Improving mental health and reducing suicide risk: how GPs can help during the COVID-19 pandemic

Dr Su is Academic Lead (GP) at the Health Education and Training Institute Higher Education, Sydney; and Adjunct Clinical Senior Lecturer in the School of Medicine, The University of Notre Dame Australia, Sydney, NSW.
Associate Professor Stone is Clinical Associate Professor, Academic Unit of General Practice, ANU Medical School, Australian National University, Canberra, ACT.
Associate Professor Blashki is Associate Professor at the Nossal Institute for Global Health, The University of Melbourne, Melbourne, Vic.
Mental health
Suicide
A potential 25% increase in suicides per annum has been predicted in Australia as a result of the distress associated with the COVID-19 pandemic. This article looks at how GPs can support the mental health of their patients while also taking care of their own wellbeing during this crisis.
Recently, the Australian Medical Association, Brain and Mind Centre, and Orygen, Centre for Youth Mental Health issued a joint statement that the COVID-19 pandemic was likely to lead to increased rates of suicide and mental illness.1 According to their modelling, they predict that there may be a 25% increase in suicides, and 30% of these may be among young people. They estimate an additional 750 to 1500 people per annum will be lost to suicide in addition to the 3000 lives lost per annum before the COVID-19 pandemic. In 2018, there were 3046 suicides in Australia, and suicide is the most likely cause of death in young people.2 Economic downturn may worsen this figure and, if the economic situation persists past 12 months, the increased risk is predicted to continue for up to five years. This difficult period comes just after the ecological disaster of mega-bushfires in Australia. Of course, Australian communities are resilient and supportive during crises and it is unclear precisely how these contemporary challenges will impact on suicide rates.3,4 Nevertheless, as the first point of call for many people in times of distress, it raises the question: how can GPs best prepare to manage this increased risk?
Impacts of COVID-19 on community mental wellbeing
The precise population mental health impacts of COVID-19 are still largely unknown, though we do know that there has been a surge of around 30% in the mental health support services such as Beyond Blue.5 Apart from the well-known risk factors for suicidal behaviour, the pandemic adds another layer of risks and stresses on people’s mental health. Because of the recency of the COVID-19 pandemic, many of the practice principles described in our paper are inferred from the general suicide prevention research rather than COVID-19-specific studies, which are yet to be undertaken.
GPs function at the nexus between clinical medicine and the community, and it is useful to take a step back and look at the various phases of societal responses to a community crisis.6 There may be an apparent lessening of distress in the initial phase as people focus on what needs to be done and there is a sense of solidarity in the community pulling together. A later disillusionment phase is influenced by their perception of injustice in resource allocation. For some, this sense of inequality can persist and result in long-term sequelae. With this in mind, the GP can be particularly vigilant to patient crises during high-risk times as well as to changing levels of mental distress in the different phases of a patient’s response to a natural disaster.
The economic impact of the pandemic may include job loss, financial loss and changes to support services and/or living circumstances including loss of stable accommodation. These impacts can compound to adversely affect people’s mental health. Even for those who have not previously considered themselves to be vulnerable to mental illness, economic downturns may pose a risk to their sense of identity, and sense of meaning and life direction. Suddenly, they may become acutely anxious or depressed, which profoundly affects their sense of self.
Effects of isolation
Changes to people’s daily work and home routines have proven to be a major challenge to maintaining their mental health. For some, isolation at home and endless video-chat meetings have taken a toll on their mental wellbeing and, as the months pass by, they become fatigued and have a sense of disconnection. For others, home life has become a pressure cooker with children at home and partners working from home. Notably, there has been a significant rise in the number of calls to domestic violence services.7
It has been said that a crisis can bring out the very best in people and also the very worst, and xenophobia and discrimination have been an unfortunate response from some parts of the community during this pandemic. Fearmongering about ‘the Chinese threat’ or scapegoating of the residents of North Melbourne’s public housing towers have reintroduced an unhelpful and stigmatising narrative for some of our patients from culturally and linguistically diverse backgrounds. The contribution of discrimination to poor mental health is well documented and GPs, as leaders in the community, can be vocal in countering unacceptable stereotypes.8
The gradual loosening up of isolation restrictions brings its own challenges. Some people, having retreated to the ‘cocoon’ of home isolation have found it to be a haven away from other life stressors, allowing them time to recalibrate and reassess. For some, it has been a time for reflection and has been transformative. For others, for example those with anxiety conditions, it has specifically potentiated avoidant behaviours and re-emerging after lockdown can be stress inducing.
