Healthy joints, healthy heart – what is good for the heart is good for the joints
Dr Lim is a Rheumatologist at Alfred Health; and PhD candidate in the School of Public Health and Preventive Medicine (SPHPM), Monash University, Melbourne.
Dr Wang is Senior Research Fellow in SPHPM, Monash University, Melbourne. Professor Cicuttini is Head of Rheumatology at Alfred Health and Head of Musculoskeletal Unit in SPHPM, Monash University, Melbourne, Vic.
 SERIES EDITOR: Associate Professor Arvin Damodaran BSc, MB BS(Hons), MMedEd, FRACP, representing the Education Training and Workforce Committee of the Australian Rheumatology Association.
SERIES EDITOR: Associate Professor Arvin Damodaran BSc, MB BS(Hons), MMedEd, FRACP, representing the Education Training and Workforce Committee of the Australian Rheumatology Association.
Osteoarthritis
Heart diseases--prevention

Individuals with osteoarthritis have an increased risk of cardiovascular death because of the shared common risk factors. Preventing weight gain, increasing physical activity and addressing cardiovascular risk factors can improve the outcomes of both osteoarthritis and cardiovascular disease in these patients.
Osteoarthritis (OA) is a major cause of pain, disability and healthcare costs.1 It is also associated with an increased mortality rate through the increased risk of cardiovascular disease (CVD).2-5 This provides us with an opportunity to improve outcomes in people with OA by targeting both joint health and heart health in parallel. This review aims to raise clinicians’ awareness of the close link between OA and CVD and provide insights for clinicians to engage populations with joint pain to adopt practical health-related behavioural change, with the potential to improve outcomes of both CVD and OA.
Risk of CVD in populations with osteoarthritis
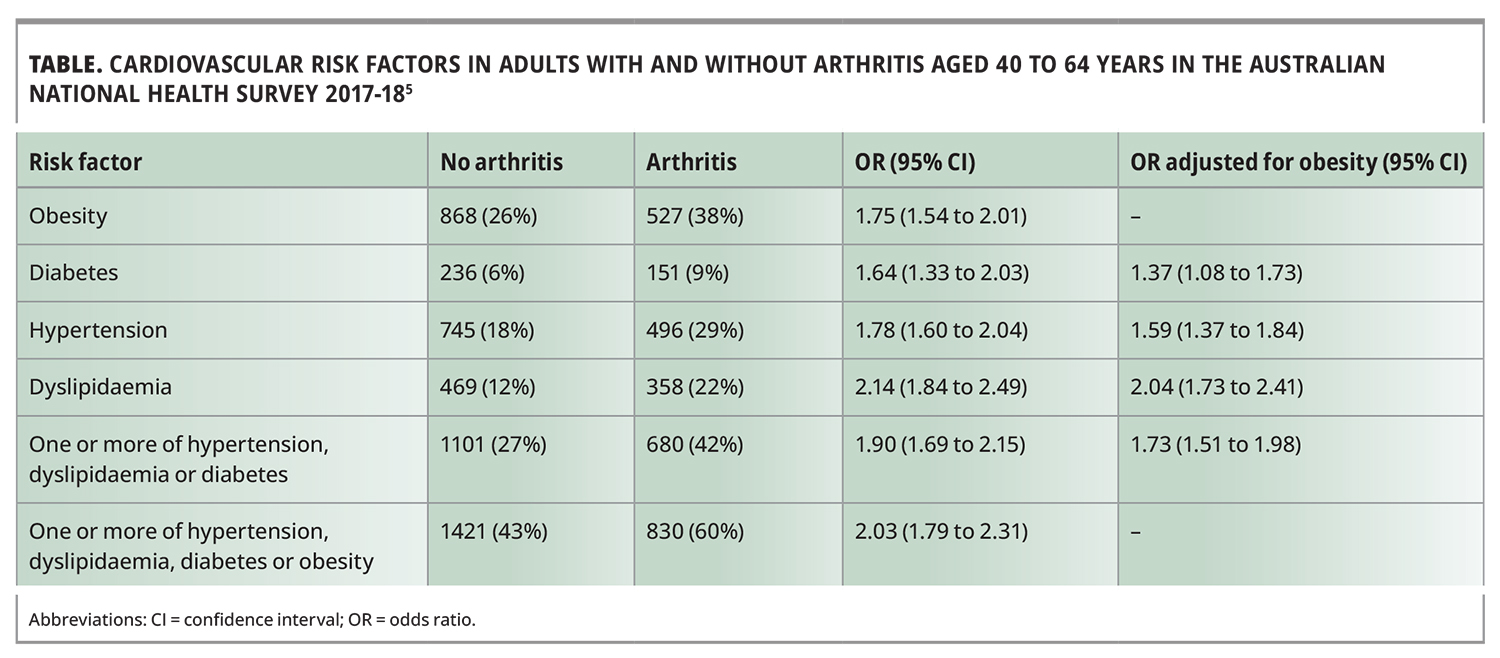
The risk of CVD in people with OA is increased by 24% compared with the general population.4 Individuals with OA are twice as likely to die from CVD, owing to the many shared traditional risk factors, such as dyslipidaemia and hypertension, which are independent of obesity (Table).2-6 They also have a 5.3-fold greater risk of metabolic syndrome than people without OA, regardless of obesity status.7
