The risks and benefits of PPIs. Are they safe?

Oesophagus disorders
Digestive diseases
In recent years, barely a week goes by without another report linking use of proton pump inhibitors with adverse health outcomes, yet they remain among the most used classes of drugs worldwide. What is the story? Are they safe or not, and who should take them?
Remember
The effectiveness of proton pump inhibitors (PPIs) – esomeprazole, lansoprazole, omeprazole, pantoprazole and rabeprazole – for specific indications has been established over many years, with many evidence-based guidelines available. The most common indication is for suspected or proven gastro-oesophageal reflux disease (GORD).1
Indications for PPIs
- Proven benefit (and superiority over alternatives) is established for the following conditions.
Erosive oesophagitis
- This can only be diagnosed at endoscopy as the severity of reflux symptoms does not reliably differentiate erosive from nonerosive reflux disease (NERD).
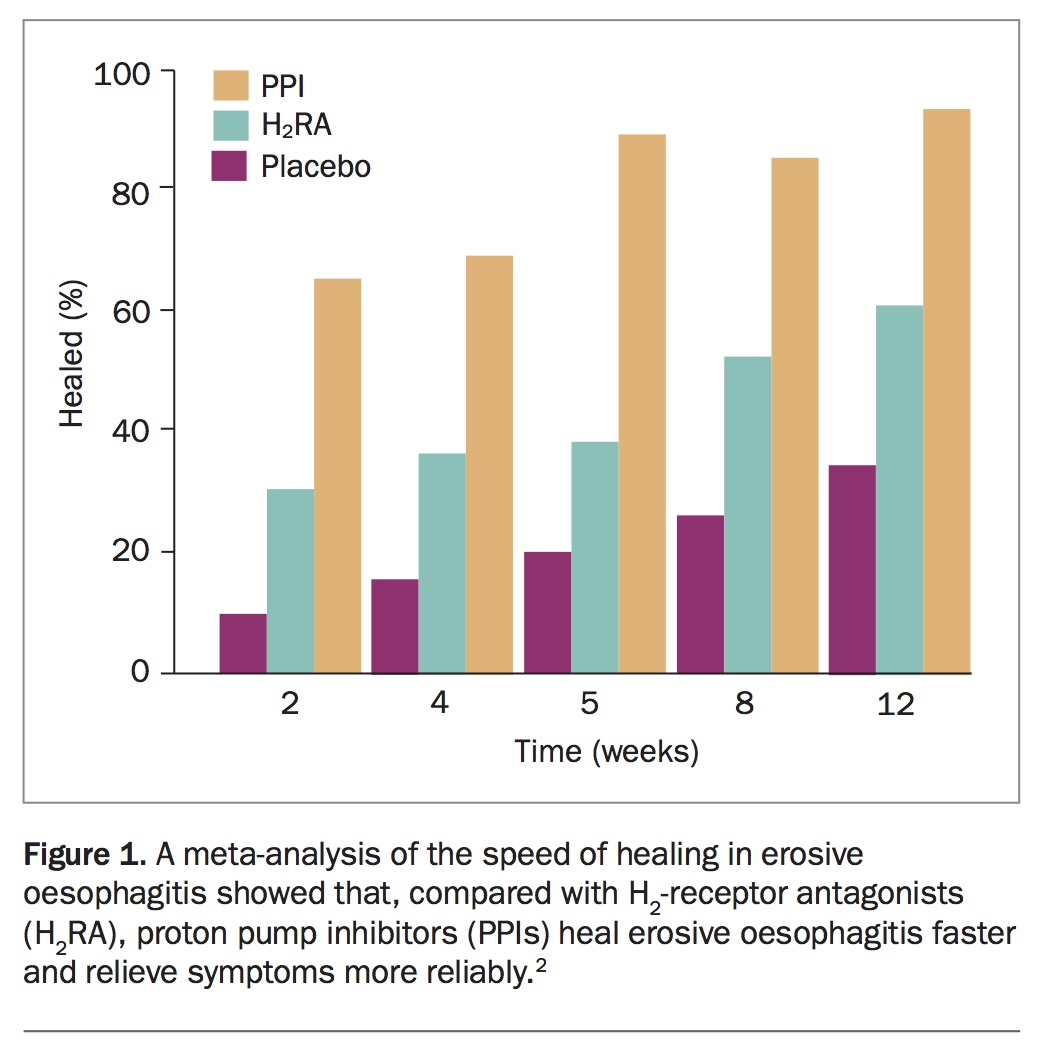
