The cardiac complications of obesity


Obesity
Heart diseases
Obesity is a powerful risk factor for cardiovascular events, but accumulating data suggest that patients can remodel their hearts and improve health outcomes by losing weight.
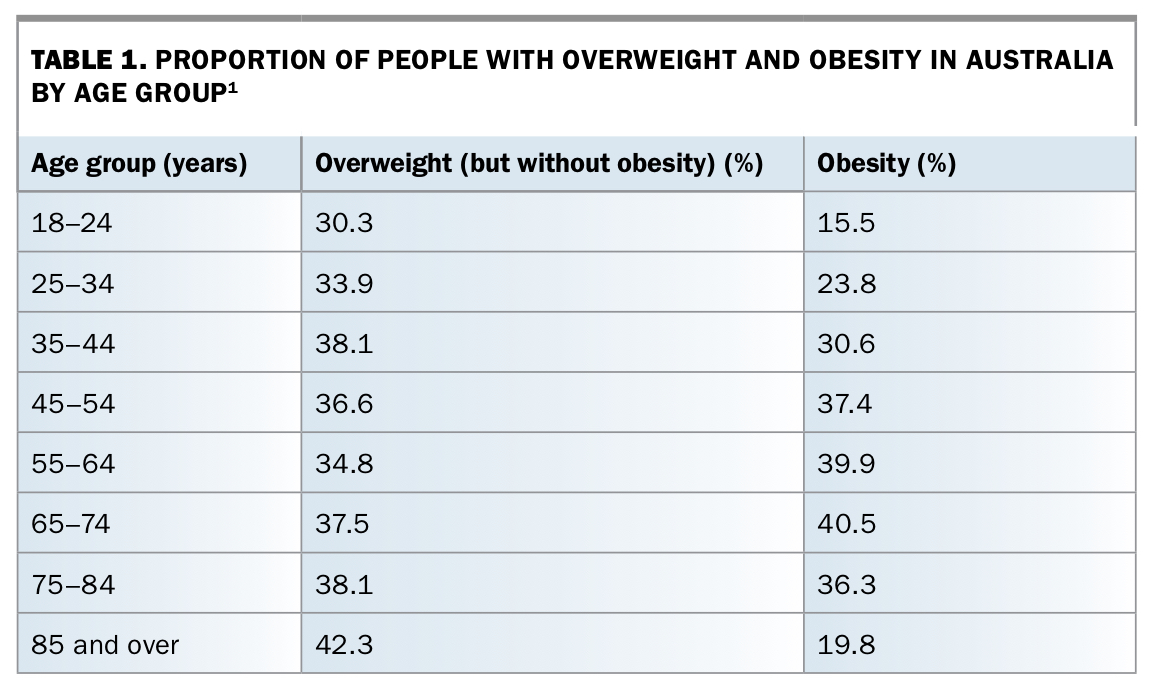
- The majority of people in Australia have overweight or obesity.
- The impact of obesity on cardiovascular (CV) risk is multifactorial and self-amplifying.
- Patients with morbid obesity and coronary syndromes are prone to increased procedural complications and poorer outcomes than patients of normal weight.
- Doctors are strongly advised to inform their patients who have obesity of their elevated CV risk profile and mortality.
- Data increasingly suggest that patients can remodel their hearts and health outcomes by losing weight.
- Accumulating evidence from prospective trials has shown that various forms of bariatric surgery may have positive impacts on CV endpoints.
A 27-year-old woman attends your practice regularly. She has morbid obesity, with a body mass index (BMI) of 47 kg/m2. Her comorbidities include hypertension, for which you have commenced her on perindopril 5 mg daily, and newly diagnosed atrial fibrillation (AF), for which you have prescribed metoprolol 25 mg twice daily. You are considering referring her to a cardiologist for possible atrial fibrillation ablation (pulmonary vein isolation).
What is the significance of this patient’s morbid obesity in terms of elevating her cardiovascular (CV) risk? What is the connection between her morbid obesity and her other comorbidities? If she were able to lose weight now, would she be able to reverse her CV risk profile and alleviate her current comorbidities? What options are available for weight loss?