{kind=link}
Role of vascular pathology in OA pathogenesis
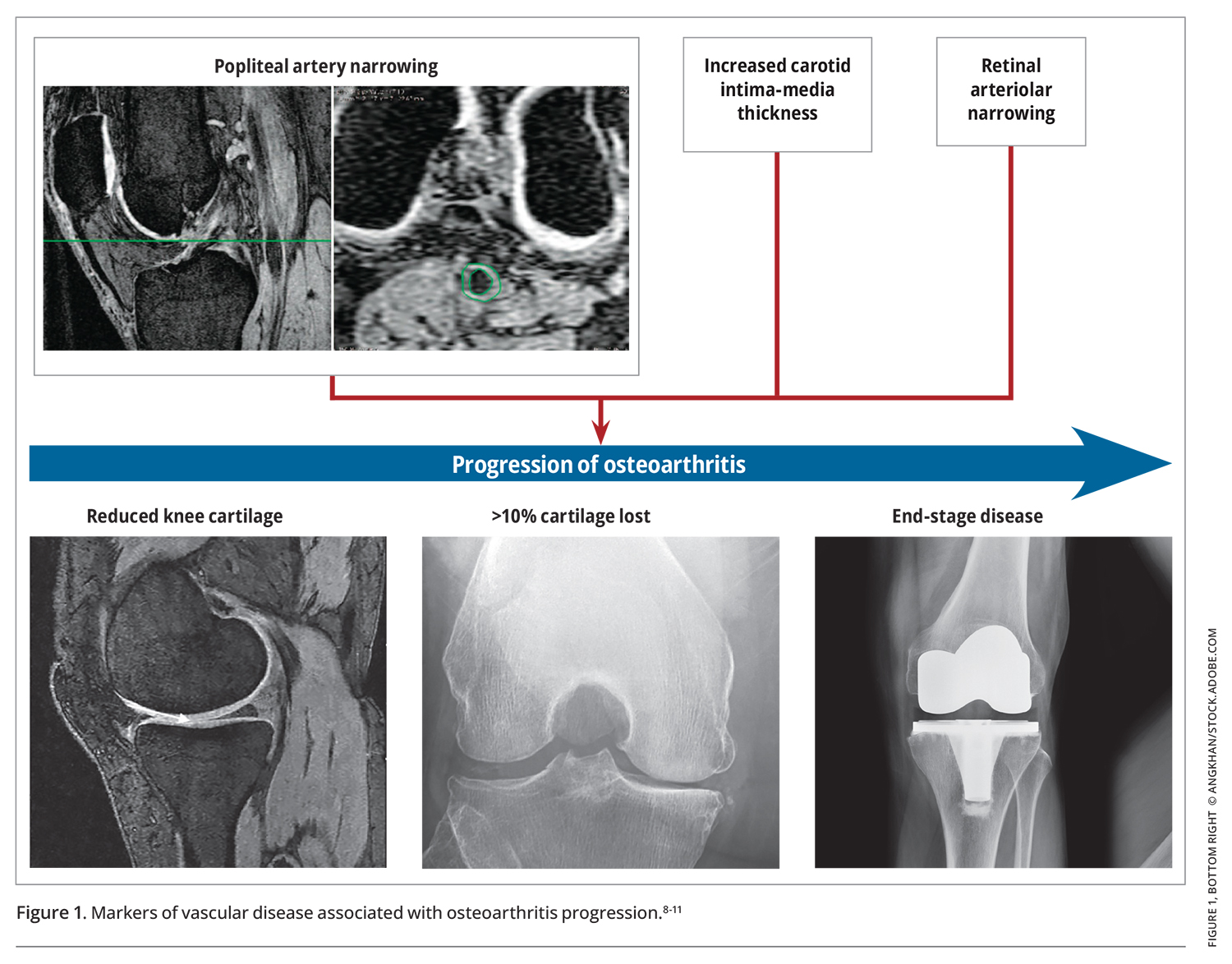
Vascular pathology is associated with joint damage, from preclinical through to end-stage OA (Figure 1).8-11 As an avascular structure, articular cartilage relies on subchondral bone and synovium for nutritional supply. In individuals with vascular pathology indicated by increased artery thickness, a surrogate marker for the burden of atherosclerosis, the blood flow to subchondral bone is compromised. This results in subchondral bone ischaemia and consequently affects articular cartilage.12-15 As such, a healthy vasculature is important to maintain a healthy joint.
{kind=link}
Targeting OA and CVD in parallel
Given the bidirectional relationship between OA and CVD and the many shared risk factors, there is the potential to improve outcomes in both by targeting these conditions in parallel. OA is associated with pain and limited function, causing an ‘immediate’ problem, whereas heart disease is considered more ‘serious’. Joint pain is a common reason for seeking health care and point of contact with health professionals, including GPs, allied health professionals and pharmacists.16 It is the second most common reason for presentations to GPs and the most common reason for attending allied health professionals and for using complementary medicines.17-19
Joint pain can be a teachable moment to target obesity and CVD risk factors
The presence of joint pain offers a potential ‘teachable moment’ for clinicians to target obesity and CVD risk factors, which could further improve adherence and overall patient outcomes in CVD and OA, especially in certain vulnerable populations. Working-age men and people with low socioeconomic status or culturally and linguistically diverse background have a greater prevalence of OA.1 They are also at increased risk of CVD and death.20
Understanding the association between CVD and OA has the potential to improve adherence to OA management