- Compared with H2-receptor antagonists, PPIs heal erosive oesophagitis and relieve symptoms of all grades of severity more often and more quickly.2 The most benefit is seen with more severe oesophagitis, which comprises a minority of all patients with reflux disease. Such patients are more likely to need long-term continuous treatment. The use of PPIs in these patients has seen the occurrence of peptic oesophageal strictures fall markedly (Figure 1).2
{kind=link}
Nonerosive reflux disease
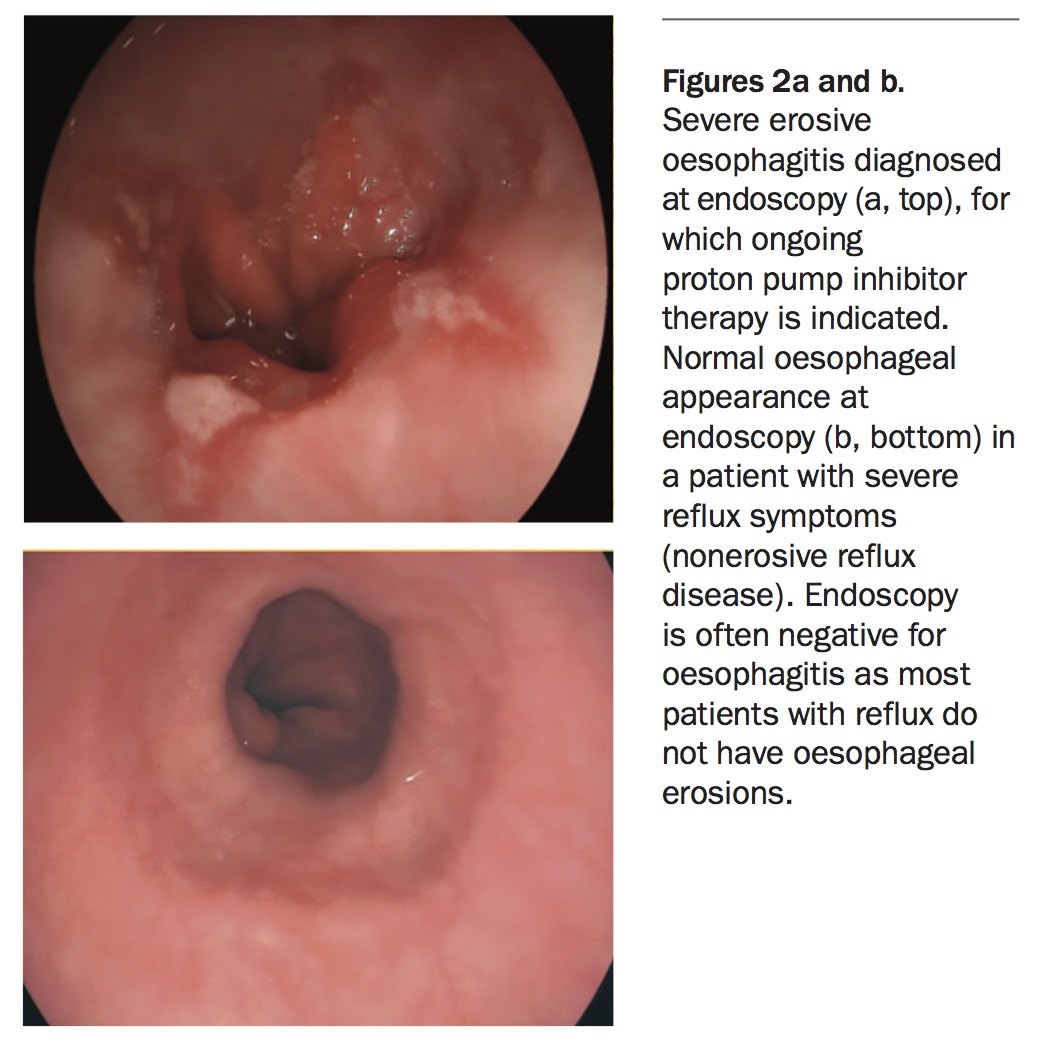
- Two-thirds of patients presenting to GPs with troublesome reflux symptoms would not have erosions seen on endoscopy if it were performed. Although the distinction between erosive and nonerosive disease cannot be made clinically, PPIs are often prescribed appropriately without endoscopy, with recourse to endoscopy if symptoms are severe, frequently relapse, atypical or nonresponsive to therapy, or when there are risk factors for or concerns about other possible diagnoses. When it is performed, endoscopy does not diagnose NERD but does exclude other problems (Figures 2a and b).