Patterns of usage have changed for patients with substance use disorders or other addictions such as gambling.9 For example, the lack of daily structure and nonrequirement to attend work have opened the door to unhealthy drinking habits.10
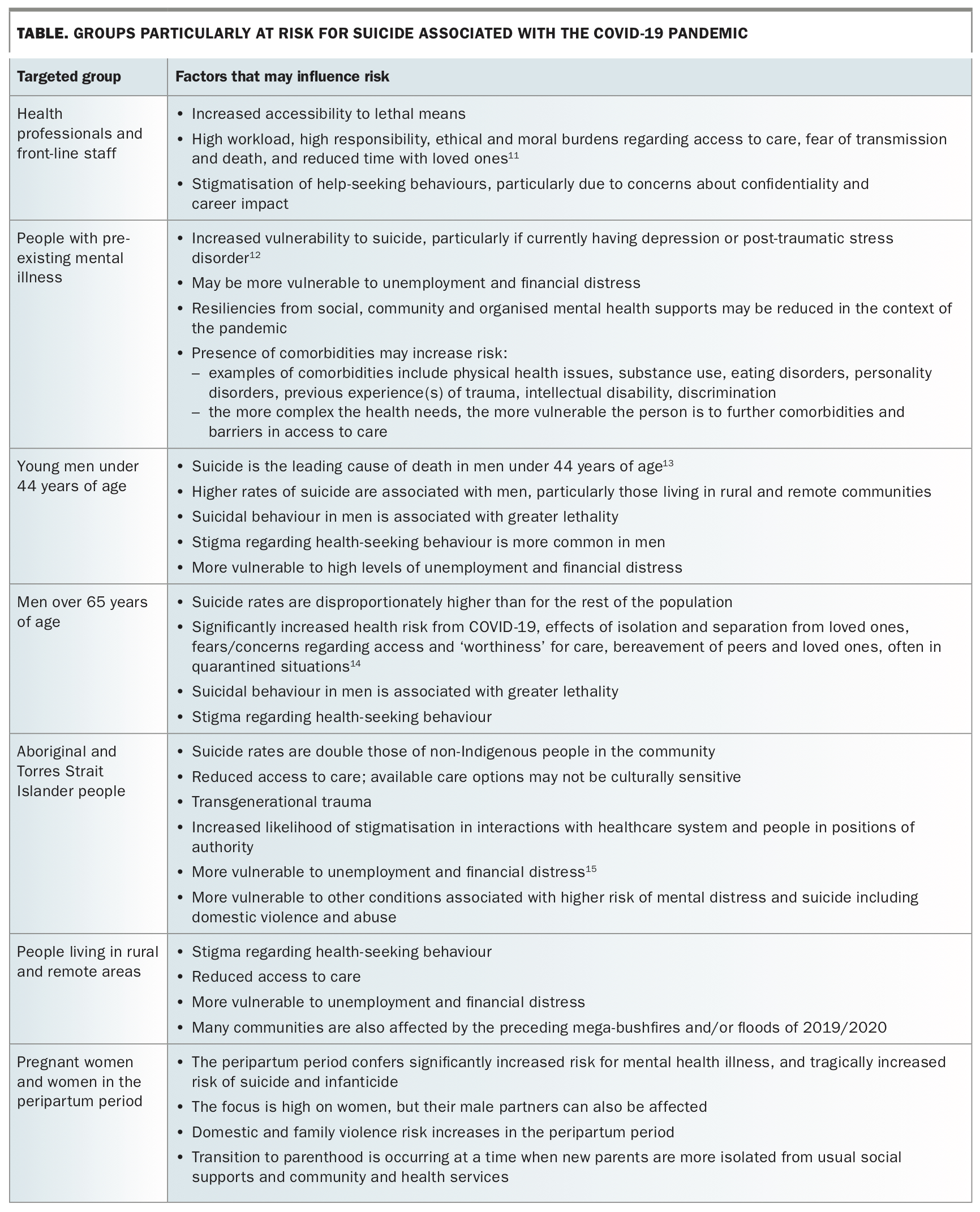
It is worth remembering that particular groups of people who were more vulnerable to suicide before the pandemic remain at risk. This includes those from Aboriginal and Torres Strait Islander communities, rural men, those discharged from forensic mental health services, young people and people with pre-existing mental illness (Table).11-15
{kind=link}
It is hard to say what impact isolation will have on the nursing home population in Australia, though it has been a difficult time for older Australians who are at higher risk of poor outcomes from the disease and find themselves unable to have the usual support from visitors during the isolation requirements. We do know a reduction in protective support may contribute to active or passive suicidal ideation.16
Listening for the underlying stories behind these vulnerable groups is a crucial step towards a therapeutic relationship and working together to address emotional distress associated from the circumstances. Problem solving and prioritising during crisis can then be achieved more effectively.
Impacts of COVID-19 on the medical workforce
The pandemic has highlighted the importance of proactive support of the mental wellbeing of the medical workforce. COVID-19-related stresses include uncertainty about the scale of the pandemic, distressing news from overseas experiences, the challenge of physical distancing (initially called social distancing) and adjustments to new forms of operation such as telehealth. Unfortunately, entrenched cultural issues in the workforce, such as bullying, harassment, and unsustainable working hours and conditions, are likely to escalate during this time of prolonged stress.
Initial projections about populations affected with COVID-19 prompted drastic reforms in the health sector in preparation for a patient load predicted to overload the health system. Health professionals in Australia were particularly concerned by stories about their international colleagues and the traumatising ethical dilemmas they faced in resource allocation. Lack of personal protective equipment necessary to safely carry out face-to-face duties was a great source of stress. The high-profile reporting of the suicide of Dr Lorna Breen, an emergency doctor working in Manhattan in the US, reverberated through the health community.17
