Obesity in primary care. 10 practical ways to help your patients lose weight


Obesity
Weight control
Obesity is a growing health problem around the world, due to systemic and individual reasons. Most countries have developed guidelines to deal with the individual causes of obesity, but these have had limited impact on the population prevalence of obesity. Primary care is an important avenue to influence the individual determinants of obesity. In this article, the authors draw on their long-term experiences to suggest 10 practical recommendations for managing weight loss in primary care.
- Obesity is now recognised as a chronic disease that continues to increase in prevalence in most countries.
- Although obesity is largely a systemic problem, with roots in politics, economics, society etc, primary care is an important avenue for clinical treatment.
- Most countries have developed guidelines for weight-loss management but, unlike many infectious disease treatments, there is no single mode of treatment.
- Despite large differences in managing weight loss in individuals, there are practical ways (additional to clinical guidelines) that can help GPs manage weight loss in primary care.
Picture credit: © World Obesity Model used for illustrative purposes only
Obesity remains, stubbornly, a major modern health problem.1 Efforts to reduce it at both the population health and clinical levels have had little impact to date.2 Although many individuals have had success in losing weight through various means, the standard diverse, multimodal treatment models for clinical practice are only marginally successful.3 Our experience indicates that, not surprisingly, many clinicians who have tried to develop a special understanding in the field have withdrawn in frustration. However, as stated in a recent review of the role of primary care in obesity: ‘…. given the influence and reach of primary care providers, we cannot afford for them to be sidelined in the treatment of obesity in larger populations.’4
There are several reasons for the lack of success in obesity management. Humans and other mammals have a genetic predisposition to gain excess fat under appropriate circumstances to help them survive the ‘feast and famine’ cycles of history. This has led to the selection of genes for energy storage, making weight gain the preferred process and weight loss a detrimental outcome.
Changes in the modern environment mean that genetic predispositions are reinforced by environmental abundances e.g. energy-dense foods and effort-saving machinery. Obesity becomes a normal reaction to an abnormal environment, rather than an abnormal reaction to a normal environment.5 It has even been suggested that ‘…obesity is merely collateral damage in the battle for modernity.’6
Also, the variable interaction of genetics and environment guarantees a wide range of outcomes from any group of people on any single treatment program.7 This disparity in outcomes is far greater than the individual variation expected from most drug therapies, exacerbating clinical fatigue in managing the problem.
Obesity treatment guidelines provide a well-defined, if evolving, clinical model for treatment.3 Before triaging through such processes as the Edmonton Clinical Staging System8 to more intensive psychological, pharmaceutical and/or surgical procedures, it’s reasonable to ask if there are any experience-based practices, outside of formal government guidelines, that can help clinicians assist patients with weight loss.
Here, we provide practical recommendations for managing weight loss in primary care. These add value to, rather than replace, the standard guidelines for obesity management.9 They are discussed after a brief reconsideration of the rationale for weight loss and come from our combined 60 years’ experience of working at the clinical, epidemiological, research and academic levels in the area, plus a rating from health professionals at the recent conference of the Australasian Society of Lifestyle Medicine.10 Although the recommendations are targeted at clinical practice, specifically medical practitioners, it should be noted that neither author of this article is medical.