Obesity in Australia
Australia, like all other developed countries, is experiencing a ballooning epidemic of obesity. The majority of people in Australia now have overweight or obesity (Table 1), with a fourfold increase in obesity having occurred over the past 30 years.1 The largest increase has occurred in the group of individuals with ‘morbid obesity’, equating to a BMI of 40 kg/m2 or above. Consequently many obesity researchers have begun to use additional classifications such as ‘super obesity’ (BMI ≥50 kg/m2) and ‘super-super obesity’ (BMI ≥60 kg/m2).2
{kind=link}
The rise in morbid obesity impacts heavily on the Australian economy, with annual costs calculated at $58 billion.3 This figure includes direct healthcare costs for morbid obesity and its known complications, disability pension costs and loss of productivity. In the Global Burden of Disease Study, obesity was identified as the strongest contributor to the burden of disease for modern Australasia.4
In many ways, the epidemic of obesity in the 21st century evokes the epidemic of smoking in the 20th century. Both are culturally-dependent epidemics, and both obesity and smoking are powerful modifiable risk factors for CV events. Despite the common misperception, morbid obesity is in fact a significantly stronger risk factor for premature myocardial infarction than smoking.5 Highly successful public health campaigns significantly reduced the prevalence of cigarette smoking; health organisations and doctors will need to campaign against environmental factors enabling obesity in a similar manner to promote national CV health. Food companies may resist (like cigarette companies), with advertising of unhealthy foods, promotion of such foods to children, and sponsoring of events.
Obesity and cardiovascular risk
Physiology
The impact of obesity on CV risk is multifactorial and self-amplifying. Obesity augments CV risk by multiple mechanisms, as illustrated in the Figure. The direct mechanical effect of excess adipose tissue increases total body blood volume, cardiac filling pressures and sympathetic activation, leading to an increased cardiac workload and cardiac hypertrophy. Adipose tissue also increases cardiac afterload and chest-wall resistance, enabling the development of both systemic hypertension and obstructive sleep apnoea.6