The cornerstone of management of patients with OA is to educate them about the fluctuating nature of symptoms, to manage symptoms when they occur and then to institute ongoing approaches that maintain joint health. Clinical guidelines consistently emphasise the importance of OA education, self-management and self-efficacy programs, including managing obesity and exercising.21-23 These depend on patient participation and adherence, which are likely to be enhanced if patients understand that the likely benefits can impact on both joint and heart health. In the following, we consider the management of obesity, exercise and targeting of cardiovascular risk factors from the viewpoint of patients with joint pain.
Obesity and joint pain
Current management of obesity in people with joint pain
Obesity is the most significant modifiable risk factor for OA symptoms and disease progression, especially at the knee joint.24,25 Weight loss is a major focus in the management of OA.21-23 However, weight loss of 10% of total body weight has only modest effects on pain (standard mean difference, 0.33; 95% confidence interval [CI], 0.17 to 0.48).26-28 This is comparable with the effect of paracetamol (effect size, 0.21; 95% CI, 0.02 to 0.41).29 Weight loss of 10% of total body weight also has a minimal effect on physical function and disease progression in knee and hip OA.26,28,30-35 Even substantial weight loss (up to 20% of total body weight) does not have a clinically significant effect on joint structure.34 This is because significant joint damage has often occurred by the time a person presents with knee symptoms and radiographic evidence of OA, so weight loss has only a modest effect because of the established disease and limited reversibility.36
Importantly, successful weight loss is difficult for most patients to achieve, even when recommended for other chronic diseases such as diabetes and CVD.7,37 Additionally, maintaining any lost weight is difficult, and relapses are common.38,39 The combination of limited effectiveness and the difficulty of achieving and sustaining weight loss have the potential to lead to unrealistic patient goals, where the likelihood of benefits is overstated.
