Taking a grip of thumb osteoarthritis

Thumb base osteoarthritis is prevalent among the elderly population. It has a large impact on hand function and overall quality of life and presents a challenge to clinicians due to the lack of highly efficacious individual treatment options available. A combination of therapies is usually used to enhance the clinical effect of treatment.
Hand osteoarthritis (OA) is a common condition with higher prevalence among postmenopausal women.1 By the age of 85 years, about 40% of the population (47% of women and 24% of men) will experience symptoms of hand OA.2 The impact of hand OA on pain and subjective reports on health is similar to that caused by rheumatoid arthritis.3
Hand OA can be subdivided into three subtypes with potentially distinct risk factors and pathogenesis:
- thumb base OA
- erosive OA
- nodal or interphalangeal (IP) OA.1
Among these subtypes, thumb base OA presents as a challenge to clinicians due to its substantial clinical burden and lack of highly efficacious treatment options. Large population-based studies have estimated that one in 20 women aged over 70 years suffers from thumb base pain and has consulted a medical professional for that reason.4
Thumb base OA may occur in isolation or concomitant with IP (nodal) OA. Erosions are rarely present.5-7 In patients with symptomatic IP OA, presence of concomitant thumb base OA is associated with greater pain levels and functional impairment.8
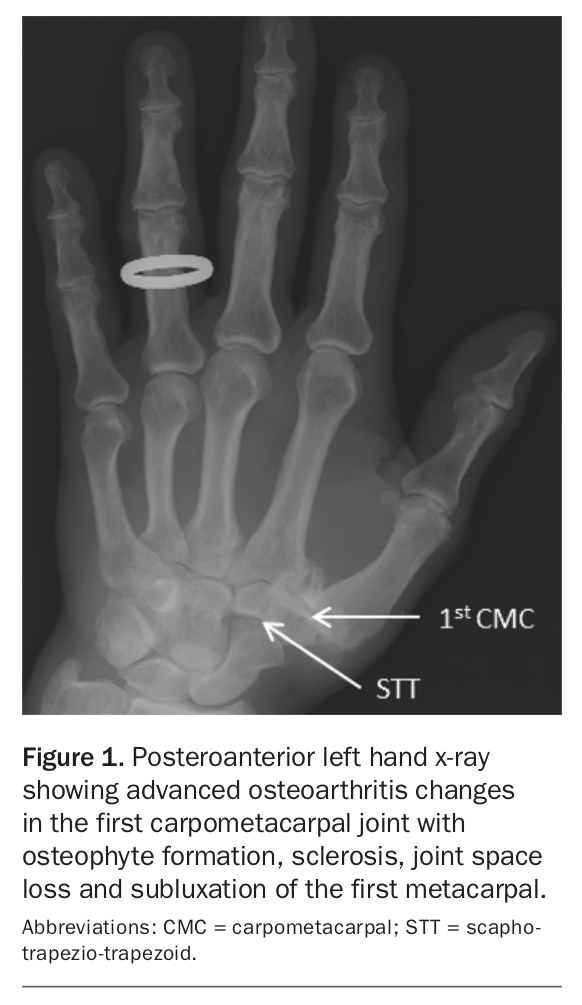
The pathogenesis of thumb base OA is believed to involve biomechanical factors.9 High forces across the first carpometacarpal (CMC) joint during strong pinching and grasping, coupled with the inherent instability to allow wide motion in several planes, are related to the development of joint changes. The scapho-trapezio-trapezoid joint may also be affected and contribute to thumb base symptoms (Figure 1). In this article, we use thumb base OA interchangeably with OA of the first CMC joint.
{kind=link}
Clinical presentation and diagnosis
Typical symptoms of thumb base OA include pain at the base of the thumb that is exacerbated by pinching and grasping, joint stiffness lasting usually less than 30 minutes and decreased hand strength and function with patients having consequent difficulties performing common activities, such as opening jars and using scissors.10 With the progression of the disease, joint deformity may be noticed with wasting of the thenar muscles, adduction of the first metacarpal and joint subluxation (squaring deformity). Other physical examination findings include pain elicited on palpation of the first CMC joint and joint swelling. Collapse of the first metacarpophalangeal (MCP) joint with MCP hyperextension may be present during pinching, contributing to the severity of the pain at the base of the thumb.