- PPIs control symptoms in NERD and uninvestigated reflux symptoms reasonably well and are superior to H2-receptor antagonists (although these drugs, along with alginates and antacids, still have a role). As this is a clinical diagnosis, it includes a heterogeneous group of patients with reflux-like symptoms that may be caused by something other than acid reflux (such as functional heartburn), who do not respond to a trial of PPI therapy, as well as those with acid reflux who do respond. Doubling the dose of PPIs is sometimes tried but has a low rate of success. Deprescribing PPIs that have not been effective, pursuing other strategies or referring the patient for investigations are often better options.1
{kind=link}
Peptic ulcer healing
- PPIs heal gastric and duodenal ulcers caused by Helicobacter pylori infection, NSAIDs or aspirin. However, PPI use is not a substitute for definitive therapy addressing the cause of the peptic ulcer disease.
Helicobacter pylori
- PPIs are a key component of both first- and second-line H. pylori eradication therapy using triple and quadruple combinations, improving eradication outcomes compared with antibiotics alone.3 PPI monotherapy does not eradicate H. pylori but does cause frequent false-negative biopsy and breath test results when these are performed for H. pylori diagnosis and for assessment of outcome after therapy.4 PPIs should be withheld for one week, and preferably two weeks, before testing.
- Long-term PPI use in patients with ongoing H. pylori infection may increase the rate at which H. pylori causes precancerous histological changes in the stomach (intestinal metaplasia and mucosal atrophy). It is therefore reasonable to test for and treat H. pylori infection before commencing long-term PPI therapy, especially in younger patients.5
Ulcer and bleeding prophylaxis
- PPIs reduce the risk of peptic ulcers in patients prescribed NSAIDs (primary prophylaxis) and reduce the risk of relapse if NSAIDs must be continued after ulceration has occurred (secondary prophylaxis). Therefore, PPI coprescription is indicated for patients at higher risk of ulcers caused by NSAIDs. This includes older patients with comorbidities, particularly if there is concomitant use of antiplatelet agents or anticoagulants, smoking or a history of ulcer or bleeding.3,6 PPIs also reduce the risk of bleeding with low-dose aspirin use, but as this overall risk is lower than that for NSAIDs, PPIs are usually only coprescribed to those at significantly higher risk of ulcer or bleeding.7
Acute bleeding
- PPI infusions are used in hospital after endoscopic therapy to control upper gastrointestinal bleeding. This reduces the rate of rebleeding by enhancing stability of clot formation.
Eosinophilic oesophagitis
- This condition may be underrecognised in adults. It should be suspected in patients with intermittent dysphagia and reflux-like symptoms, particularly in the context of a history of allergy. Diagnosis requires endoscopy with oesophageal biopsies (raised mucosal eosinophil count). Treatment is usually with swallowed (not inhaled), poorly absorbed corticosteroids, such as budesonide or fluticasone. A subset of patients with eosinophilic oesophagitis respond to the addition of PPIs, and both drugs are usually given at least initially. PPI monotherapy is not sufficient.
Inappropriate use of PPIs
- PPIs are frequently prescribed for indications for which there is little evidence of efficacy or are continued when no benefit is apparent.8 PPIs are no better than placebo for functional dyspepsia and nonspecific gut symptoms. Although they are often tried for treating such symptoms (as some of these patients may have reflux), they should not be continued in the long term when there is no response. Similarly, long-term empirical use for nonspecific cough or throat symptoms, in the absence of reflux symptoms, is usually unhelpful.
- Short-term PPI treatment is frequently prescribed to hospitalised patients; PPIs should not be continued long term on discharge without a clear and valid indication. Low-risk NSAID users do not routinely require PPI prophylaxis. The indication for ongoing therapy should be reviewed periodically.
Assessment
- In most cases, PPIs are prescribed empirically; a clear clinical provisional diagnosis should be made. When endoscopy is indicated, PPI use is guided by its findings.
- For patients with reflux, PPI therapy has two phases and should be tailored to the individual. The first phase is a trial of therapy to relieve symptoms, often for up to eight weeks. The second phase is to determine the role and mode of longer-term use. Response to a treatment trial will direct whether the treatment is continued, modified or ceased and if other investigations are needed. When symptoms are relieved, a trial off therapy guides the need for continuous therapy. Patients who relapse infrequently may be satisfied with intermittent self-directed therapy (on-demand therapy).1
Management
- All PPIs are similar, with only minor pharmacological differences. For most patients with reflux, PPIs are most effective when taken about 30 minutes before breakfast. When long-term PPI therapy is ceased, it may be best to taper treatment over a week or two rather than stopping abruptly, to avoid the possibility of transient ‘rebound’ symptoms (that may lead to resumption of therapy).
The possible risks of PPI therapy
- Many recent publications have reported an association between PPI use and an increased risk of a dazzling array of adverse outcomes. Reports of an increased risk of osteoporosis, myocardial infarction, renal disease, stroke, dementia, pneumonia, liver disease, stomach cancer and death have caused alarm among doctors and patients alike. Unfortunately, these reports are often accepted uncritically, with any proper scientific scrutiny being much less well publicised.