Adipose tissue is more than just a mechanical load, however, creating a web of metabolic consequences. It is very active metabolically, both in synthesising and in metabolising numerous substances. These substances are predominantly pro-inflammatory and prothrombotic (tumour necrosis factor-alpha, interleukin-6, plasminogen-activator inhibitor 1, oestrogen) or worsen insulin resistance and lipid metabolism (leptin, adiponectin, insulin-like growth factor, insulin-binding-protein 3).7
Clinical events
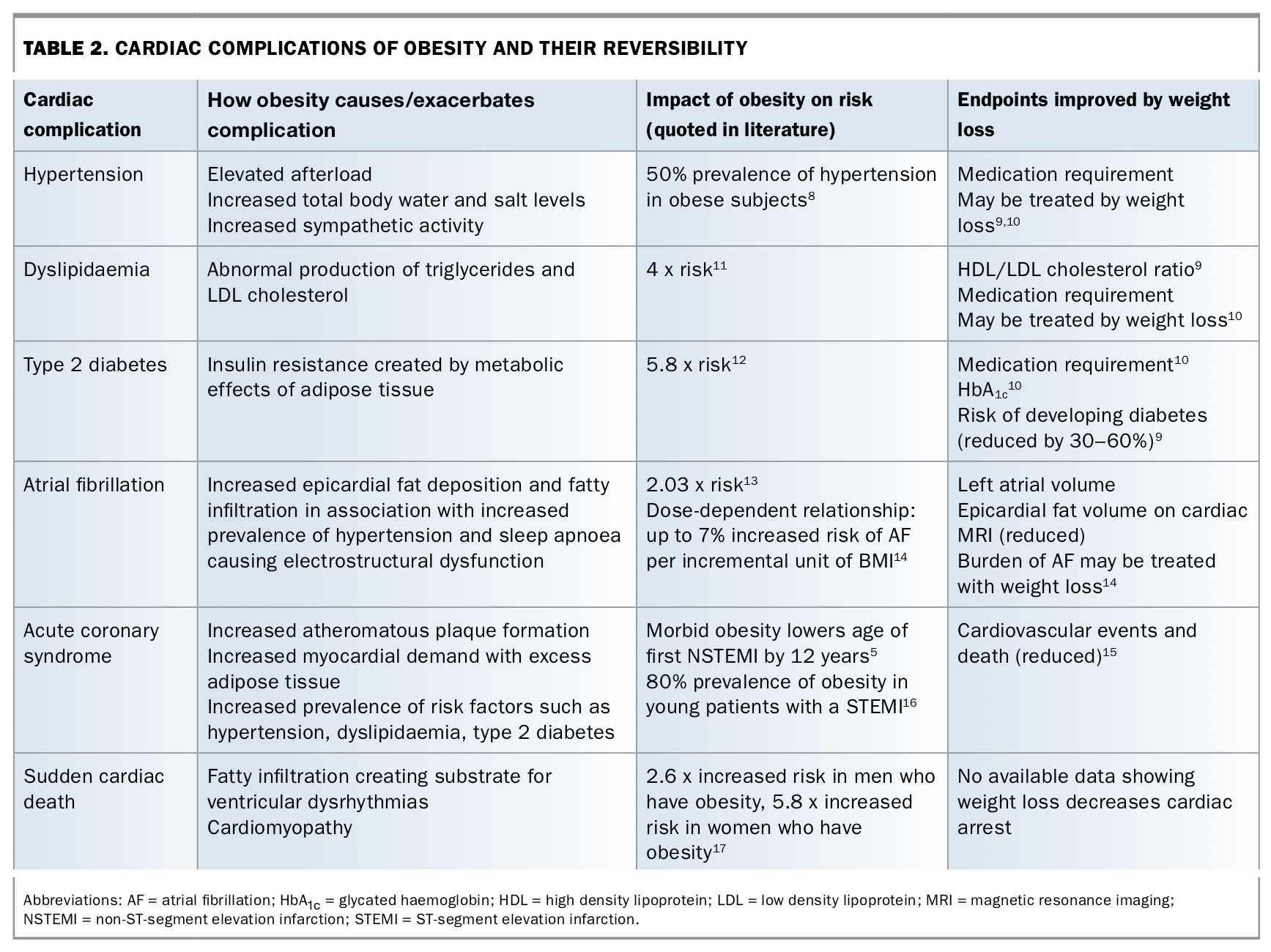
The physiological effects of obesity directly elevate the risks of multiple cardiac conditions (Table 2).8-17 Hypertension and dyslipidaemia are widely prevalent in patients with obesity, and the association of hypertension, dyslipidaemia and central obesity has been formally recognised in ‘the metabolic syndrome’. Type 2 diabetes is also strongly associated with obesity, which has led to the coining of the term ‘diabesity’.18
{kind=link}
The presence of obesity as a contributing risk factor for several cardiac conditions now features prominently on several risk scores (e.g. STOP-BANG score for obstructive sleep apnoea and Q-RISK3 score for cardiovascular risk). Further, the presence of obesity is a feature of the H2FPEF score for heart failure with preserved ejection fraction (HFpEF).19 This reflects that obesity is very strongly associated with HFpEF,20 with up to 80% of patients with HFpEF either having overweight or obesity.21
The combination of cardiac hypertrophy and direct fatty infiltration creates a substrate for arrhythmias. The most common arrhythmia observed is AF, and the dose-dependent link between obesity and AF is now well established. Pathak and colleagues have quoted an increased risk of 3 to 7% for developing AF for each incremental unit of BMI.14
Patients who have obesity also have an elevated incidence of ventricular dysrhythmias, raising the risk of sudden cardiac death.22,23 Obesity is now the leading cause of nonischaemic sudden cardiac death in young people,17,24 responsible for approximately 25% of cases. Cardiopulmonary resuscitation is more difficult in those with obesity, potentially further compromising outcomes.