Patients with OA reported dissatisfaction with their weight and emotions of anxiety and disempowerment about achieving weight loss despite being aware of the potential health benefits of weight loss.40-42 Repeated failures to achieve idealistic weight loss outcomes have the potential to demoralise and perpetuate negative thoughts and self-blame that further deter successful weight loss.43,44 This may help explain the poor adherence with the recommendation to lose weight in patients with OA.40,45
Preventing weight gain in people with knee pain and OA
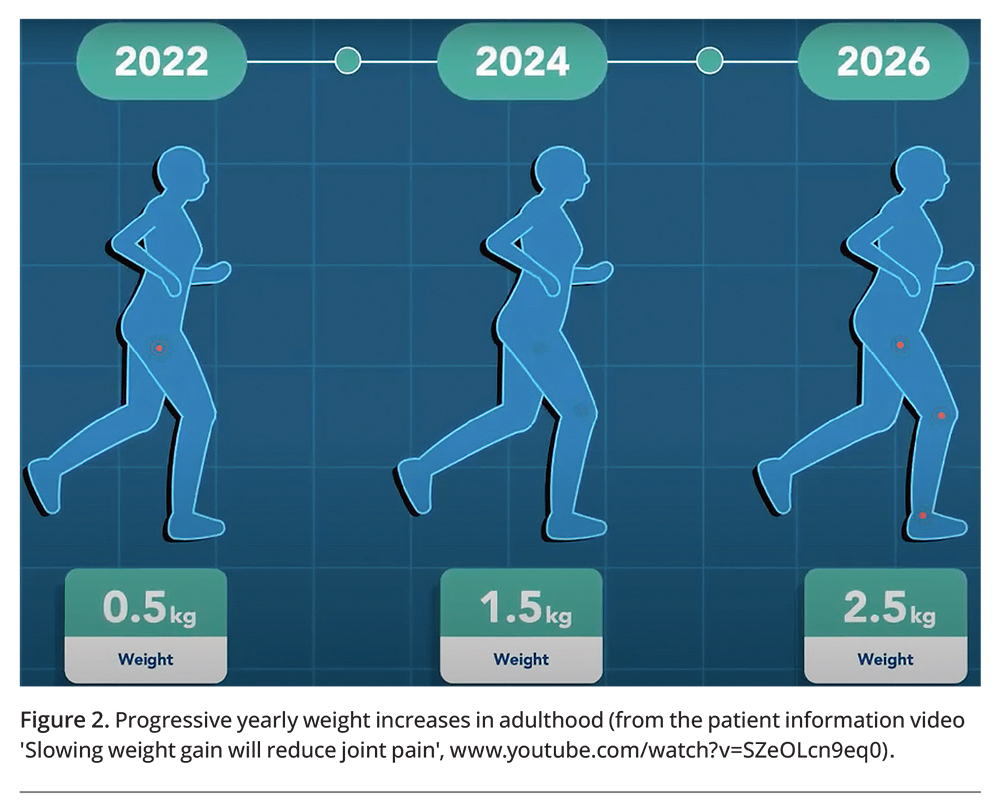
In early to middle adulthood, there is a progressive weight increase of 0.5 to 1 kg annually (Figure 2).46,47 To date, little attention has been paid to this slow, steady increase in weight. Rather, when an individual with a healthy weight presents with knee pain, the approach is usually to provide reassurance, wait until that individual’s weight increases over time and then focus on weight loss.