Physical distancing has meant the loss of touch, of connection. For GPs on the front line, it has meant a complete restructure of their mode of practice. Telehealth has been widely embraced by Australian GPs and their patients, and it has afforded the opportunity to provide health care for chronic medical conditions in addition to mental health care using telephone or video-chat facilities. However, telehealth is not ideal for all patients. It presupposes access to a phone, computer or the internet, and the organisational and psychological foundations to be able to access telehealth. Many vulnerable patients have found the change of style of interaction has increased their isolation, often when they are already significantly isolated.18 Some patients report that this has stopped them from accessing care, even when care nominally may be available.19,20 For GPs, it has meant adapting their style of practice and the challenge of projecting empathy through a screen. Ensuring that there are reflective processes for individual and group practice can be an important mechanism to adapt to rapid changes.
What can GPs do to mitigate suicide risk?
Suicide prevention strategies can be conceptualised as primary, secondary and tertiary prevention.21
Primary prevention
Primary prevention includes public health initiatives from the government, including awareness campaigns, appropriate reporting in the media and reducing access to means.22 Government initiatives should be directed towards social determinants of health: financial support (both medium and longer term); a focus on rebuilding the economy; strategies towards reducing domestic violence, substance use and online gambling; and improved access to mental health education and support. The narrative that frames the disaster recovery is crucial; people need to hear that the burden of isolation was necessary.23 Examples of community messages that provided meaning or purpose include: ‘Staying home to save lives’; and ‘As a community, we support each other during a tough time’. As GPs, we can continue to stay up to date with and reinforce the community messages of COVID-19-specific health advice, as well as general public health advice. Government resources including federal, state and local council resources can be important to address the societal impacts of unemployment and financial or accommodation stress. GPs can assist and advocate to facilitate patients towards these resources. Primary Health Networks can help to improve the co-ordination between health professionals and the services available.