A 2008 study of more than 100,000 patients with acute coronary syndromes demonstrated that morbid obesity is now the most powerful risk factor for premature CV events, lowering the age of first coronary syndrome by a mean of 12 years.5 By contrast, smoking lowered the age of first coronary syndrome by a mean of only 9.7 years.5
With an increasing morbidly obese population, cardiologists are seeing an increase in young patients with ST-segment elevation infarctions (STEMIs). A 2011 study into the high prevalence of obesity in young patients with STEMIs found that almost 80% of young patients (men aged less than 45 years, women less than 55 years) who experienced a STEMI had obesity.16
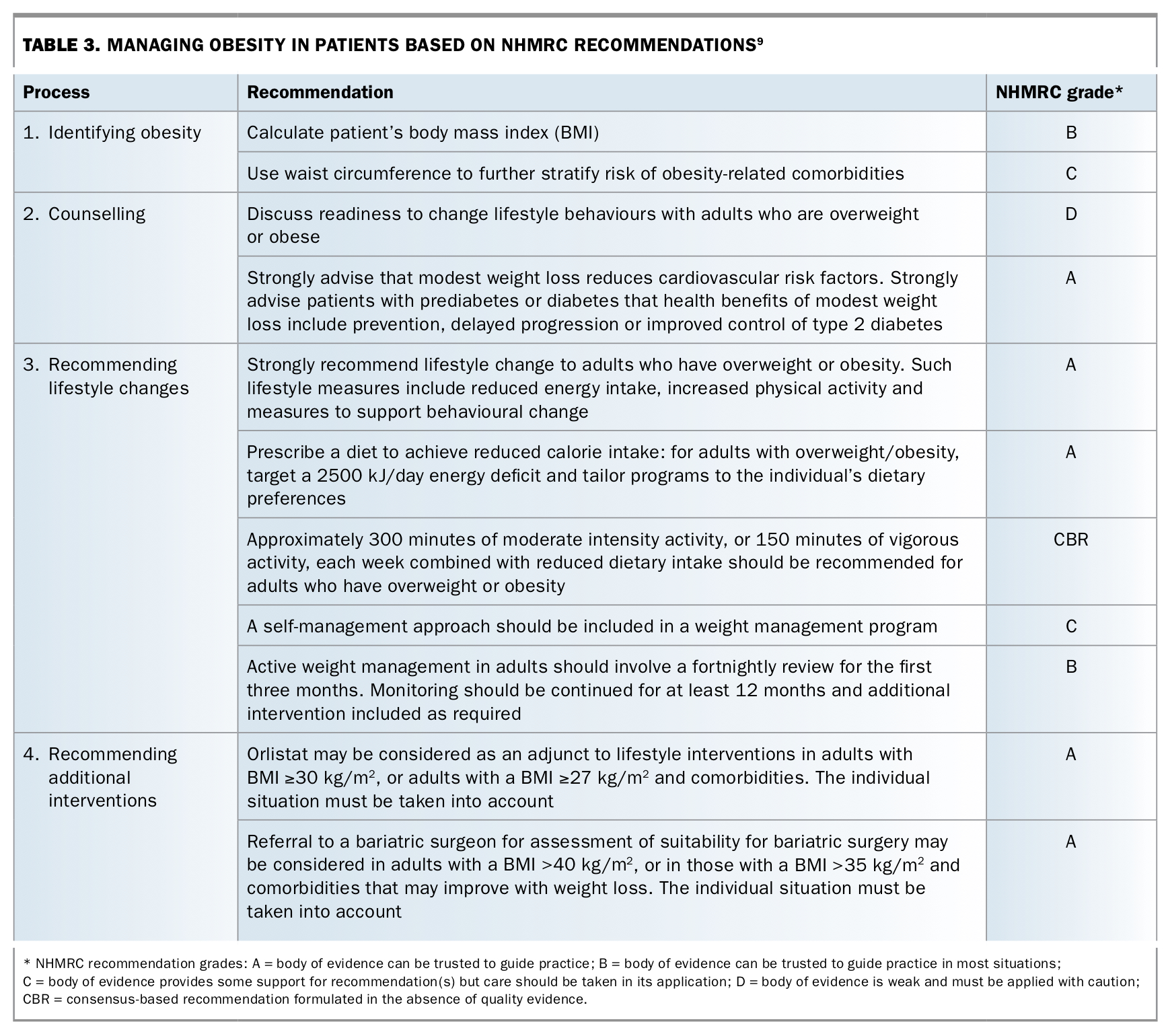
Appreciation of the adverse effects of obesity has driven recommendations in societal guidelines. For instance, in the NHMRC guidelines on the management of obesity, doctors are strongly advised to inform their patients who have obesity of their elevated CV risk profile and mortality (Table 3).9
{kind=link}
Morbid obesity and procedural complications and outcomes
Despite typically being younger, patients with morbid obesity and coronary syndromes may be prone to increased procedural complications and poorer outcomes than normal weight patients. Cardiac work-up of patients with obesity is problematic, both in the difficulty of these patients exercising and in the poor image quality achieved across a range of investigational modalities. The ECG from such patients often has baseline abnormalities that obscure correct interpretation (for example, axis deviation or diffusely low QRS voltages).25 In addition, false-positive results suggesting ischaemia have been recorded at higher frequency for patients with morbid obesity undergoing echocardiography, stress echocardiography and stress thallium testing.26
Coronary angiography may be hazardous for patients with obesity, with complication rates in excess of those experienced by normal weight patients. The Blue Cross Blue Shield of Michigan Cardiovascular Consortium registry is one of the largest registries from which CV outcomes in patients with morbid obesity have been assessed. In 2013, analysis of data from 227,044 patients in the registry undergoing percutaneous coronary intervention revealed that compared with overweight patients, patients with morbid obesity experienced more vascular complications, almost twice the rate of contrast-induced nephropathy, a fourfold increased risk of contrast nephropathy requiring dialysis, and an increased risk of mortality (odds ratio, 1.63).27 This increased risk of mortality has been confirmed in other publications.28,29 Other problematic elements of coronary angiography include three to four times the typical quantity of radiation exposure, increased contrast use and lengthened procedural time.30
