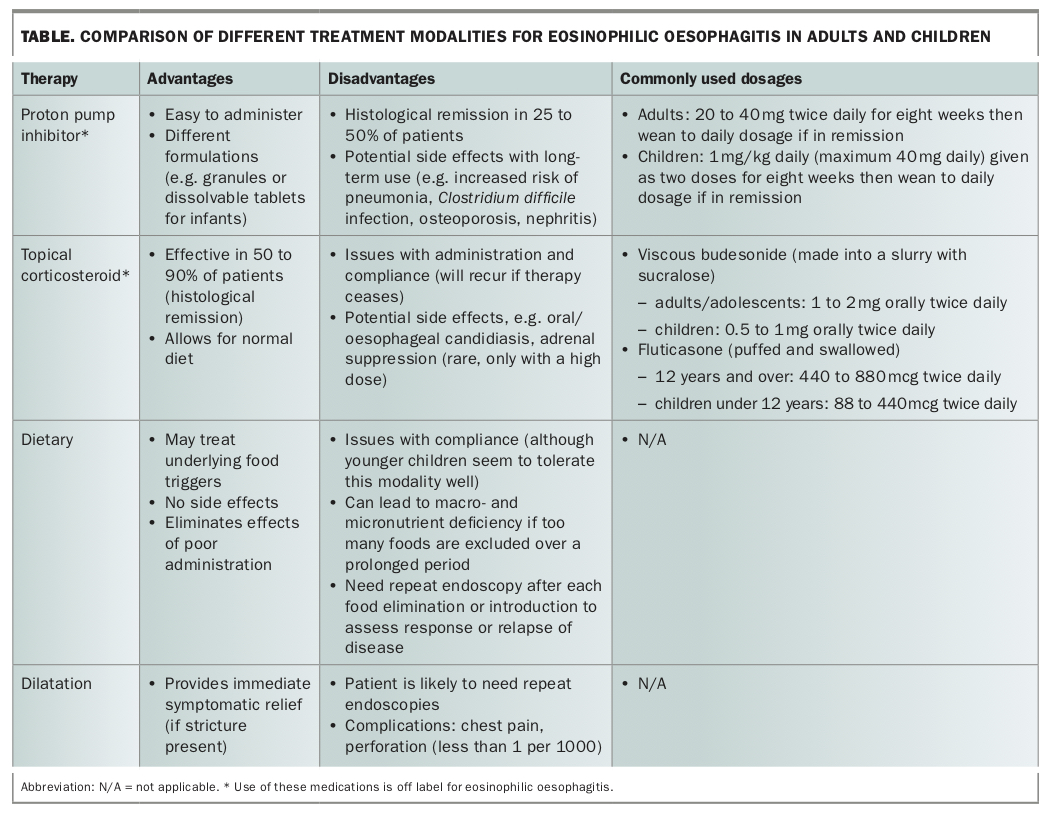
Five options are available for the treatment of EoE: all are valid acutely, but the specific choice may depend on severity of clinical presentation and patient preference following discussion (Table). Although patients may become asymptomatic with treatment, histological examination may show ongoing disease activity, making treatment compliance an ongoing challenge in management of EoE.
{kind=link}
Proton pump inhibitors (off-label use)
- Endoscopic and histological remission is achieved in 25 to 50% of patients. PPIs possibly work by decreasing acid exposure in the lower oesophagus, therefore restoring barrier integrity and decreasing food antigen contact with the gastrointestinal immune compartment.
- Start with a high-dose PPI and decrease to daily treatment (Table). A decrease to daily treatment (dose reduction or step-down) will lead to continued remission in 85% of patients.4
- Long-term data are lacking.
Topical corticosteroids (off-label use)
- Most clinical trials conducted internationally used budesonide (as a viscous gel that is swallowed). In Australia, dry powder fluticasone was used initially, and although viscous budesonide is the first choice in adults due to better tolerability, both budesonide and fluticasone are still used in children. In addition, a newer topical corticosteroid therapy – ciclesonide – may be used in some children not responding to budesonide or fluticasone (although evidence is based on case series at this stage).