The diagnosis of thumb base OA can be made clinically based on a suggestive history and physical examination in patients 40 years and over. There is no diagnostic criterion that is specific to thumb base OA. Complementary tests (such as x-rays or laboratory tests) are only used in atypical cases to rule out or confirm other differential diagnoses and/or to evaluate the structural severity of the disease and presence of subluxation and erosions.
Typical findings on posteroanterior hand radiographs include reduction of the joint space between the trapezium and the first metacarpal, osteophytes, sclerosis and cysts (Figure 1). Other features that may be present are subluxation of the first CMC joint (radial subluxation of the base of the first metacarpal off the trapezium) and central erosions. Peripheral erosions should raise the suspicion for an alternative diagnosis such as rheumatoid or psoriatic arthritis. Although the clinical burden tends to be greater in patients with more severe radiographic disease, imaging should not be used for thumb base OA diagnosis since radiographic OA changes are often asymptomatic.11
Management
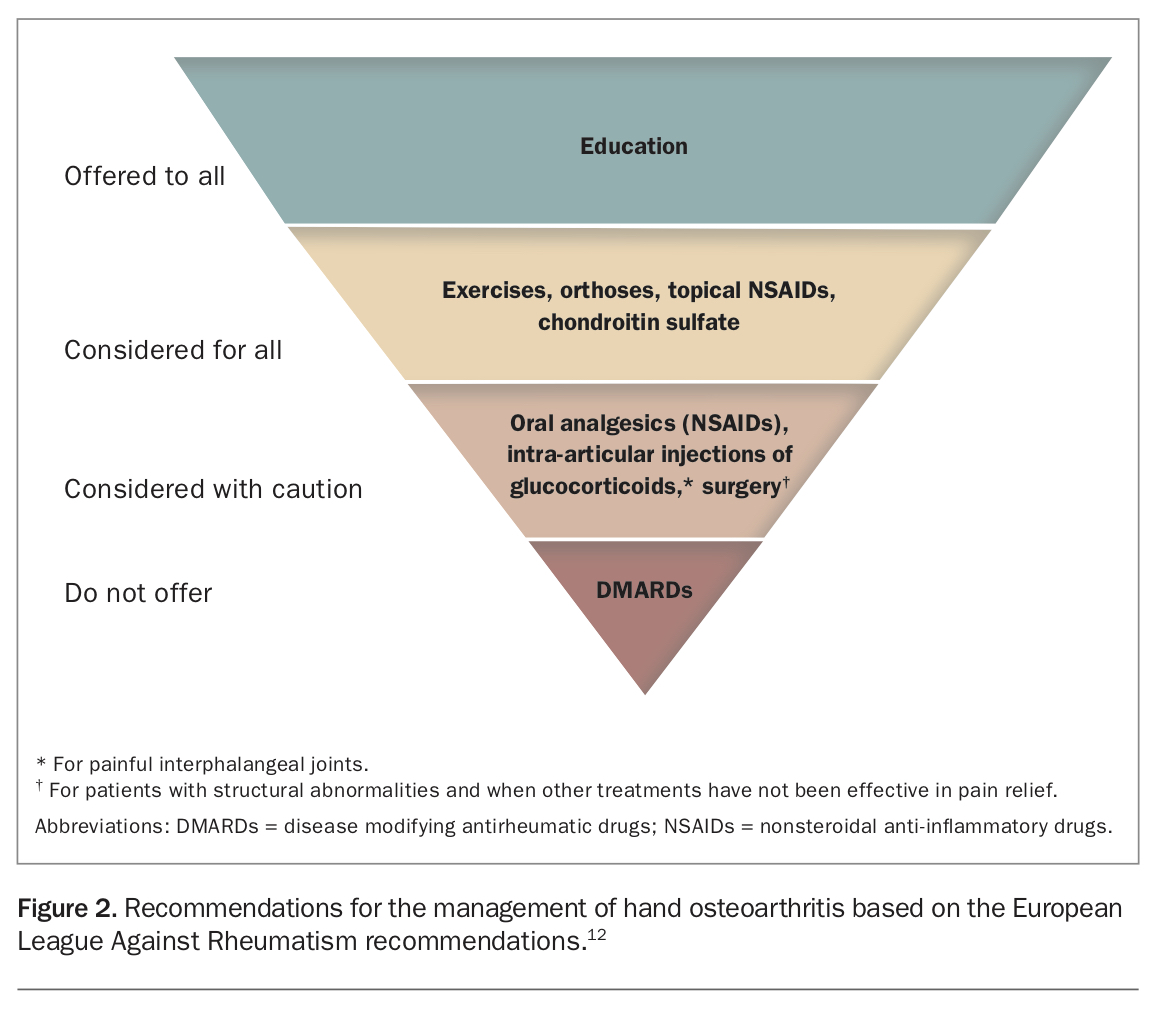
The European League Against Rheumatism (EULAR) released in 2019 updated recommendations for the management of patients with hand OA, including nonpharmacological and pharmacological interventions (Figure 2).12 The cornerstone of treatment includes therapies with good safety profiles and evidence of efficacy. In clinical practice, a combination of therapies is usually used to enhance the clinical effect of the treatment. Education on OA and activity modification