Rationale for weight loss
Although obesity is associated with several chronic diseases, the exact nature of this relationship remains unclear.1,11 In most cases, a molecular basis (i.e. ‘cause’) remains elusive, hence the more correct use of the term ‘determinants’ instead of ‘causes’. Recently a form of low-grade, systemic inflammation (‘metaflammation’),12,13 which can lead to dysbiosis and allostasis with or without obesity,11 has been found to be present in most forms of adiposity-based chronic diseases (ABCD).14 There are suggestions that obesity may thus be an element within a larger milieu of problems in society, rather than the unequivocal cause of all ill-health associated with ABCD.6
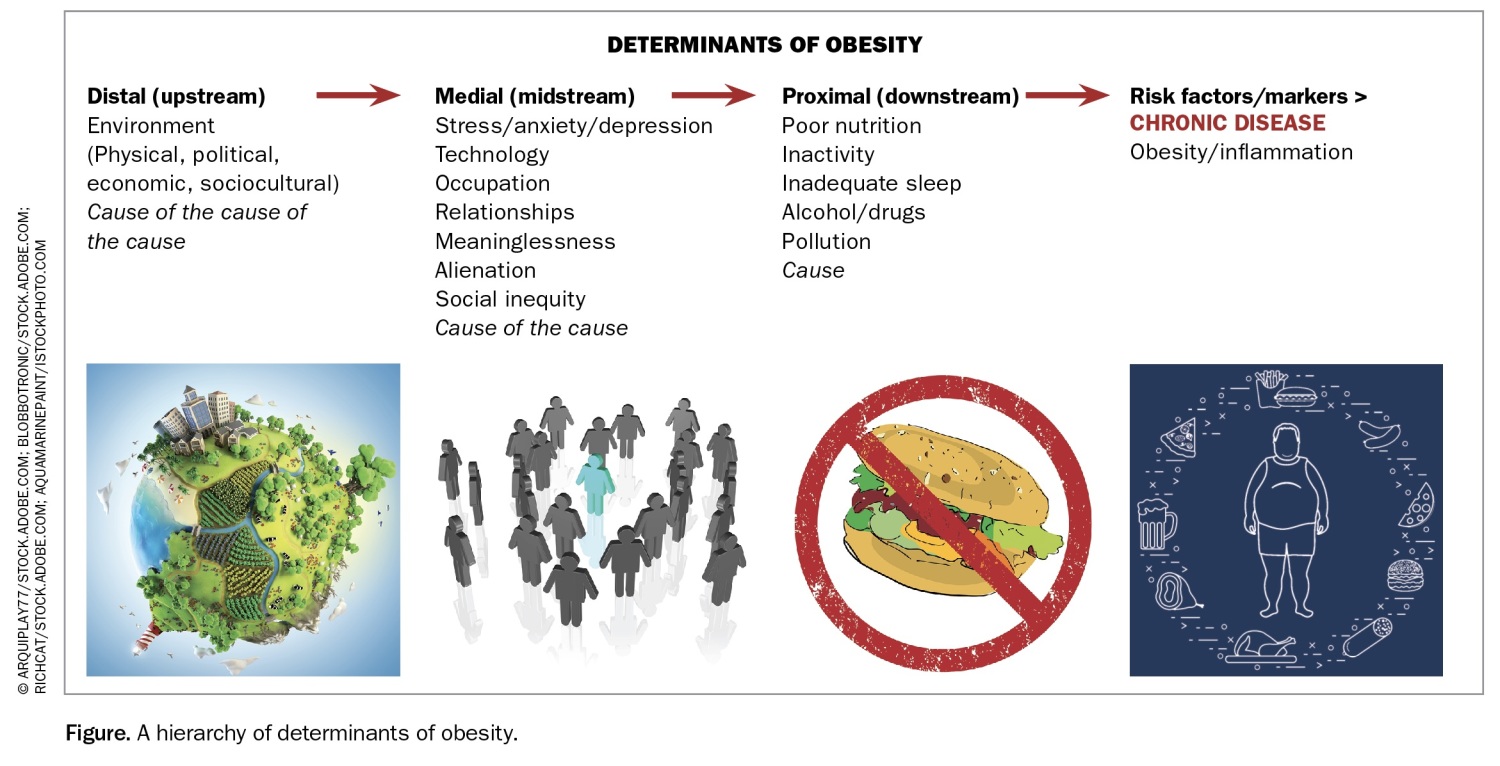
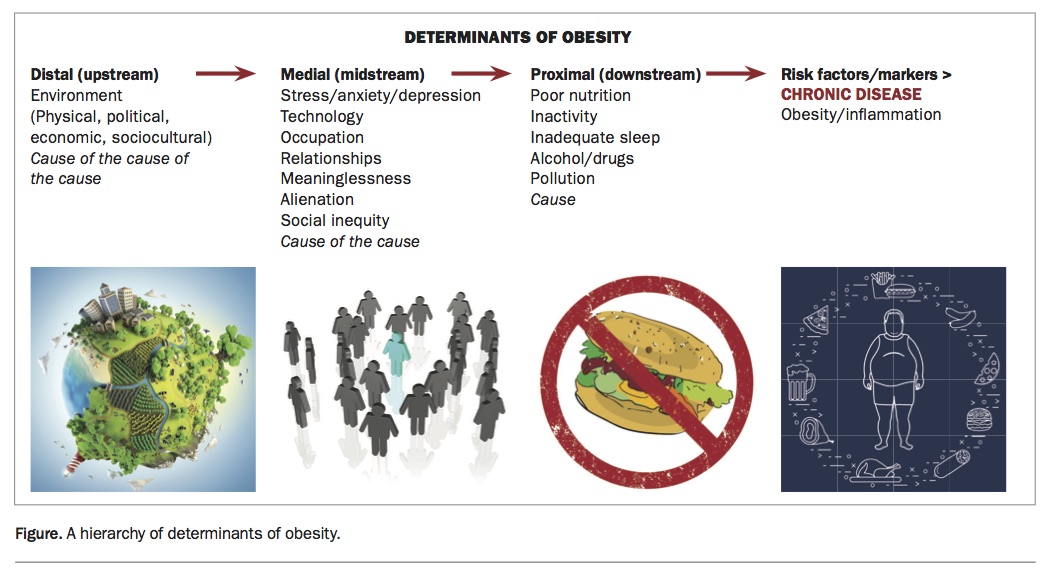
It has been demonstrated that certain energy-related behaviours such as poor or over-nutrition, inactivity, lack of sleep and stress – which are known determinants of metaflammation, as well as obesity – can lead directly to chronic diseases independent of obesity.15,16 The implications are that, although treating obesity should decrease the risk of many adiposity-related conditions (such as diabetes, obstructive sleep apnoea, hypertension and heart disease), effective prevention and management of chronic disease still requires attention to the full range of lifestyle and environmental factors that are determinants of chronic disease – with or without obesity (Figure).17 To address the problem it is important to deal not only with the proximal, or immediate, causes of ill-health, but also with more medial and distal causes (i.e. the ‘cause of the cause’ and the ‘cause of the cause of the cause’).18
{kind=link}
Given the need to address the range of lifestyle and environmental factors that determine obesity, the following 10 suggestions are proposed for clinicians to approach weight management in primary care. Due to space limitations, these have not been extensively elaborated. They are intended for consideration for further discussion.
1. Encourage reduced energy intake volume
