Altitude illness: back on the horizon

As Australia’s international borders reopen, people will again be making plans for trips to high altitude destinations. GPs are well placed to advise intending travellers about the risks of altitude illness and appropriate mitigation strategies.
Altitude illness is common among unacclimatised individuals travelling to altitudes over 2500 m. With increasing numbers of tourists travelling to high altitude environments globally, many are being exposed to potentially significant risks. There are tour operators in Australia that offer treks to Nepal, South America and Mt Kilimanjaro, where hiking to extreme altitudes (defined as >5500 m) can be achieved without any technical climbing experience, making these expeditions readily available to the general population. In addition, some international ski resorts expose travellers to altitudes of almost 4000 m (e.g. Breckenridge, Zermatt, Chamonix, Aspen Snowmass), which can be underestimated.
It is important that intending travellers have information to help them understand the risks associated with travel to high altitudes and the support to mitigate these risks in advance. Many will seek advice from their GP and travel clinics regarding travel vaccinations, which presents an opportunity to discuss these concerns and the role of prophylactic medications for altitude sickness as well as for ensuring individuals are medically fit to participate in their planned activities. The Wilderness Medical Society Clinical Practice Guidelines for the Prevention and Treatment of Acute Altitude Illness, which were updated in 2019, provide a useful online resource for clinicians.1
Altitude physiology
The defining feature of high altitude is the reduction in the partial pressure of oxygen when compared to sea level. This means that the air being breathed at altitude is still composed of 21% oxygen, but the absolute number of oxygen molecules in each breath is less because the barometric air pressure is lower.
The reduction in the partial pressure of oxygen, which becomes exponentially lower with increasing altitude, drives all of the physiological adaptions to altitude, which will not be covered in detail here. Broadly speaking, when individuals are exposed to high altitude, they experience short term physiological changes to cope with the reduced partial pressure of oxygen and longer term changes (continuing over some weeks) that represent acclimatisation. The extent of these short term changes varies between individuals and is mainly dependent on the rate of ascent and maximum altitude reached, rather than level of fitness or age.2
The first physiological change to altitude exposure is an increase in respiratory rate to meet oxygen demands. This leads to carbon dioxide being blown off, causing a metabolic alkalosis and excretion of bicarbonate via the kidneys, resulting in diuresis. In addition, lower oxygen content in the blood stimulates increased sympathetic nerve activity, resulting in increased heart rate, cardiac output and blood pressure.
Altitude illness
The term ‘altitude illness’ refers to a number of diagnoses, including high altitude headache and acute mountain sickness (AMS) as well as the more severe conditions of high altitude cerebral oedema (HACE) and high altitude pulmonary oedema (HAPE).3 High altitude headache, AMS and HACE can be considered disorders of increasing severity within a spectrum, whereas HAPE has some separate pathophysiological changes. The risk factors consistently associated with the development of all forms of altitude illness are fast rate of ascent and absolute altitude reached.1,4 Chronic mountain sickness is a condition that typically affects people living for long periods at high altitude and will not be covered here.
Acute mountain sickness and high altitude cerebral oedema
Cerebral blood flow is very sensitive to hypoxia, and in the presence of low arterial oxygen concentration vasodilation takes place. This leads to a degree of cerebral oedema, which has been demonstrated in those travelling to altitude.4 Cerebral oedema of varying degrees is thought to largely account for high altitude headache (which occurs in up to 80% of travellers who ascend over 3000 m), through to AMS and finally to HACE, which is fatal if left untreated.4
AMS is common and presents as nonspecific symptoms that range in severity from mild through to severe. The condition is defined as the presence of headache plus one or more of the following symptoms in an individual who has recently arrived at altitude: gastrointestinal upset (anorexia, nausea or vomiting), sleep disturbance, dizziness and fatigue.3 Patients in whom AMS becomes more severe and progresses to HACE display evidence of increasing neurological disturbance, such as ataxia, confusion and stupor, and eventually coma and death from brainstem herniation if left untreated.