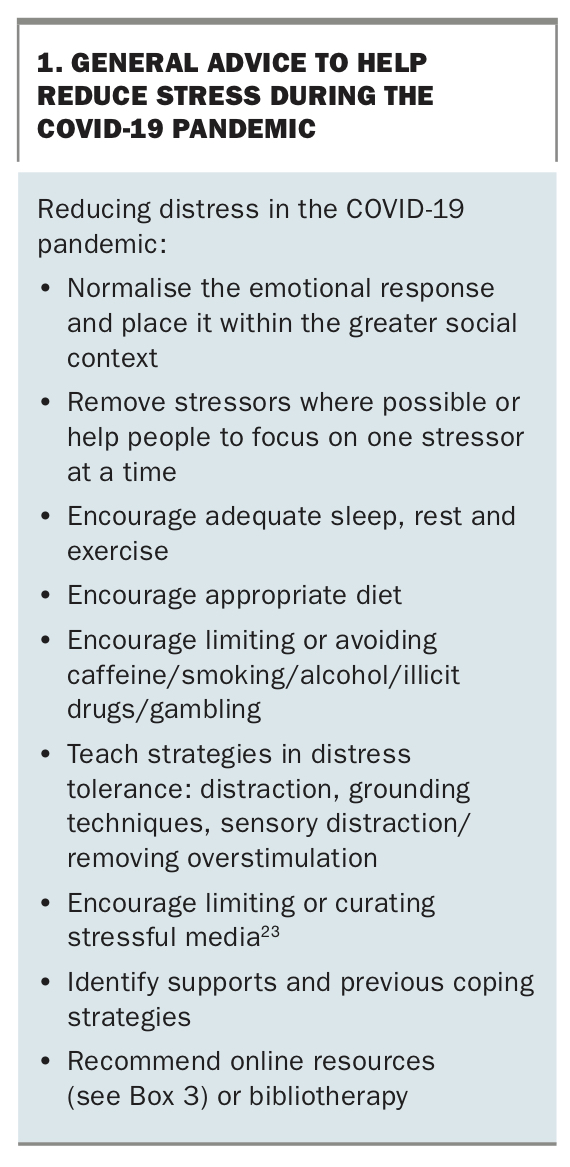
GPs also have an important role in early prevention through advising about management of stress and mental health conditions before they become more severe. Box 1 includes some common-sense advice and resources that GPs can provide for patients to manage their mental health and build resilience during the COVID-19 pandemic.24
{kind=link}
Secondary prevention
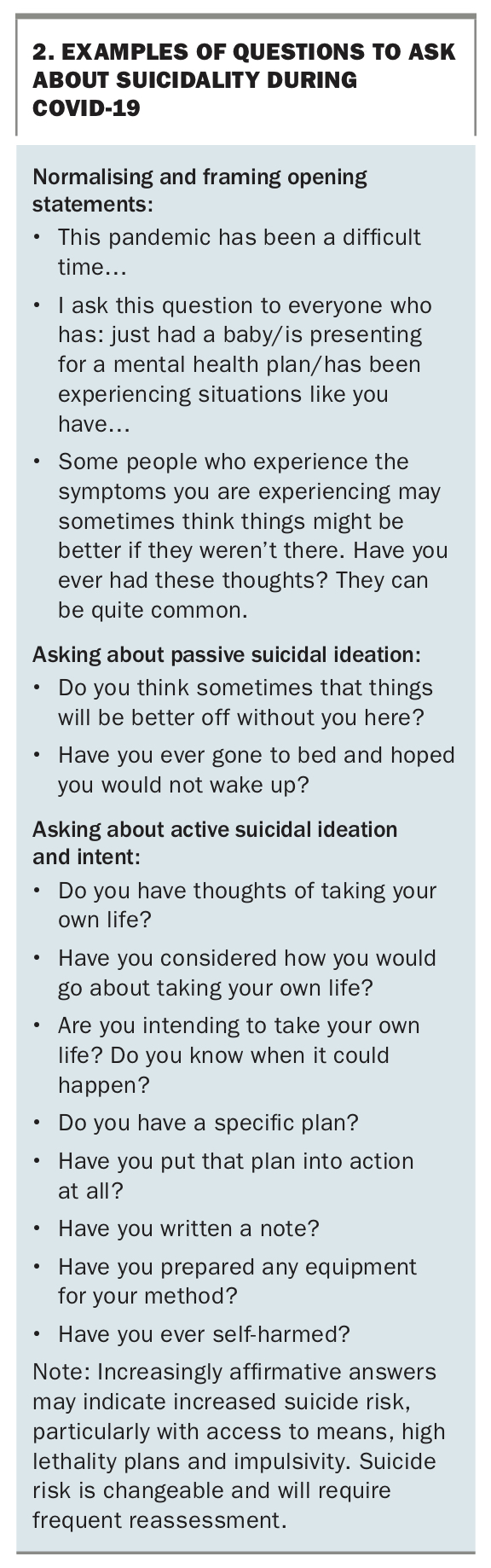
Studies show that many patients visit their GP in the months leading up to suicide (even for non-mental health reasons). Therefore, it is important that GPs are up to date on suicide assessment skills.25 GPs should be aware that suicide cannot always be accurately predicted even by the most highly skilled clinician with all the information available. Suicide assessment comprises multiple factors and is not a tick-box approach. Thus, although risk factors and screening tools can provide useful information, they cannot definitively predict the risk of suicide. Suicide risk assessment is unfortunately an inexact science.26 Raising the conversation with the patient requires delicate communication skills and some useful phrases are listed in Box 2. Relevance to the presenting issue and a nonjudgemental approach enhance patient acceptability of the question. Normalising and framing statements can help create a context for asking about self-harm or suicide.
{kind=link}
Suicide prevention plans
Putting in place a suicide prevention plan with a patient is good practice and can provide a template to monitor progress during subsequent consultations. One approach developed by Beyond Blue uses the Beyond Now app (Figure), which works with the patient to identify key steps in suicide prevention. The GP can ask the patient to download the app during the consultation