Pneumococcal vaccinations in Australia: current recommendations and beyond

Pneumococcal vaccines are effective in protecting against disease. They are recommended in Australia for young children, older people, Indigenous Australians and those at increased risk of disease, and funded under the National Immunisation Program for many of these groups. Clinicians should be aware of the available vaccine types and the current recommendations to effectively advise about and administer vaccines to those who will benefit most while also being abreast of the latest developments in this field.
Invasive pneumococcal disease (IPD) is the severe form of pneumococcal disease and is a nationally notifiable disease in Australia. Although rates of infection have been low during the COVID-19 pandemic, they are predicted to increase with relaxation of COVID-19 restrictions, including the resumption of international travel. In Australia, pneumococcal vaccination is recommended for young children, older people, Aboriginal and Torres Strait Islander Australians and at-risk cohorts, and is funded for most of these groups under the National Immunisation Program (NIP). This article gives an overview of the pneumococcal vaccines available and highlights the recent changes to the pneumococcal vaccination schedule.
Pneumococcal disease
Pneumococcal disease is caused by the encapsulated Gram-positive coccus Streptococcus pneumoniae, with pneumococcal disease responsible for 14% of deaths in children under five years of age in 2019 globally.1 IPD is characterised by the presence of S. pneumoniae in sterile body sites, including blood and cerebrospinal, pleural, peritoneal and joint fluid, causing severe disease.2 Noninvasive pneumococcal disease typically presents as localised mucosal infections that are usually less clinically serious and more common than IPD, such as otitis media, often seen in children.3 The most common adult presentation of IPD is bacteraemic pneumonia; however, most community-acquired pneumococcal pneumonia cases are noninvasive.4 In most cases,
S. pneumoniae resides in the nasopharynx, leading to asymptomatic carriage, which can be a precursor to disease and an important transmission factor.5 One hundred unique pneumococcal serotypes have been identified so far based on the polysaccharide capsule of S. pneumoniae, which is an important virulence factor, with vaccines targeting serotypes that commonly cause disease.6
Pneumococcal disease in Australia
IPD became nationally notifiable in 2001, with 2028 notifications in 2018, 14% of which were in children aged younger than five years and 37% in adults 65 years or older.7 Notification rates are consistently higher among Indigenous Australians than non-Indigenous Australians.8 Internationally, rates of IPD have decreased, both in adults and children, during the COVID-19 pandemic mainly due to public health restrictions resulting in reduced circulation of viruses associated with IPD. The reduced testing capacity and healthcare presentations may also have contributed to this observed decline.9,10 However, trends showing surges in respiratory virus infections linked to the recent relaxation of COVID-19 restrictions raise concerns of the potential for increased pneumococcal coinfections, including increases in IPD cases as well as the re-emergence of certain pneumococcal serotypes.11,12
Pneumococcal vaccine types
Pneumococcal conjugate vaccines (PCVs) involve the conjugation of multiple selected pneumococcal polysaccharides to a protein. This protein carrier conjugation converts the pneumococcus polysaccharide to a T cell-dependent antigen that induces immune memory and results in a robust, high-quality immune response, sufficient to prevent pneumococcal disease, including in infants, together with the ability to reduce carriage of the vaccine serotypes.13,14 In comparison, pneumococcal polysaccharide vaccines (PPVs) generate antibodies against pneumococcal disease alone, producing relatively short-lived immunity and are considered to have no effect on pneumococcal carriage.15 Pneumococcal vaccines currently available in Australia are 13-valent pneumococcal conjugate vaccine (13vPCV) and 23-valent pneumococcal polysaccharide vaccine (23vPPV).
Current pneumococcal vaccine recommendations
In Australia, all adults aged 70 years and older are offered a dose of the 13vPCV for free through the NIP.16 For children, the NIP schedule is three doses of 13vPCV at ages 2, 4 and 12 months (2+1 schedule).17 Aboriginal and Torres Strait Islander people and those with certain underlying risk conditions are recommended adult vaccine doses at a younger age and additional doses of pneumococcal vaccines, including 23vPPV, because of their increased risk for pneumococcal disease, with a considerable proportion caused by extra serotypes in 23vPPV. The Figure summarises current pneumococcal vaccine recommendations for each target population.