For patients with morbid obesity requiring cardiothoracic surgery, risks remain elevated above baseline. Australian data suggest that morbid obesity is associated with prolonged ventilation, deep sternal wound infection, renal failure, return to intensive care and longer length of hospital stay.31 International studies have confirmed these elevated risks32 and associated increased costs,33 and have stated that the increased number of patients with obesity undergoing cardiothoracic surgery ‘demands attention’.
Can cardiovascular morbidity be reversed by weight loss?
It can be dispiriting to connect the links between increased CV risk in obesity and consequent worsened outcomes. However, data increasingly suggest that patients can remodel their hearts and health outcomes by losing weight. Some of the most powerful data in this area are Australian and may ultimately dramatically shape future guidelines on CV care of patients with obesity. GPs will have a key role in this new paradigm of obese CV care (Table 3).
It is increasingly being recognised that successful weight loss may alleviate the ‘metabolic syndrome’, with reductions in hypertension, dyslipidaemia and insulin resistance. One of the most powerful trials to date bearing out this association was the STAMPEDE (Surgical Treatment And Medications Potentially Eradicate Diabetes Effectively) trial.34 In this trial, published in The New England Journal of Medicine in 2012, 150 obese patients with type 2 diabetes mellitus received either medical treatment for their obesity or a combination of surgical (gastric bypass or sleeve gastrectomy) and medical treatment. Although external validity is limited by its nature as a single-centre, nonblinded study, results were highly significant. Patients in the combined surgical and medical arm of the trial lost an average of 27 kg of weight over 12 months. This weight loss was associated with mean improvement in HbA1c from 9.4% to 6.5%, a 28.4% improvement in HDL-cholesterol readings, and a 43% improvement in triglyceride levels. Particularly impressive was the significant reduction in patients’ requirement for diabetes medications and lipid-lowering, antihypertensive and antithrombotic agents following surgery. These outcomes, including the degree of weight loss, were largely sustained at the three-year follow up in 2014.10
The findings of this trial suggest that significant weight loss achieved by surgery may outperform many of our currently available medications in terms of reducing hypertension, dyslipidaemia and insulin requirements. In some cases, weight loss appeared to have induced complete remission of these conditions, with remission sustained for at least three years’ follow up.