to protect the joint from exacerbating activities should be given to all patients. Orthoses (splints) and exercises are also recommended for symptomatic management. Among the pharmacological options, topical NSAIDs are the most used therapies to alleviate pain due to their good safely profile, with the most common side effect being minor skin rashes. We discuss each therapy below in more detail.
{kind=link}
Education and activity modification
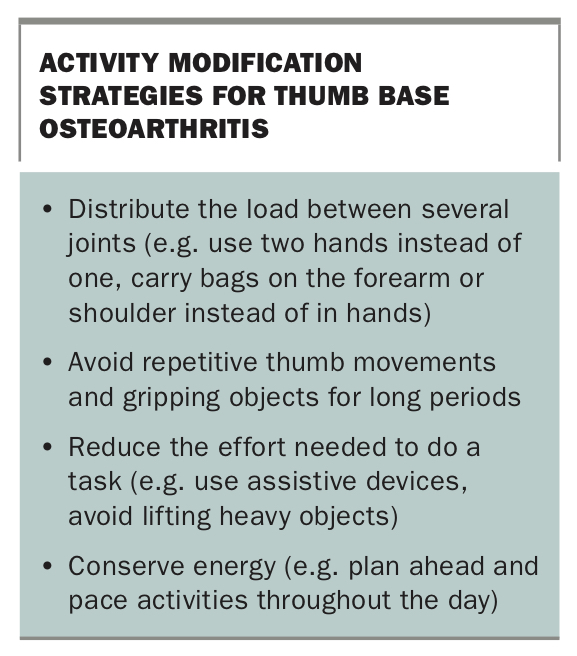
Education and activity modification should be offered to all patients regardless of the severity of their OA and have been shown to be effective for self-management of symptoms.13 Patients should be educated about the nature and course of the disease, as well as the different treatment options and their efficacy. Activity modification (formerly called ‘joint protection’) principles are centred around providing techniques to reduce the microtrauma to articular cartilage and subchondral bone by strengthening surrounding muscles, reducing mechanical stress and improving shock absorption.14 Specific attention should be paid to the positions of the first MCP and IP joints to avoid hyperextension, which would increase the shear forces through the thumb base.15 Examples of activity modification strategies are shown in the Box.
{kind=link}
Assistive devices such as cutlery with ergonomic handles or tools for opening jars can also be of benefit to those with thumb base OA and have been shown to improve activity performance and satisfaction.16 This, in turn, allows patients to complete activities of daily living independently and fosters self-management.