{kind=link}
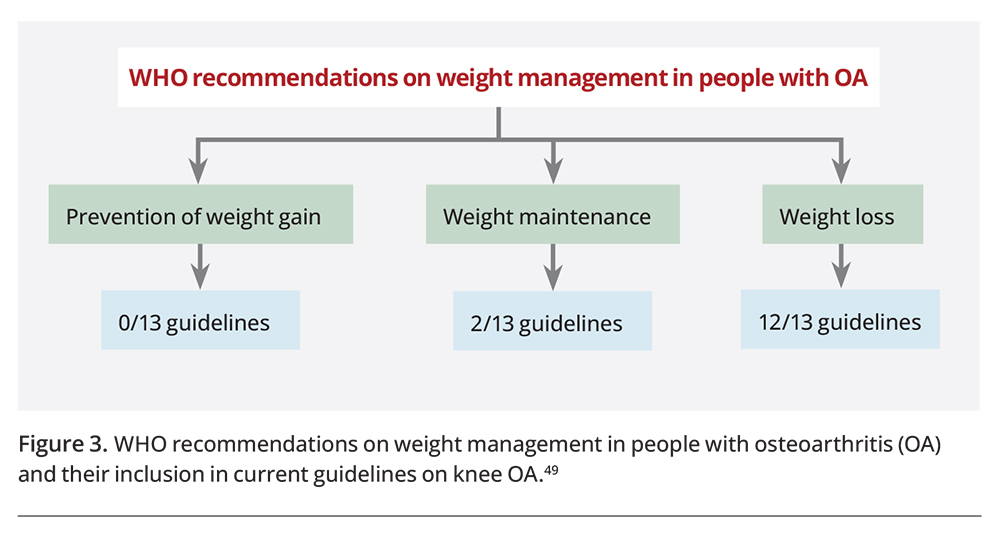
The World Health Organization has identified that management of obesity should encompass weight gain prevention and weight maintenance in addition to promotion of weight loss.48 Yet, weight loss currently remains the focus in addressing obesity in patients with OA, with minimal attention to preventing weight gain, as shown in current international guidelines on OA management (Figure 3).49
{kind=link}
A recent Australian study showed that up to 36% of knee replacements could be avoided if overweight and obesity were prevented, whereas 20% of knee replacements could be avoided if people with overweight or obesity were to lose weight equivalent to moving down one category of body mass index.50
Feasibility of preventing weight gain
A recent meta-analysis showed that low intensity weight-related behaviour interventions, including diet and physical activity that result in small energy deficits, were effective in preventing weight gain.51 They were most effective in non-obese populations.51 The small estimated cumulative energy imbalance was about 30 kJ per day, which is comparable to reducing intake by half a medium-sized apple a week or a serve of dark chocolate a fortnight, or increasing physical activity by 10 minutes of extra walking a week or five minutes of extra cycling a week.52,53
This small modification in energy balance is potentially more feasible than the large energy changes required to lose weight. It should be considered when people present with joint pain, irrespective of their weight. Clinicians can provide patient-focused advice for minor lifestyle changes targeting this small cumulative positive energy imbalance, which are more pragmatic, achievable and sustainable in daily life, aiming to prevent the insidious development of obesity over time.54,55
Exercises for joint pain
An exercise program is central to managing joint pain at weight-bearing joints such as the knee.21 This program is important not only to maintain a healthy joint but also when episodes of pain occur. The exercise program can be tailored to pain levels, increasing as joint pain improves. There is a lack of evidence to support any specific type of exercise program in managing joint pain at the knee. Rather, there is evidence that any land-based exercise program is effective, providing the opportunity to cater to individual patient preferences.21,56-58 Additionally, the mode of delivery is less important than patient engagement in exercises, whether they be self-directed or supervised.59
Joint pain as a reminder to have a heart check
In Australia, it is recommended that people aged 45 years and over undergo screening for CVD.60 However, this requires initiative from asymptomatic individuals to undergo screening. The significant burden of CVD in Australia is due to untreated or undertreated risk factors: hypertension for 48% and dyslipidaemia for 21% of CVD disease burden.61 Thus, presentation with joint pain can act as a reminder to do a heart health check and institute any required management.
