Rich with potential: the role of platelet-rich plasma in osteoarthritis and tendinopathy

Increasingly, platelet-rich plasma injections are being used for patients with osteoarthritis and tendinopathy. GPs play an important role in helping patients understand their treatment options and in managing expectations about emerging treatments such as this musculoskeletal ‘biological’ therapy.
In Australia, arthritis and other musculoskeletal conditions account for 13% of the total disease burden; musculoskeletal disease is ranked fourth among disease groups for causes of disability.1 Osteoarthritis affects 2.2 million (9.3% or one in 11 people) nationally and is the eighth most frequently managed problem in general practice.2 As there is currently no cure, treatments are aimed at reducing pain and improving function.
Evidence-based management guidelines for osteoarthritis identify patient education, exercise and weight loss as key treatments. Generally, imaging is not needed for diagnosis. Ineffective treatments such as arthroscopy and opioids are actively discouraged, and appropriate candidates for surgical referral and joint replacement are generally patients who are considered to have end-stage disease, and are preferably in an older age group so revision is less likely to be required.3 Many people with osteoarthritis live with the disease for 20 to 30 years, and it is difficult to manage patients who fall into this ‘treatment gap’ – that is, those who have symptomatic osteoarthritis but are too young for a joint replacement.4,5 Patients invariably try simple analgesia (such as paracetamol) or NSAIDs, which have low efficacy and risks of gastrointestinal and renal side effects.6,7 Corticosteroid injections are widely used, even though their duration of action is short term and repeated injections cause more rapid loss of cartilage volume.7 Similar long-term management concerns exist with chronic tendinopathies – most particularly in gluteal tendinopathy, which occurs in up to 10% of women over 60 years of age.
Platelet-rich plasma (PRP) injections are appealing because they are safe, minimally invasive and may have the potential to delay the need for surgical intervention.
Since PRP therapy was covered in Medicine Today as an emerging treatment in 2011,8 its role in the treatment of osteoarthritis and tendinopathy has changed. This article provides an update on the clinical experience of PRP and the implications of the current evidence base with reference to primary care clinical practice guidelines. A summary is provided in Box 1.
{kind=link}
What is platelet-rich plasma?
Made by the centrifugation of whole blood, PRP is defined as plasma with an increased concentration of platelets, and potentially white blood cells, compared with whole blood. Growth factors released from alpha granules in platelets and from white blood cells in PRP have the ability to regulate cell migration and proliferation and assist with the regulation of tissue repair through chemotaxis, cell proliferation, differentiation and angiogenesis. These include platelet-derived growth factor (PDGF), transforming growth factor beta (TGF-β), insulin-like growth factor (IGF), vascular endothelial growth factor (VEGF) and epidermal growth factor (EGF). In general, the growth factor concentration increases as the cell and platelet concentrations increase. Cytokines, which are immunomodulatory proteins such as the interleukins (IL-1, IL-4, IL-6, IL-10), contribute to the mechanism of action of PRP.9
PRP preparation methods vary widely, and the resultant concentrates can have quite different biological activity and potentially different therapeutic results relating to composition. In musculoskeletal applications, two common types of PRP are used: leucocyte-rich (LR-PRP) and leucocyte-poor (LP-PRP). In our practice, we prepare PRP by taking between 10 and 60 mL of blood, drawn into a syringe using a needle or cannula from a cubital vein using an arm tourniquet. Anticoagulants are used to coat the syringe to prevent platelet coagulation, which would reduce yield. The whole blood is spun using a centrifugation process to separate the blood into homogeneous layers: red cell concentrate, buffy coat layer and plasma. The platelet-containing plasma and sometimes the buffy coat layer (containing the white blood cells) are decanted from the original tube manually or automatically and spun a second time – this separates the plasma-rich fraction, which is then used for treatment (with the white blood cells included if these are desired). PRP preparation can be done manually, although using a commercially available kit will generally achieve more consistent preparations.
As PRP injections are autologous, they carry a low risk of an immune reaction. The potential for infection has been shown to be low, with white blood cells acting as antimicrobial agents (note that platelets also have this property).10,11 Some patients have short-term post-treatment soreness in the local treatment site, which may relate to inflammatory effects from white blood cells, particularly neutrophils, and the resultant cytokine release. Increasingly, injections are being performed under ultrasound guidance to increase accuracy of placement, and this is particularly important when treating tendinopathies.
Use of PRP in osteoarthritis
Evidence of efficacy
The latest edition of The Royal Australian College of General Practitioners’ Guideline for the Management of Knee and Hip Osteoarthritis was published in 2018.12 Only four low-quality randomised controlled trials of PRP were assessed at that time, and these were at serious risk of bias and inconsistency and were generally small in size. As a result, the guidelines state that the authors were ‘unable to recommend either for or against the use of PRP injection for people with knee and/or hip osteoarthritis’.12
The most recent systematic review and meta-analysis of PRP therapy in osteoarthritis, published earlier this year, analysed 21 randomised controlled trials that involved a total of 1743 patients with knee osteoarthritis.13 The meta-analysis found PRP to be superior to both intra-articular saline and corticosteroid injections in reducing pain in patients with knee osteoarthritis. This confirmed the findings of a meta-analysis published in 2020 that involved 1608 patients with knee osteoarthritis and found PRP to be superior to hyaluronic acid.14 Both systematic reviews concluded that recent trials showed PRP is of clinical benefit in reducing knee pain from osteoarthritis, but the reviewers commented that it had not been possible to establish whether leucocyte-rich or leucocyte-poor concentrates were better.