For children who are at increased risk of pneumococcal disease, four doses of 13vPCV at two, four, six and 12 months of age (3+1 schedule) are recommended. Children and infants can receive 13vPCV coadministered with other routine childhood vaccines, including inactivated influenza vaccines. However, parents and caregivers should be made aware of a small increased risk of fever when 13vPCV and influenza vaccinations are given together. The 13vPCV should not be coadministered with Menactra, the quadrivalent meningococcal ACWY vaccine, in children and adults because of possible immune response interference. It is preferred that 13vPCV be administered first, followed by Menactra at least four weeks later. Either 13vPCV or 23vPPV can be coadministered with live attenuated herpes zoster vaccine (Zostavax) and inactivated influenza vaccines in adults.16
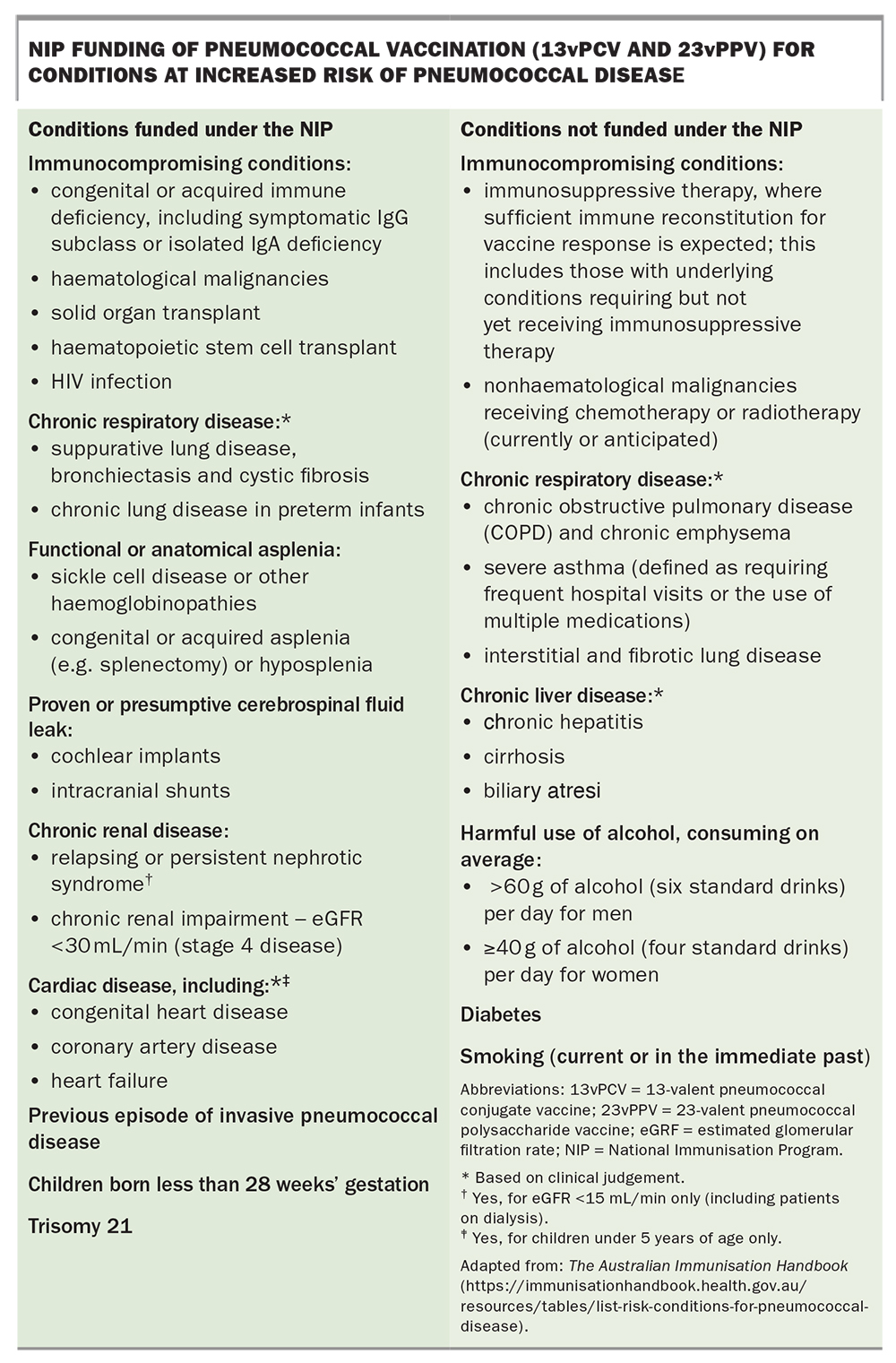
People with conditions that put them at increased risk of pneumococcal infection are also recommended to receive the pneumococcal vaccine. Vaccination for people with most (but not all) of these high-risk conditions is funded under the NIP and are summarised in the Box. All current recommendations by the Australian Technical Advisory Group on Immunisation (ATAGI) for pneumococcal vaccines are published in the Australian Immunisation Handbook (https://immunisationhandbook.health.gov.au).16
{kind=link}
Changes to the pneumococcal vaccination program
The current recommendations and funding of 13vPCV for adults were introduced in July 2020.18 This updated schedule no longer recommends the 23vPPV for healthy adults aged 70 years or older, and instead recommends a single dose of 13vPCV for this cohort. Under the updated recommendations, the 23vPPV is reserved for Aboriginal and Torres Strait Islander adults aged 50 years or older and adults with underlying risk conditions only, following a dose of 13vPCV in both. The key evidence leading to the decision to use 13vPCV in adults came from the results of a randomised controlled trial that showed 13vPCV was effective against all pneumococcal pneumonia, including less severe but more common nonbacteraemic pneumonia.19 Serotype epidemiology of pneumococcal disease in adults in Australia showed that most disease from the additional serotypes contained in 23vPPV occurred in Indigenous adults and individuals with pre-existing risk conditions; therefore, 23vPPV doses are now offered to those groups only.