Despite various theories and claims for the weight-loss benefits of a range of different diets, exercise programs, techniques, tools, etc., there is no evidence that weight loss can occur without a negative energy balance (where energy expenditure exceeds energy intake). There may be individual differences in nutrient storage capacities and energy costs of metabolic processes but, in general, total energy intake can be explained in terms of the total ‘volume’ of food and drink (Box 1).
{kind=link}
2. Advocate increased energy expenditure volume
As with energy intake above, there are no substantive data to support different forms of physical activity in weight loss, over and above that provided through an increase in total energy ‘volume’.
Some forms of activity may be more efficient than others in expending energy, such as excess post-exercise oxygen consumption (EPOC) or ‘afterburn’ – this is strenuous activity that leads to a measurably increased rate of oxygen consumption after the activity and sustained calorie burning.19
Still, the general requirement for weight loss is to increase total energy expenditure ‘volume’, i.e. through increasing the frequency, intensity and duration of physical activity (Box 2).
{kind=link}
3. Recognise the hierarchy of determinants of obesity (the bigger picture)
Every person is different. It is useful to consider the wide range of possible determinants of disease (Figure) and identify the key factors driving weight gain or inhibiting weight loss in an individual that should be prioritised for intervention.
{kind=link}
For example, stress can lead to greater food intake, less physical activity and changes in metabolic rates in one individual but may have the opposite effect in another. Lack of sleep can affect a person’s ability to be physically activity during the day as well as their food intake. All determinants on the pathway need to be considered and not just one end, or even one aspect of one end (e.g. diet or exercise at the proximal end).
This will also require focusing on the patient’s environment, both micro (e.g. home, neighbourhood, school, etc) and macro (e.g. city, country, world, etc),7 to understand the often-unrecognised influences on energy balance and, if possible, act to relieve these or at least acknowledge their influence.