This evidence substantiates the use of PRP for symptom relief in knee osteoarthritis. It may also work in other large and small synovial joints; however, evidence has not yet been established.
Clinical implications
When no recommendation is made in clinical practice guidelines, clinicians may be flexible in their decision-making, being alert to new published evidence that clarifies the balance of benefit and harm and taking patient preference into account.15
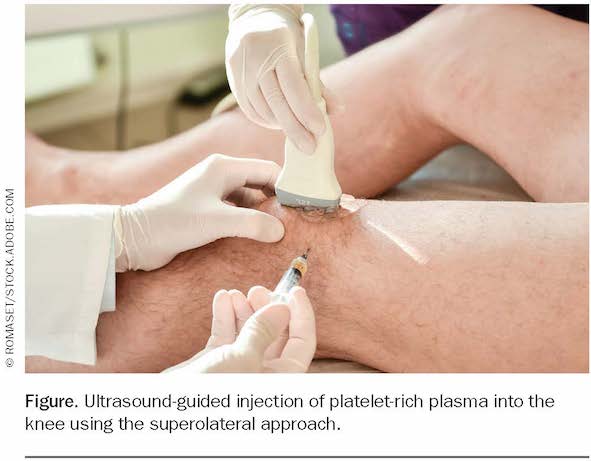
Recent evidence indicates that PRP injections are safe and efficacious for patients with knee osteoarthritis who do not respond to conventional treatments and are most likely to work well for patients who have mild to moderate osteoarthritis (Figure). Benefits are related to pain and functional improvements, as there is no evidence that PRP influences disease progression. There is a published protocol for a ‘living’ systematic review of PRP injections for knee osteoarthritis, to be updated monthly, incorporating relevant high-quality evidence as it emerges (see https://doi.org/10.1002/14651858.CD013341).16 As trials continue, this is a useful reference point.
{kind=link}
A case study of a typical patient with knee osteoarthritis is presented in Box 2.
{kind=link}
Use of PRP in tendinopathy
Evidence of efficacy
Tendinopathy is a common reason for patients to present to their GP, with frequently affected sites including the rotator cuff and elbow extensors as well as the gluteal, Achilles and patellar tendons. For 90% of patients, it is expected that the condition will resolve with appropriate load management and conservative treatment. However, 10% of patients have persistent symptoms, and these patients are often considered for surgical intervention or, more recently, PRP injections.17
The first small clinical trial of PRP in tendinopathy, published in 2006, showed improvement in tennis elbow pain.18 More recently (2017), a systematic review and meta-analysis of PRP in all tendinopathies that included 18 studies and involved 1066 participants found good evidence that PRP (particularly LR-PRP) improved pain and functional outcomes in tendinopathy.19 Subsequent systematic reviews for specific tendons have identified good results for pain and function for PRP therapy in tennis elbow,20 rotator cuff pathology,21 and gluteal tendinopathy.22
To date, Achilles tendinopathy and patellar tendinopathy have not been shown to respond to PRP.23,24 The number of studies in this area is limited and they are often difficult to interpret, with heterogeneity of pathology and variability in the type of PRP. There is no clearly identified reason for the apparent lack of response in the Achilles and patellar tendons, but one possible explanation is that these do not respond in the same way because they are different anatomically, with a more cylindrical anatomy and neurovascular bundle. It is also possible that studies on these tendons have been done in small cohorts with insufficient sample sizes to demonstrate effects.
Clinical implications
PRP injections may be considered for patients with tendinopathy who have failed conventional treatments and exhausted other options. Patient selection is an important consideration. For gluteal tendinopathy, tennis elbow and rotator cuff tendinopathies, the evidence suggests the use of a single injection and a peppering technique intratendinously into the affected area, generally under ultrasound guidance. Local anaesthetic (1 to 2 mL) should be injected before the PRP injection. These technical considerations help to avoid the potential for microtrauma from repeated injections since there is evidence for single rather than multiple injections. There is some evidence that LR-PRP may be more effective in tendinopathies compared with LP-PRP. However, there is a clear need for further research regarding the use of PRP injections in all types of tendinopathy.
Conclusion
The use of biologicals that target growth factors such as adalimumab (a TNF blocker) has become commonplace in rheumatology. In the musculoskeletal area, the emergent growth factor technology in biological therapies such as PRP now has established safety. The efficacy for PRP in osteoarthritis is sufficiently strong to support recommending PRP for patients with mild to moderate osteoarthritis who have not responded to conservative treatments and are not ready for joint replacement surgery. Tendinopathies of the gluteal, tennis elbow and rotator cuff tendons that fail to respond to conservative care may be managed using PRP therapy, but prescribers and patients should be aware that the evidence for use of PRP therapy in tendinopathy and osteoarthritis of other joints is still limited. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.