if they have a smart phone and work through the pages, including topics such as: my warning signs; make my space safe; my reasons to live; things I can do by myself; people and places I can connect with; people I can talk to; and professional support. Patients can also download and use the app on their own and, to date, more than 80,000 downloads have been undertaken in Australia.
{kind=link}
Suicide contracts vs safety plans
In the past, suicide contracts were a common recommendation for managing suicide risk. Suicide contracts are now considered unhelpful as they can create a power imbalance at a time when the focus should be on empowerment. In contrast, suicide safety plans are developed with the person and consider the person’s resilience and supports to keep them safe. It is easiest to work on these when the person’s emotional distress is more contained.
Safe spaces and havens
Safe spaces and havens are another emerging, primarily peer-led initiative in some communities, providing a nontertiary alternative for people in suicidal crisis and can be crucial parts of a suicide prevention plan for vulnerable people.27 A safe space is a designated place that aims to provide a safe, welcoming and supportive environment for people experiencing psychological distress, allowing them to have an alternative to presenting to an emergency department.28
There are opportunities to set up such spaces within aftercare services or GP practices. These spaces can be equipped with sensory tools for emotional regulation, which can assist the person in distress to calm down.29 Sensory tools aim to be relaxing and can focus on sight, smell (aromatherapy), touch (e.g. stress balls, weighted fabrics), taste (e.g. sweet or salty food, tea), hearing (relaxing sounds) or proprioception (rocking chairs).