An example of a booklet that can be given to patients to expand on the information given during the medical encounter can be found in Appendix 1 of our previously published paper (https://bmjopen.bmj.com/content/bmjopen/7/1/e014498/DC1/embed/
inline-supplementary-material-1.pdf?download=true).17
Hand exercises
The aim of hand exercises is to improve muscle strength, co-ordination and stability of the thumb joint, and can be considered as part of the treatment regimen for patients with thumb base OA. Strengthening of the first dorsal interossei muscle should be targeted as it has a role in the stability and alignment of the thumb.18 An appropriate exercise program can be prescribed by a hand therapist (physiotherapist or occupational therapist) and might include a range of strengthening exercises such as squeezing a stress ball or tearing sheets of paper and range of motion exercises such as opposing the thumb to each finger.19
Although hand exercises have only shown small beneficial effects on self-reported outcomes such as pain and function, joint stiffness and grip strength, they are relatively safe, resulting in few serious adverse events.20 At present, the optimal exercises and dosage remain undetermined.20
We recommend using the Australian Hand Therapy Association website to find a suitable therapist (www.ahta.com.au/individual-directory).
Splinting
Splints can be worn to support the first CMC joint during aggravating activities, with evidence of beneficial effects on pain and hand function in the medium term (three to 12 months) but not in the short term (up to three months).21 No splint type (custom-made vs prefabricated soft splints) has proven to be superior to another for the general thumb base OA population, although thermoplastic splints that further restrict the first MCP joint might be more effective in stabilising the first CMC joint in individuals with greater joint subluxation.22
NSAIDs
Topical NSAIDs are the preferred option for pain relief in patients with symptoms impairing quality of life, particularly when nonpharmacological options are not sufficient for adequate symptomatic control. Diclofenac 1 or 2%, ibuprofen and piroxicam gel are often used options and can be used in patients with no contraindications, either as needed or in fixed doses, within the maximum daily dosage of each drug.
Oral NSAIDs are reserved for cases when other therapies are not effective. They should be used in the lowest dose and duration possible to avoid cardiovascular, renal and gastrointestinal complications, particularly as most patients with thumb OA are older adults.
Joint injections
Intra-articular injections of glucocorticoids or hyaluronic acid have no role in the management of thumb base OA as they were not superior to placebo in clinical trials.23
Recent hand OA trials
Six-weeks’ treatment with oral prednisone (10 mg) has been recently suggested as a treatment option for management of flare-ups in patients with painful IP OA and presence of inflammatory signs, as it resulted in greater pain relief and increased hand function compared with placebo.24 In contrast, other recent trials have shown no benefits over placebo of disease modifying antirheumatic drugs, including etanercept and adalimumab, for people with erosive hand OA and hydroxychloroquine for symptomatic hand OA.25-28
Surgery
Surgical interventions most often involve trapeziectomy, with or without ligament reconstruction, and are considered for patients with persistent disabling symptoms despite an adequate trial of nonsurgical interventions. Other procedures include arthroplasty, arthrodesis and joint resurfacing, with little evidence supporting one procedure over the others.29
Prognosis
Progression of symptoms and structural abnormalities is usually slow in hand OA, although most patients experience radiographic progression after 10 years.30 Progression of symptoms occurs in about half of patients with hand OA, particularly those with more severe pain and a greater number of joints affected.31
Conclusion and outlook
Thumb base OA is a prevalent disease among the elderly population with a large impact on hand function and overall quality of life. Relieving joint load while enhancing the support to the joint with joint protection measures, splinting and exercises are the foundation of treatment, with topical NSAIDs the first-line pharmacological option for pain relief.
Research in thumb base OA is evolving and a diagnostic criterion for use in trials is underway. Tailoring treatment according to individual features such as the presence of CMC subluxation, erosions and MCP collapse is also a way to potentially optimise outcomes in this population and should be the focus of future research. MT