4. Check parental and family weight history and invoke family and/or peer support
Genetic makeup plays a big part in the risk of weight gain and the ease of weight loss. However, this effect is the result of the interaction of numerous genes associated with energy regulation rather than a single gene defect. Thus, although expensive gene sequencing techniques are now becoming more available and affordable, there is no need for these techniques in the clinical situation as the presence of one or both obese parents and obese sibling/s indicates a genetic predisposition and implies an added level of complexity in dealing with the problem. There is a strong interplay between genes and the environment in the development of weight problems. As families share environment as well as genes, it is important to consider problem lifestyle behaviours within a family. (To differentiate this, one of our colleagues suggests asking the patient if their mother, father or siblings are overweight or obese and if the family dog or cat is overweight or obese.)
Family and/or peer support should also be encouraged in any prescribed weight management program. Our experience with the men’s program GutBusters suggests a female partner will generally support a male partner’s program, but this is not necessarily the case in reverse.20 Peer support can also be encouraged through pairing the patient with a partner (buddy system). The use of group education, shared medical appointments and programmed shared medical appointments is another way to use peer support to assist the treating clinician.21
5. Consider the environmental influences on the patient
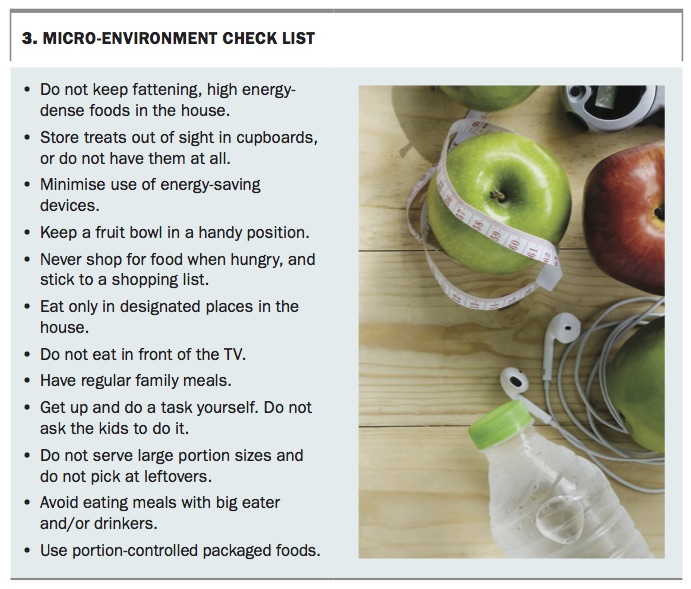
The environment in which we live and work includes elements of various types and levels that can influence a patient’s risk of and response to weight gain and loss. Elements of the environment are often characterised as physical, political, economic and sociocultural, which operate either at a macro or micro level to influence components of energy balance.
At the clinical level, it’s difficult to deal with many of these environmental influences, particularly at the macro-environmental level. But it is feasible and necessary to consider the micro-environmental elements (e.g. home, schools, neighbourhood), although this area is often overlooked due to the difficulty and time-consuming nature of dealing with these issues. Still, it is possible to mitigate the potential negative influence of the micro-environment with a range of simple strategies to change dietary or activity responses that may contribute to an excess or positive energy balance (Box 3).
{kind=link}
6. Realise the limitations of counting calories
Self-weighing and self-monitoring of diet, activity and other behaviours has consistently been linked with better weight-management outcomes.22 In recent times there has been an explosion of electronic applications that promise to improve the ease, completeness and interpretation of this monitoring process, such as activity trackers like Fitbits and heart rate monitors, although their utility over simpler recording techniques remains unclear.23 Many of these programs claim to calculate total calorie intake and predict the amount and rate of weight loss. However, calorie counting should be viewed with scepticism. The claimed accuracy of calorie counts of these programs is greatly exaggerated, and the limitations of calorie-intake data make calorie counting less meaningful in terms of weight management.
The calorie (or kilojoule) content of food is usually seen as the amount of energy stored within that food and is accurately measured by burning the food in a calorimeter or more usually estimated from the constituent macronutrient composition. It is often assumed that each calorie consumed has the same contribution to energy balance regardless of how the food is consumed or who consumes it. However, individual differences in metabolic rate, the compensation of the microbiome in the gut, digestion, thermogenesis and a range of other factors can lead to small but meaningful differences in how much of that calorie is available to an individual.24 This can lead to the same calorie surplus or deficit resulting in different weight gain or weight loss outcomes in similar individuals. Thus, strict calorie counting is misleading and best avoided.