A South Australian cardiac team has provided further support for the key role of weight loss in improving CV health, this time in the context of AF. As described earlier, AF may be mechanistically linked to obesity via systemic hypertension, cardiac hypertrophy, fatty infiltration of cardiac muscle and electroanatomic remodelling. Obesity is now the second-highest population attributable risk for AF behind hypertension.35 Pathak and colleagues have shown that weight loss has a dose-dependent effect in reducing patients’ burden of AF.36 Patients who were able to lose more than 10% of their body weight had a sixfold greater probability of remaining free from AF. This reduction in AF has also been shown to be associated with structural improvements in cardiac measurements, with partial reversal of pathological cardiac remodelling.37
There are also increasing data suggesting that even established coronary artery disease may be attenuated or reversed by weight loss. In one observational study, patients who achieved sustained weight loss with Roux-en-Y bypass had reduced coronary calcification compared with patients with obesity, and assessment of atherosclerotic carotid plaque patterns showed a similar trend.38 In the Swedish Obese Subjects study in 2012, the risk of CV events and death was significantly reduced in patients with obesity who underwent bariatric surgery compared with obese control subjects receiving usual care (hazard ratio, 0.67).15 It is worth noting, however, that in post-hoc statistical analysis, risk reduction was not able to be definitively linked with the observed weight loss; the authors suggested a range of possible reasons, including underpowering.
How can patients with morbid obesity lose weight?
Weight loss appears increasingly to be one of our most powerful weapons against CV disease. However, achieving and sustaining significant weight loss is not easy. It is believed that a complex interplay of genetics, epigenetics, diet, exercise and shifting cultural patterns have led to the current ‘obesity epidemic’. Despite recognition of the rewarding benefits of weight loss, it is not possible to reverse all predisposing factors (i.e. strong genetic factors, possible in utero effects) for obesity.
Practically, it is usually not feasible for patients with morbid obesity to participate in regular exercise programs to an adequate degree to achieve weight loss. Pharmacotherapy may be effective for people with obesity when combined with lifestyle modifications and can be considered to prolong weight loss after bariatric surgery.39
Obesity surgery is hence emerging as an increasingly popular first step to weight loss in the population of morbid obesity, and is likely to become more available to Australians. Government bodies are now recognising it as a cost-effective intervention, and, as mentioned above, its ability to improve health outcomes was clearly demonstrated in the STAMPEDE trial. Accumulating evidence from prospective trials has shown that various forms of bariatric surgery may have positive impacts on CV endpoints.40
A suggested approach for doctors involved in the care of patients with obesity is outlined in Table 3, based on the 2013 NHMRC’s Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia.9 Within these and other international guidelines, the role of referral for consideration of bariatric surgery is increasingly being emphasised, particularly for patients with comorbidities that are identifiable as obesity-related.41 Assessment before such surgery is essential and lifetime follow up afterwards is necessary as nutritional deficiencies and other side effects must be minimised.
Conclusion
Morbid obesity is increasingly common in Australia today. GPs will see many patients with morbid obesity in their practice who have associated cardiac comorbidities. It is important that doctors and patients appreciate how powerfully morbid obesity amplifies the risks of premature CV events, and that it may in fact be an even stronger risk factor than smoking. This is especially the case for people with HFpEF, where obesity is very strongly associated.
Patients with morbid obesity are likely to have many CV comorbidities, and hence earlier cardiac events. When they experience cardiac events and interventions, they are at risk of significantly worse clinical outcomes.
Reversal of morbid obesity appears to be a potent intervention for reversing the burden of disease experienced by the morbidly obese. Cardiac comorbidities may be alleviated by weight loss, and medication requirement may be significantly reduced.
Alongside counselling patients sympathetically about diet and suitable exercise, GPs will increasingly be able to expedite referrals for obesity intervention to help optimise the CV risk profile of patients with obesity. MT