- Such studies are mostly retrospective analyses of mismatched heterogeneous cohorts or patient prescription databases that were never designed to address the specific issue. These methods are subject to major confounding. Although they may raise hypotheses, they do not prove them. Importantly, the magnitude of the risks claimed is low. Odds ratios of risk in these studies were usually less than two (which is unlikely to provide a meaningful signal of risk in such studies) and often disappear when better matching is done.9-16
- A feature of these studies is that PPIs were used more often in more morbid patients. That is, PPI use was a surrogate for morbidity rather than the cause of it. One example that highlights this confounding is a report linking PPIs to renal disease.17 The patients treated with PPIs had significantly lower glomerular filtration rates and higher body mass indexes (BMIs); patients with GORD often have higher BMIs. They also had significantly more pretreatment comorbidity related to kidney disease, including hypertension and cardiovascular disease, and greater use of other drugs, indicating their higher pre-existing risk of renal disease.12 Similar problems have been found in studies linking PPIs to myocardial infarction.9-11
- The claim regarding an increased risk of dementia was derived from a health insurance claims database, which was never intended or able to address this question.18 The study was highly confounded, as older age, depression, heart disease, stroke and polypharmacy were all more common before treatment in patients using PPIs. It did not control for diet, smoking or obesity. The study authors reported a minimally increased odds ratio. The report was thoroughly refuted.14-16 The authors conceded that highly correlated variables biased the results, that the association was weak and that they had not proven that PPIs cause dementia. The study was widely reported, but the rebuttals were not.
- Similarly, the osteoporosis scare has been strongly rebutted and the flaws in the data have been highlighted.9-11,19,20 There is no recommendation to avoid appropriate PPI use in patients at risk of osteoporosis.
- The possibility of a link between PPIs and gastric cancer is highly confounded, as PPIs are used in patients as part of H. pylori treatment and frequently in patients with upper gut symptoms, who may have undetected precancerous gastric mucosal changes. Eradication of H. pylori does not abolish symptoms in many patients, leading to ongoing (often futile) PPI use. Eradication reduces but does not abolish gastric cancer risk if atrophy and intestinal metaplasia are already present. As noted above, PPI use in a patient with an infected stomach may hasten the development of these changes, such that H. pylori eradication before PPI use should be considered. Lastly, cancer of the gastric cardia and gastro-oesophageal junction is an occasional sequela of reflux, for which PPIs are often used.
Established adverse effects of PPI
- There are several established risks of PPI therapy. There is about a one in 10,000 risk of interstitial nephritis and rare reports of hypomagnesaemia.9-11 Theoretical risks of iron or vitamin B12 malabsorption appear minor.
- A modestly increased risk of bacterial diarrhoea (with Salmonella and Campylobacter species) has been reported, especially in travellers. An association between PPI use and greater risk of Clostridium difficile infection is confounded by the comorbidity of the patients studied, but there may be a small, although not yet proven, increase. PPIs may cause changes in the gut microbiome but the consequences of this, if any, are far from clear. A slightly increased risk of microscopic colitis has been noted and may relate to this.9-11
- Lastly, there is a potential risk of competitive inhibition of clopidogrel in patients with cardiovascular disease, which has not been confirmed in the one controlled trial undertaken to date.9-11 If real, the risk is very small and circumvented by the use of other antiplatelet agents (i.e. ticagrelor, prasugrel or aspirin).
Responding to patient concerns
- Lay and medical press can misinterpret association studies, and sensational headlines lead to public anxiety and sometimes inappropriate cessation of therapy. The resultant confusion between an association of a drug with an outcome and causation has negatively influenced the perception of the safety of PPIs despite the weak, inconclusive and negative evidence. Balanced expert reviewers and editorialists are tackling this problem and defining
standards to separate association from causation, but such efforts garner fewer headlines.9-11 - GPs need to have a considered, caring and nondismissive way of responding to patient concerns that are increasingly being raised. There is a need to explain, in lay terms, the difference between an association and causation and the flaws in these reports, perhaps using simple analogies.
Conclusion
PPIs may be considered a safe and useful class of drugs when used for appropriate indications. As with all drugs, there are established risks that must be balanced against the benefits of therapy, and ongoing pharmacovigilance is required. However, the recent spate of claims of adverse outcomes have been based on unconvincing data. Explaining to patients the difference between an association and cause and effect may be helpful. As with all drug use, the lowest effective dose should be prescribed for the shortest time required, and the indications for use should be periodically reviewed. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.