Another implication of this observation is that although it remains important to encourage reduced energy intake ‘volume’ and increased energy expenditure ‘volume’ (as set out in points 1 and 2), the means of achieving this objective and the ‘volume’ of energy associated with the same change in behaviour may vary between individuals (or even within individuals). Some experimenting will be required to determine the extent of behaviour change required to achieved the desired weight loss for each individual patient.
7. Avoid fad diets and single-option programs
It has been well established that any diet that conforms to principle 1 above (where energy expenditure exceeds energy intake) can achieve at least short-term weight loss, but that the best ‘diet’ (more properly called an ‘eating plan’) for any one individual is one that can be adhered to over the long term.25 Fad diets and single-option weight-loss programs as promoted in common diet or weight-loss books, as well as an over-reliance on calorie counting alone, rarely meet these criteria and should be avoided.24 It is best to devise a long-term eating plan that is not overly rigid and that can be rationally adhered to even with diversions along the way. Patients who require strict instructions may not welcome this approach, but it is likely to be best maintained over the long term in the current environment.
8. Focus on weight-loss maintenance as much, or more than, initial loss
Although short-term weight loss is relatively easy to achieve, maintenance at the lower weight is more problematic. As pointed out above, evolutionary selective pressures favour the storage of excess energy over the potential survival threat of undefended weight loss. Hence, it is well established that adaptation processes, such as changes in the gut hormone levels or gut microbiota, may result in increased hunger or more efficient ‘food harvesting’ that promotes weight regain for years after a major weight loss.
In addition, the imperative for weight regain may be influenced by the length of time and degree of overweight before these losses. A strong focus on weight maintenance after loss is therefore vital, requiring regular and ongoing support at the clinical level. The balance of treatment may also vary, such that physical activity takes on a more important role than in initial weight loss.19
9. Evaluate and act on hunger
Hunger is the biological drive to need to eat. Appetite is the psychological drive to want to eat. The former is inbuilt and difficult to divert. The latter is an interaction between physiology and cognitions, resulting in a learned response, and can therefore be unlearned (e.g. eating associated with drinking, time of day and social occasions). Where genuine hunger is diagnosed as the reason for energy imbalance, the clinician needs to consider foods, drinks and drugs that can delay or avert hunger. Low energy-dense, high-fibre foods and drinks (i.e. fruits, vegetables, grains, water) are first-line approaches to this.26 However, there is some evidence supporting the use of products such as chewing gum, capsaicin (e.g. chillies, curries, red peppers), nuts and green tea as mild hunger suppressants.27 If unsuccessful, recourse to medication (e.g. phentermine, exanatide and liraglutide) might be considered, particularly if metabolic syndrome is a comorbidity.
However, it is often noticed that obese patients do not report genuine hunger but have a ‘learned’ appetite. Food intake in these cases is driven by other factors, generally psychological, or in some cases simple habit. Psychological issues, including occupational, family or existential stresses or adverse childhood experiences,28 should be considered and dealt with, or the patient referred to appropriate treatment, preferably before starting weight-control management.
10. Understand individual motivation and stages of change
In the modern ‘magic bullet’ environment, it is common for patients to expect their clinicians to provide a simple effort-free way to lose weight. This can result in a precontemplative or neutral motivational state from which the necessary changes in energy balance are unlikely to occur. Techniques such as motivational interviewing, recognising a stages-of-change model of motivation, are necessary to shift the motivation from ‘extrinsic’ to ‘intrinsic’, so the patient can learn to self-manage what is essentially a chronic, long-term and often relapsing problem.29
Conclusion
Obesity, and particularly the lifestyle factors and determinants associated with weight gain, have important implications for health, but established treatment techniques for dealing with these issues at the clinical level are far from universally effective. Australia was one of the first countries to develop clinical guidelines for managing overweight and obesity. Although these guidelines are evidence based and well considered, the continuing growth of the problem suggests that these have not been fully effective in dealing with the problem. The current article adds some practical suggestions in addition to the existing guidelines that aim to improve the understanding of the weight loss process, increasing patient engagement and add treatment options for the primary care clinician. MT
References
chronic disease management in clinical practice. Aust J Gen Practice 2017; in press.