Importantly, not only is the management of CVD risk factors important to reduce CVD and cardiovascular deaths in people with OA, but it is also likely to improve joint health. For example, we recently showed that, although atorvastatin (40 mg once daily) did not significantly slow knee cartilage loss over two years in patients with symptomatic knee OA compared with placebo, it reduced joint damage in those with milder OA.62 This, together with data from cohort studies, suggests that the widespread use of statins in the management of CVD may reduce the burden of knee OA.63,64
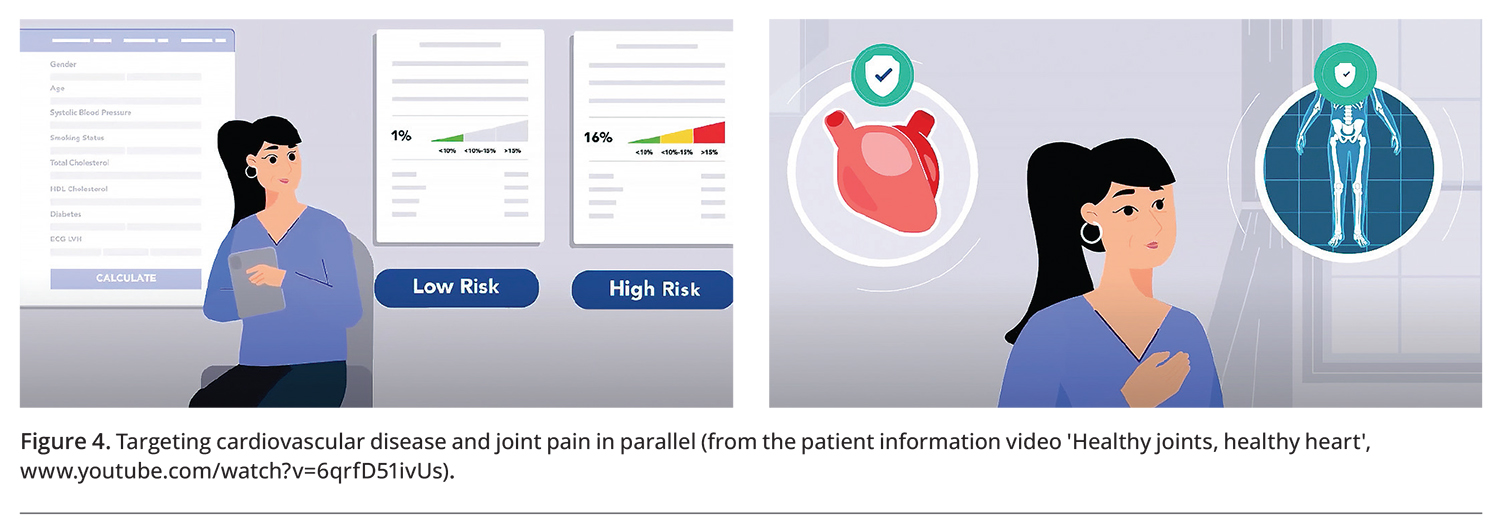
A simple clinical approach
Ideally, when a person presents with joint pain, the clinician can use this as a teachable moment to raise awareness of the association between OA and CVD and to empower patients with OA to make small, practical and sustainable lifestyle changes. These include better management of cardiovascular risk factors and prevention of weight gain (Figure 4). These changes are also likely to improve joint symptoms, as evidence shows that weight gain is associated with increased joint pain, whereas preventing weight gain reduces knee pain.27,59,65
{kind=link}
To assist with this education, we have developed a series of videos on weight management, heart health and osteoarthritis for use by clinicians and consumers (Box 1). Key practice points for GPs treating patients with joint pain are summarised in Box 2.
{kind=link}
{kind=link}
Conclusion
Given the close link between OA and CVD, presentation with joint pain is a golden opportunity for clinicians to manage both OA and CVD in parallel. By targeting the shared risk factors in both conditions, including preventing weight gain and addressing the hidden burden of CVD risk, there is a real potential to improve outcomes in both OA and CVD. MT
COMPETING INTERESTS: None.
Acknowledgements
Dr Lim is the recipient of NHMRC Clinical Postgraduate Scholarship and Royal Australasian College of Physicians Woolcock Scholarship. Dr Wang is the recipient of NHMRC Translating Research into Practice Fellowship. Professor Cicuttini is the recipient of NHMRC Investigator Grant. The funders of the study had no role in the study design and conduct of the study; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.