Premature menopause: managing the long-term consequences
Menopause
Women's health
Management of women with premature menopause should focus on maintaining good cardiovascular and bone health and alleviating menopausal symptoms. The psychological consequences of the loss of fertility should also be considered.
Case scenario
Jaya is a 40-year-old woman who is experiencing frequent episodes of sweating and who had her last period one year ago at 39 years of age. She has been investigated by her GP for premature menopause; she has a follicle stimulating hormone (FSH) level of 60 IU/L and currently normal bone density. No secondary medical reason for the cessation of periods was found.
She has no family history of premature menopause and has never had children, by choice. Her cardiovascular risk factors are normal. She is surprised that the GP wants to put her on either menopausal hormone therapy (MHT) or the oral contraceptive pill (OCP). She has no contraindications to either.
What other investigations are required and how should Jaya best be managed?
Commentary
Premature menopause, more accurately described as premature ovarian insufficiency (POI), is a syndrome of at least four to six months of amenorrhoea, hypo-oestrogenism and elevated gonadotrophin levels in a woman younger than 40 years of age, where other causes of secondary amenorrhoea have been excluded.1 POI was first described by Fuller Albright, a Harvard endocrinologist, who used the term ‘primary ovarian insufficiency’ to describe the condition – ‘primary’ referring to the primary defect lying within the ovary.2 It is estimated that about 1% of women will become menopausal before the age of 40 years, whereas the prevalence in women under the age of 30 years is estimated to be 0.1%.3
The diagnosis of POI is based on the measurement of two elevated FSH readings in the accepted menopausal range (>40 IU/L) usually four to six weeks apart. Women with POI have anovulation and hypo-oestrogenism and present with primary or secondary amenorrhoea, infertility, sex steroid deficiency and elevated levels of gonadotrophins. Early loss of ovarian function has significant psychosocial sequelae and major health implications including an almost twofold age-specific increase in mortality rate.4
How common is premature menopause?
POI is said to affect 1% of women before the age of 40 years.3 However, this estimate typically refers only to the prevalence of idiopathic POI. The best estimate of the overall prevalence of POI comes from the long-term follow up of a 1958 UK birth cohort. By the time this cohort reached 40 years of age, 7.8% of women had experienced POI.5
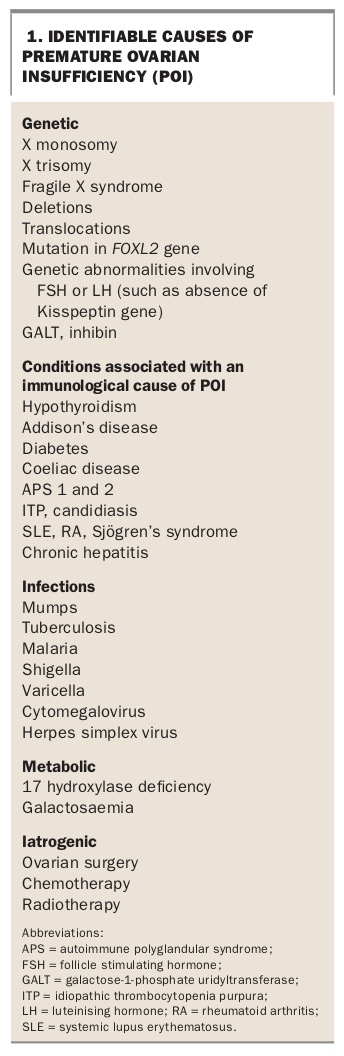
Although the aetiology of POI is often unknown, identifiable causes include chromosomal abnormalities, autoimmune disease, metabolic disorders and surgery on the ovaries (Box 1). Increasingly, the effects of chemotherapy and radiotherapy used to treat malignant conditions are a cause of POI.
{kind=link}
What is the difference between premature and early menopause?
Menopause is said to be premature when it occurs before the age of 40 years. Early menopause occurs between the ages of 40 and 45 years, whereas the average age of the menopause is western communities is 51 years.
What investigations should be performed in patients with suspected POI such as Jaya?
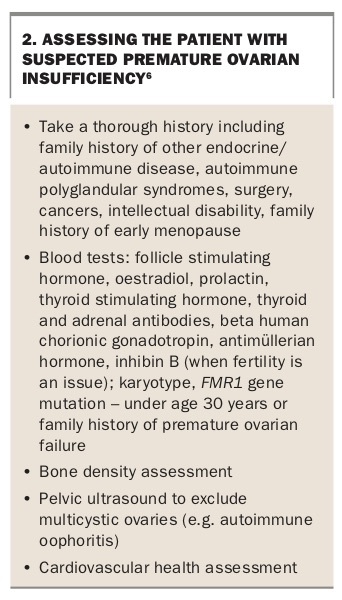
Investigation of a patient with suspected POI should be thorough (Box 2)6, even if the diagnosis seems clear cut as in Jaya’s case. Common causes of secondary amenorrhoea (such as pregnancy, hyperprolactinaemia, polycystic ovarian syndrome, hypothalamic amenorrhoea and POI) should be investigated. In Jaya’s case, her FSH level should be measured again six weeks later to confirm the diagnosis of POI. Measurement of her prolactin and beta human chorionic gonadotrophin (BhCG) levels could also be performed to exclude other causes of secondary amenorrhoea such as pregnancy and hyperprolactinaemia. A thorough personal and family history should be taken.