- Topical corticosteroid treatment for EoE can be effective but EoE will almost certainly recur if therapy is stopped. Endoscopic and histological remission is achieved in 50 to 90% of patients. Common doses of topical corticosteroids are listed in the Table. Low-dose or alternate daily dosing has not been associated with a durable response.
- The method of administration of topical corticosteroids is important to provide maximal effect through direct contact with oesophageal mucosa. Viscous budesonide needs to be made in to a slurry with sucralose (artificial sweetener) and swallowed. Fluticasone and ciclesonide should be puffed and swallowed, not inhaled, so spacers should not be used. As distinct from their use in asthma, the mouth should not be rinsed and the patient should not eat or drink for 30 minutes after administration.
- The safety of topical corticosteroids is unknown but a recent meta-analysis of all studies suggests that the risk of side effects is small.5 Side effects include oral candidiasis and potential adrenal suppression with higher doses. If topical corticosteroids are already being used for rhinitis, asthma or dermatitis an alternative treatment for EoE should be considered given that the corticosteroid dose will be higher and may cause adrenal suppression.
- Long-term data are lacking.
Dietary therapy
- Dietary therapy is theoretically appealing in that it involves treating the underlying cause (since EoE is a unique form of food allergy). The difficulty is that no allergy tests can predict the food triggers. Dietary therapy can be used in two settings:
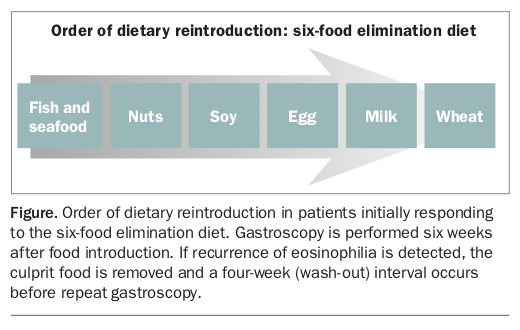
— Food elimination diet (FED): remove a set number of presumed ‘culprit foods’. These are based on known food triggers from previous studies. We recommend the ‘3FED’ (gluten, dairy, eggs) based on our Australian experience in adults. A ‘2FED’ (dairy, wheat) up to a ‘6FED’ (dairy, wheat, egg, soy, tree-nuts, fish) may be required in many children. Highly motivated patients who are prepared to undergo multiple endoscopies and adhere strictly to the diet would be suitable for this regimen. For example, in the 3FED, gluten, dairy and eggs are avoided initially. After six weeks a repeat endoscopy is performed to determine if resolution of EoE occurs. If so, the least likely food trigger is reintroduced and, again, after six weeks an endoscopy is performed (Figure). Long-term maintenance data are lacking.
{kind=link}
— Elemental diet: liquid nutrition. About 90% of individuals will respond. This diet is generally reserved for children who are unwell due to dysphagia (e.g. failure to thrive) or children who are already on enteral feeds (e.g. poor swallow and aspiration risk in cerebral palsy).
Oesophageal dilatation
- Oesophageal dilatation is a safe procedure that can ameliorate dysphagia immediately and may provide relief for between six to 18 months. This can be performed in patients with a demonstrable stenosis (stricture; Table).
- Dilatation does not address the underlying inflammation that is responsible for EoE and should be viewed as a means of providing rapid symptom relief and to complement other therapies. In individuals who fail to respond to other therapies, dilatation can be used in a standalone capacity.
Combination therapy
- Patients who fail to respond to a single medical therapy may benefit from combination therapy, although randomised controlled trials have not been performed to support this management approach. PPIs in particular, that are simple to administer and may treat coexistent GORD, are often advocated in combination with the elimination diet.
Conclusion
EoE is a unique form of food allergy presenting as dysphagia and food bolus impaction in adults and adolescents, with an array of additional symptoms in children, ranging from chronic abdominal pain to failure to thrive. Diagnosis requires endoscopy and biopsy showing more than 15 eosinophils per HPF. Allergy tests do not form part of routine management. Reasonable first-line treatment options include PPIs, topical corticosteroids, dietary therapy or oesophageal dilatation. Maintenance treatment is thought to be required in most patients to prevent stricture formation, food bolus impaction events and (in children) failure to thrive. MT