Alongside this change, two doses of 23vPPV were added to the existing recommended 3+1 schedule of 13vPC for Aboriginal children living in the Northern territory, Queensland, South Australia and Western Australia to provide broader serotype protection. In 2018, the PCV schedule was changed, from the long-standing 3+0 to the current 2+1, for most children in Australia to address the waning immunity from the second year of life.20,21 Early assessment of this change shows that the expected reduction in breakthrough cases of IPD in older children is occurring.22
What's next for pneumococcal vaccination?
As current pneumococcal vaccines target specific serotypes, infections with certain non-vaccine serotypes of S. pneumoniae may occur when those serotypes have a competitive advantage in nasopharyngeal carriage, leading to some ‘serotype replacement’ disease.23 The development of vaccines with expanded serotypes (known as higher valency vaccines) aims to maintain and optimise pneumococcal disease prevention by covering these emerging and common residual serotypes.
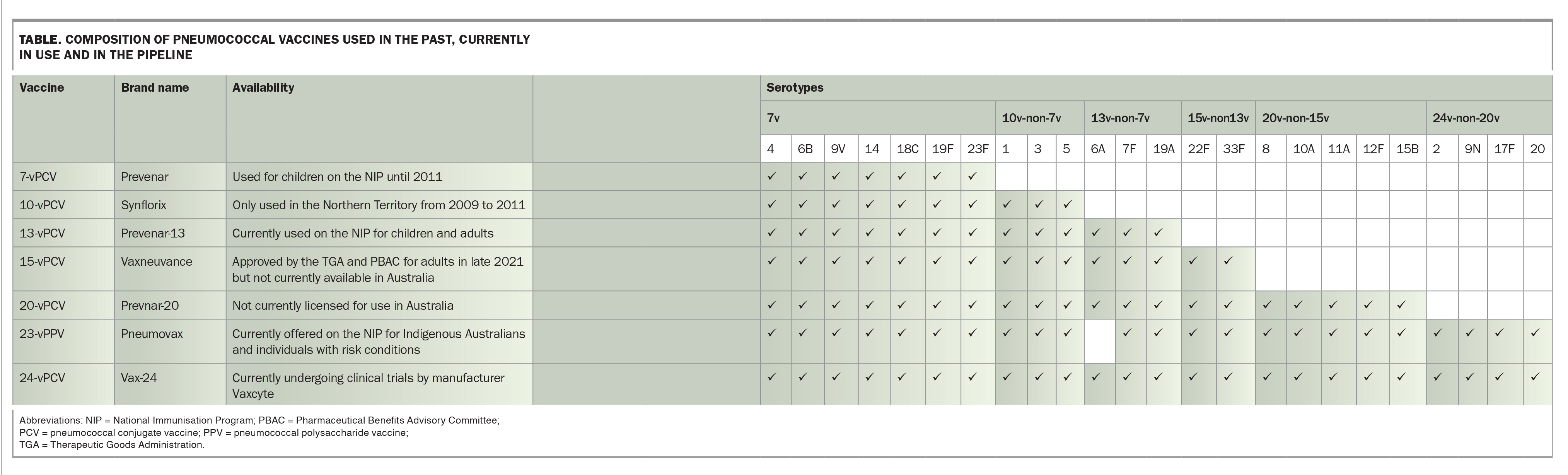
Previous pneumococcal conjugate vaccines used in Australia have been superseded by vaccines with an expanded serotype spectrum (e.g. 13vPCV replacing 7vPCV in 2011).24 Two PCVs with expanded serotypes, Vaxneuvance (a 15-valent PCV by Merck) and PREVNAR20 (a 20-valent PCV by Pfizer) have become commercially available overseas and are being considered for use in several countries, first in adults and then in children, aligning with clinical development of these vaccines.25 In late 2021, the TGA licensed the use of 15vPCV for adults in Australia and the Pharmaceutical Benefits Advisory Committee recommended listing of 15vPCV on the NIP for the adult populations currently offered NIP-funded 13vPCV.26
The Table summarises important details of pneumococcal vaccines previously used in Australia, those currently part of the NIP and the higher valency vaccines currently available or under development. In the US, 15vPCV has been recently approved by the Food and Drug Administration and recommended by the Advisory Committee on Immunization Practices for use in children and adults interchangeably with 13vPCV, and 20vPCV for use in adults as an alternative for 13vPCV and 23vPPV, which is the existing recommendation.27,28
{kind=link}
Conclusion
In Australia, the recommendations of pneumococcal vaccination are based on vaccine characteristics and individuals’ IPD risk factors, including age, Indigenous status, state or territory of residence, the presence of risk factors and previous pneumococcal vaccination history. It is important for immunisation providers to be aware of the differences between pneumococcal vaccine types, their dose schedules and approved population groups, as well as changes to recommendations, with potential inclusion of new vaccines. Understanding the difference between pneumococcal vaccines and potential changes with future vaccine approvals will provide easier implementation of updated pneumococcal vaccination and patient recommendation practices. MT
COMPETING INTERESTS: Dr Jayasinghe holds an emerging leadership investigator grant from the NHMRC. Dr Norman: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.