There is a plethora of community supports for mental health and suicide prevention including online resources and phone numbers through which people can speak to mental health professionals. Some of these are listed in Box 3.
{kind=link}
For some patients, their care may include a range of self-direction, personal supports, community supports and professional supports. Professional supports may be health related, financial, social, legal or vocational. These can be located in the community or in hospital as voluntary or involuntary admission. Framing the care as a whole-of-team approach, in which different levels of care may be necessary at different recovery points, can assist the discussion regarding at which point different levels of care may be enacted. This can be part of the safety plan. Having the person be part of the plan can be pivotal to retaining the relationship when involuntary care is required.
Tertiary prevention
Referral of patients at suicide risk to tertiary services is one of the more challenging referrals that GPs undertake. This usually involves a phone conversation with an intake worker who is trying to assess risk and usually balancing highly limited inpatient hospital resources. The GP can assist by having important information at hand, such as previous suicidal behaviours, previous psychiatric history, whether or not the patient has suicidal thoughts, suicidal ideation, intention, a clear method and access to means. Hospital admissions can sometimes be a circuit breaker and a haven of safety during an acute crisis, but the reality is that many of these patients then get discharged back to the GP who is still managing some degree of suicidal risk. Working with a team of mental health specialists with good communication about the plan is the ideal approach for managing ongoing suicidal risk. The most difficult situation is where the GP is highly concerned about the patient’s risk, but public mental health services do not accept to undertake care. In these cases, it is essential that the GP sees the person frequently, and considers re-referral as needed. For GPs, this is a difficult situation and it can be helpful to seek support from peers. Assertive advocacy is often needed to ensure the patient has access to a safe space if needed, and the GP may have to speak up on behalf of the patient or take a more directive role during crisis.
Rarely, a patient is at high risk to themselves and is unwilling to accept medical assistance. The focus of care is to put in place a collaborative plan that is patient centred and the least restrictive to keep the person safe. It may be necessary to enact transfer for assessment under the Mental Health Act and, if so, requirements differ between states. It is essential that GPs create a safe space where patients feel heard and understood, even if involuntary transfer is required, though in reality it is often an irreconcilable blow to the patient’s trusting relationship with the GP.
This has an added layer of complexity during COVID-19 as hospitals may be seen as risky during the pandemic. Section 203 of the COVID-19 Legislation Amendment (Emergency Measures–Miscellaneous) Bill 2020 was passed recently, amending the Mental Health Act 2007, permitting audio-visual assessment, and is intended to continue for the duration of the pandemic.
Conclusion
Suicide remains a significant and tragic cost and burden to individuals and the community. The unprecedented events of the mega-bushfires followed by the COVID-19 pandemic are predicted by some authorities to increase the risk of suicide, potentially causing more deaths in Australia than the virus itself. Disaster research shows that mental illness and suicide in the context of the pandemic may have a staged approach with an initial ‘honeymoon’ period, during the period of community cohesion and increased supports, followed by increased risk potentiated by disillusionment, particularly in vulnerable groups. Groups already at risk for suicide before the COVID-19 pandemic are further vulnerable to the health impact of COVID-19 and the psychological effects of isolation, bereavement and economic uncertainties. Health professionals are also particularly vulnerable given the nature and burdens due to the pandemic.
GPs play a pivotal role clinically in supporting mental health and undertaking suicide risk assessment and prevention. A suicide prevention plan such as the Beyond Now app can be helpful. Part of the plan can include strategies for when increasing supports are required. Telehealth is a mixed blessing providing more access for some and creating barriers for others. The rapidly changing nature of the pandemic has created additional stressors, although some health professionals and practices have used the opportunity for organisational restructure that will be beneficial into the future. GPs have also demonstrated strong leadership in advocating for appropriate health policy and the profession continues to play an important public health leadership role.
The impact of COVID-19 on health professionals is significant. Being adaptive to change, reflective of our own vulnerabilities and seeking support when needed can help to improve mental wellbeing. MT