Descent is the single most effective strategy for managing AMS and HACE. The amount of descent required for symptomatic relief varies and can be as little as 300 m to 1000 m.1 If symptoms are mild then it may be more appropriate to rest and allow symptoms to settle before trialling further ascent. These decisions will be affected by the expedition, the medical support available and the local facilities. In addition, there is evidence for use of supplemental oxygen, dexamethasone (oral or intramuscular) and acetazolamide in treatment.1
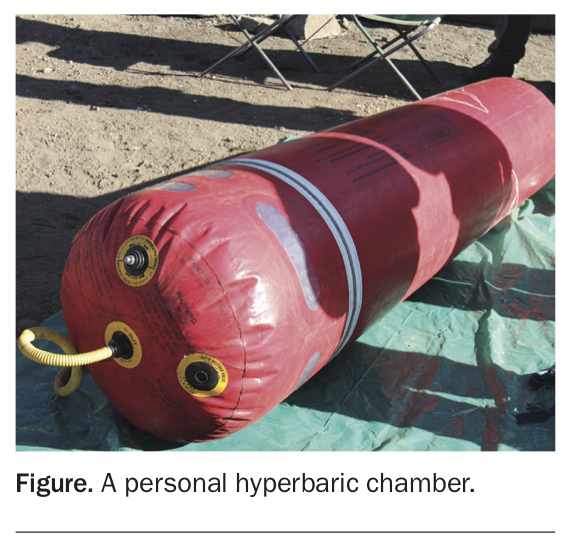
A personal hyperbaric chamber (e.g. Gamow bag) offers a temporary solution if descent is temporarily unfeasible and supplemental oxygen is not available. This is an inflatable chamber for a single person that typically relies on a manual pump to create and maintain a raised interior air pressure, increasing the partial pressure of oxygen (Figure). Personal hyperbaric chambers are carried by some tour operators and can be effective; however, descent should not be delayed for the use of these.
{kind=link}
AMS is common on typical tourist treks, particularly those with fast ascent profiles. In groups of trekkers on Mt Kilimanjaro (5895 m), the incidence of AMS has been reported to be up to 77% on a four-day ascent and 52% on a six-day ascent.5 In contrast, tourist expeditions to similar altitudes with ascent over a couple of weeks, such as in the Himalayas (5400 m), have rates of AMS less than 50%.6 It is important for individuals who intend to participate on such treks to be counselled about the risks and appropriate management of AMS before committing to their plans.
High altitude pulmonary oedema
The pulmonary manifestation of altitude illness is HAPE. Local pulmonary vasoconstriction is thought to be a normal defence mechanism against local areas of hypoxia in the lung; however, in a generalised hypoxic state at altitude, this can cause pulmonary hypertension and in exaggerated cases the vasoconstriction can lead to HAPE.
HAPE is far less common than AMS/HACE, occurring in up to 5% of people at 4300 m but at significantly lower rates below that altitude.7 HAPE that is undetected and untreated can be fatal and is thought to be the leading cause of death at high altitude.
Symptoms of HAPE usually develop two to five days after ascent. It presents as increasing dyspnoea with exertion, which can be hard to differentiate from a normal physiological response to altitude, and progresses to dyspnoea at rest, which is always abnormal and should raise high suspicion of HAPE. A dry cough is common and can progress to frank pulmonary oedema with pink frothy sputum. Other causes of respiratory symptoms such as infection should be considered, but a high degree of suspicion for early HAPE is required in individuals with respiratory symptoms at high altitude.
Immediate descent is the best treatment for HAPE and should be continued until symptoms resolve. If descent has to be delayed due to weather or nightfall then supplemental oxygen (aiming for oxygen saturation >90%) can be used. In severe cases, oxygen during descent/evacuation is indicated. Portable hyperbaric chambers can be beneficial if descent is not possible but, again, descent should never be delayed for the use of these.
Nifedipine has been shown in one study to be useful if descent is not possible and supplemental oxygen is not available.1 Acetazolamide and other diuretics have no role in the treatment of HAPE.
Altitude illness: risk assessment and prevention
As the two key predictors of altitude illness are the speed of ascent and maximum altitude reached, it is essential that the itinerary of a proposed trip be reviewed in order to ascertain an individual’s risk. An approach to risk assessment for AMS based on the Wilderness Medical Society guidelines is presented in the Flowchart.1
The best strategy for the prevention of all forms of altitude illness is gradual ascent and this should be prioritised. Many expedition itineraries now factor this in, but some trips, such as to Mt Kilimanjaro, are particularly prone to fast ascents to limit the number of days on the mountain. It is the increase in the sleeping altitude that is most relevant, hence the adage ‘Climb high, sleep low’. A trip with tight schedules that has little flexibility or limited rest days represents a higher risk for participants.
There is a wide variety in medical support/supervision provided on commercial treks, which may range from an accompanying Australian doctor joining the expedition to local ground operators providing first aid. Participants should always be advised to check the medical support provided from their expedition organiser or company and understand the evacuation protocols in place in the event of a medical emergency, and to ensure they have appropriate travel insurance.