{kind=link}
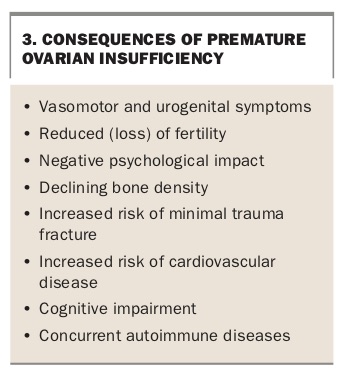
Once the diagnosis of POI is confirmed, other tests should be performed. Autoimmune diseases can coexist with POI and screening requires measurement of thyroid stimulating hormone, vitamin B12 and thyroid, adrenal and coeliac antibody levels. Screening for chromosomal abnormalities such as Turner syndrome and fragile X syndrome (by measurement of the fragile X mental retardation 1 gene [FMR1]) should also be considered. A pelvic ultrasound will exclude possible autoimmune oophoritis and allow for an antral follicle count. For patients concerned about future fertility, an antimüllerian hormone (AMH) measurement may be helpful but this is a poor predictor of menopausal status. A baseline bone density assessment and metabolic health screen should also be arranged. The consequences of a diagnosis of POI are listed in Box 3.
{kind=link}
Many women diagnosed with POI will be overwhelmed by the diagnosis and its consequences and professional counselling and support must be a part of the management plan. Further information and support for patients can be found at the Australasian Menopause Society (www.menopause.org.au), the Daisy Network (www.daisynetwork.org) and Monash University (www.monash.edu/medicine/sphpm/units/womenshealth/toolkit-management-of-the-menopause).
What are the nonhormonal ways of treating hot flushes associated with POI?
Major health concerns for women with POI include an increased risk of premature death, cardiovascular disease, osteoporosis and fracture, cognitive decline and usually significant menopausal symptoms due to oestrogen deficiency. For most women, MHT will be the appropriate treatment for the prevention of these conditions and, unless contraindicated, should be recommended until at least the average age of the menopause.4
When MHT is contraindicated, or refused, management should focus on measures to maintain good cardiovascular and bone health and nonhormonal measures to alleviate menopausal symptoms (Box 4). These include cognitive behavioural therapy, selective serotonin reuptake inihibitors such as escitalopram and paroxetine (off-label uses), serotonin noradrenaline reuptake inihibitors such as venlafaxine and desvenlafaxine (off-label uses), gabapentin (off-label use) and the alpha-adrenergic agonist clonidine. A new class of drugs, neurokinin B receptor blockers, are currently undergoing phase II trials.
{kind=link}
What is the best choice for patients with POI – MHT or the OCP?
MHT is the ideal first choice for most women with POI.7 However, younger women are often more inclined to take the OCP as it is more familiar, less associated with controversy and offers the reassurance of contraception. However, there is a small body of evidence that suggests that OCPs containing ethinyloestradiol may not be as effective in maintaining bone density as MHT.8 The OCP is also contraindicated in women who smoke and those with migraine with aura, and is associated with an increased risk of thromboembolic disease with increasing age.
What is the risk of Jaya’s periods returning spontaneously and what advice would you give her regarding contraception?
A recent mixed retrospective and prospective study that included 358 consecutive women with idiopathic POI found 24% of women showed features of resumption of ovarian activity.9 Most did so within the first year of diagnosis. A total of 21 spontaneous pregnancies were noted in 4.4% of women. Logistic regression analysis showed that secondary amenorrhoea, the presence of follicles on a pelvic ultrasound scan, a family history of POI and higher oestradiol levels were positively predictive for the resumption of ovarian activity.
Women with POI can have intermittent ovarian activity and have a chance of natural conception, although this is likely to decrease with increasing age and duration of amenorrhoea. The likelihood of natural conception in women with POI is estimated to be in the region of 5%. MHT is not contraceptive and women with POI who are keen to avoid pregnancy should be advised to use contraception.
Conclusion
Jaya’s FSH level is measured again six weeks later and the diagnosis of POI is confirmed with no secondary cause identified. She is given advice regarding a healthy lifestyle including attention to diet, weight and regular exercise. She is advised to have a baseline bone mineral density assessment, blood tests to check her fasting lipid and blood sugar levels and to have these tests repeated at regular intervals. She is offered counselling to discuss the ramifications of this diagnosis.
Jaya is prescribed MHT for alleviation of her symptoms and to aid her metabolic and bone health. She is also warned that this is not contraceptive and that, although the chance of spontaneous pregnancy is low, she should continue to use contraception, if she does not wish to conceive, until the normal age of the menopause. MT