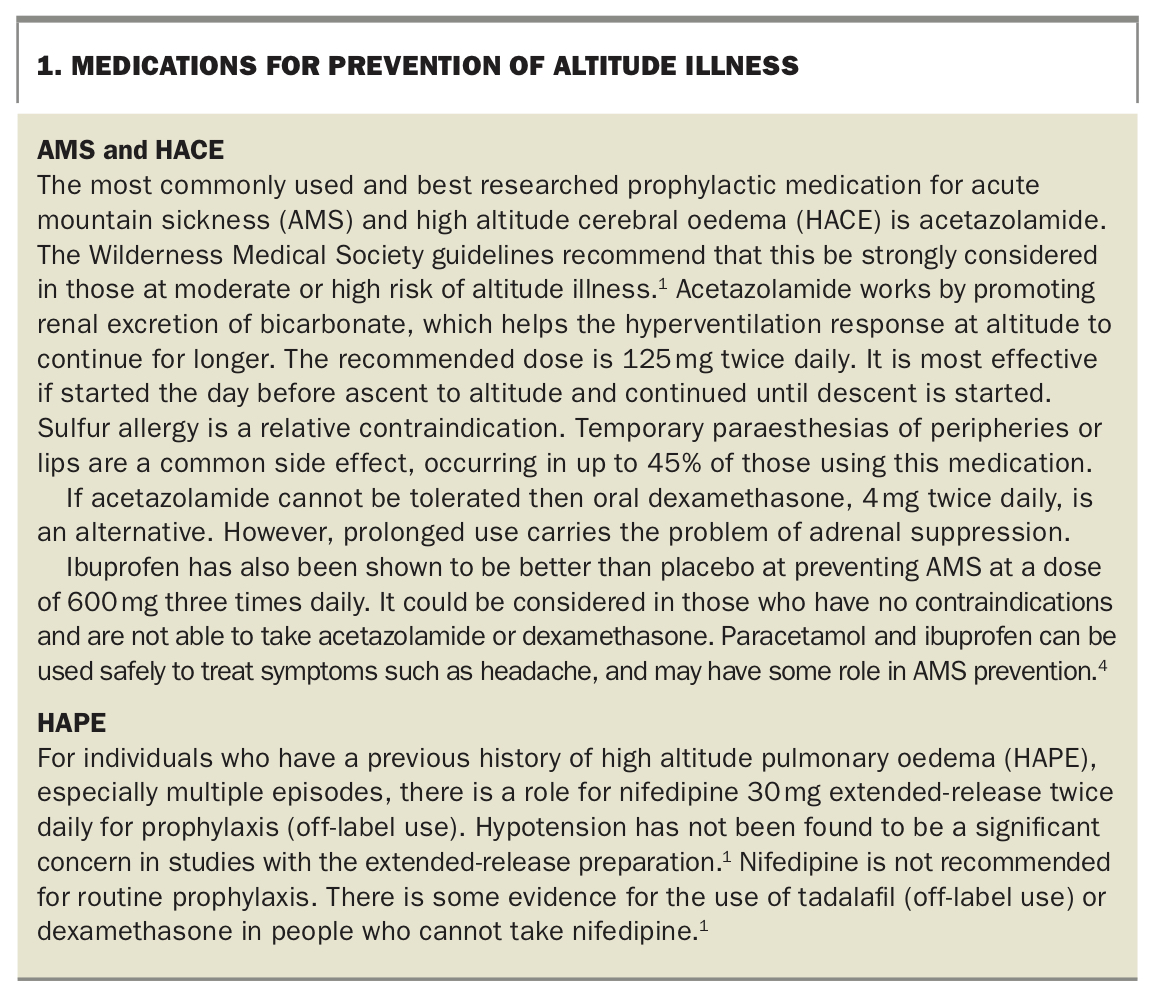
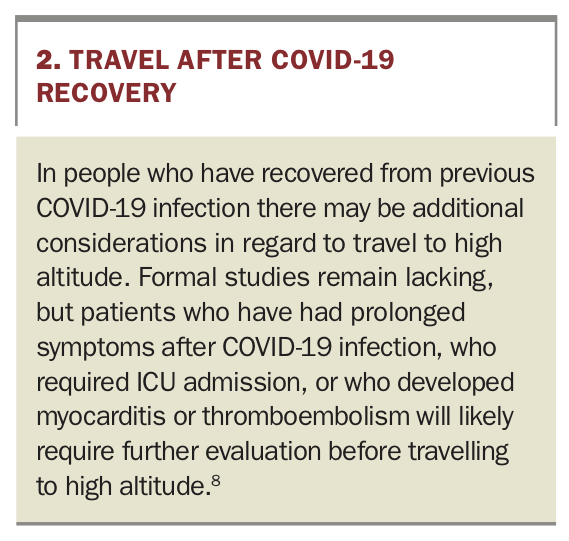
Prophylactic medications to help prevent altitude illness are discussed in Box 1;1,4 travel considerations for those recovered from COVID-19 are given in Box 2.8 It is important to note that intending travellers in low risk situations, as categorised above (see Flowchart), do not necessarily require any prophylactic medication.
{kind=link}
{kind=link}
Conclusion
As international borders reopen, there will be people attempting high altitude travel from Australia, a country that offers no opportunity for pre-acclimatisation. These travellers are at significant risk of developing altitude illness and will often seek guidance from GPs and travel medicine clinics before their departure, so practitioners need an understanding of the spectrum of clinical conditions that can present at altitude, the importance of the travel itinerary (especially the planned rate of ascent) and the options and indications for prophylactic medications. MT
COMPETING INTERESTS: None.