Managing bipolar disorder – key clinical recommendations

Mental health
Bipolar disorder typically arises with depressive symptoms during late adolescence, with mania following some years later. The GP has a key role in identifying patients presenting with mania and ensuring appropriate acute and long-term management. Key recommendations on each stage of the disorder can aid in developing a comprehensive biopsychosocial and lifestyle approach to management.
- Management of bipolar disorder requires a biopsychosocial and lifestyle approach.
- The aim of management is to maintain mood stability.
- The medications required differ according to the stage of the illness.
- In the long term, maintenance of an effective mood-stabilising agent is essential.
- Management of bipolar depression differs from the management of major depressive disorder.
- Antidepressant monotherapy for bipolar depression is not indicated.
Bipolar disorder (BD) is a chronic lifelong illness characterised by acute exacerbations of mania or hypomania and episodes of depression, along with periods of euthymia (normal mood), that affects both sexes equally.1 Onset typically occurs during late adolescence with either depressive symptoms or an episode of major depression, and mania usually follows some years later (Box 1). In clinical practice, this is a problem because there are no clinical features that reliably distinguish a first episode of major depressive disorder (MDD) from one of bipolar depression, and the diagnosis of BD is often delayed for many years. The detection and diagnosis of BD are therefore inherently complicated.
{kind=link}
For classification and research purposes, BD is sometimes divided into bipolar I and bipolar II subtypes. However, in practice, this distinction, which is based on the severity and duration of manic symptoms, is arbitrary and does not meaningfully inform management.2 Hence, this article simply refers to BD.
The treatment of BD is complex because each phase of illness requires a different approach. Management calls for attention to the lifestyle factors that help to maintain wellness, in addition to biological and psychological treatments, so a comprehensive biopsychosocial and lifestyle (BPS-L) approach is needed. The Royal Australian and New Zealand College of Psychiatrists (RANZCP) Clinical practice guidelines for mood disorders provide detailed evidence- and consensus-based recommendations for the assessment and management of BD over each phase of the disorder.3 A summary version of these guidelines for BD is also available.4
This article provides an overview of the guidelines’ key recommendations for managing each phase of the disorder: mania (acute and continuation treatment), bipolar depression and long-term maintenance.
Clinical recommendations for the management of mania
Acute mania
Treatment of acute mania should generally occur under the supervision of a psychiatrist in an inpatient unit, with the patient being cared for under the relevant Mental Health Act if necessary. The GP has a key role in identifying patients presenting with mania – for example, identifying the early warning symptoms of mania when a patient’s family or carers present with concerns about problem behaviour – and ensuring appropriate management. This will involve organising a referral to the local mental health service or emergency department (often using the provisions of the Mental Health Act).
Inpatient treatment is usually necessary because the reckless spending, inappropriate sexual behaviour and other high-risk goal-oriented actions associated with mania can damage the individual’s relationships and reputation. Patients with mania can be very persuasive and may convince their family and GP that they are well and nothing is wrong. It is not uncommon for patients presenting with mania to push limits and rationalise their inappropriate behaviour to make a case for not being admitted. It is wise to be prudent in such cases, to insist on the patient being admitted to hospital and to not succumb to the patient’s persuasive arguments that all is well, while still maintaining rapport with both the patient and family members.
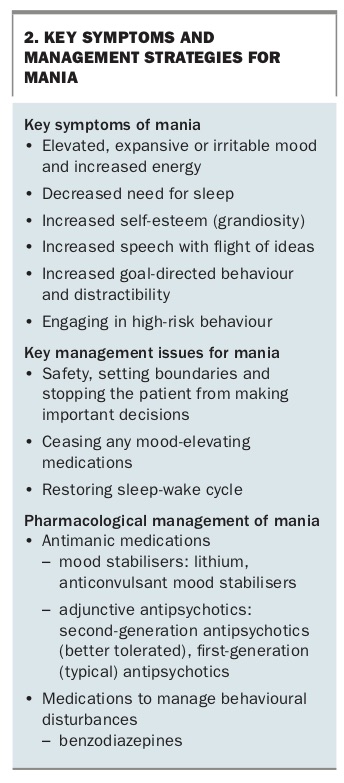
The management of acute mania involves treating the biological symptoms using an antimanic agent, such as lithium (a mood stabiliser), or an anticonvulsant mood stabiliser in combination with an antipsychotic, preferably one of the better tolerated second-generation antipsychotics (SGAs). Benzodiazepines can be added, especially at the outset, for a limited time, to counter overarousal and disturbed behaviour, and a hypnotic can be useful to reinstate a regular pattern of sleep.
Behaviourally, firm limit setting is essential, and a low-stimulus environment is necessary to lower activity levels. While in a manic state, patients should be prevented from making important and lasting decisions, such as changing jobs, investing money or starting or ending relationships.
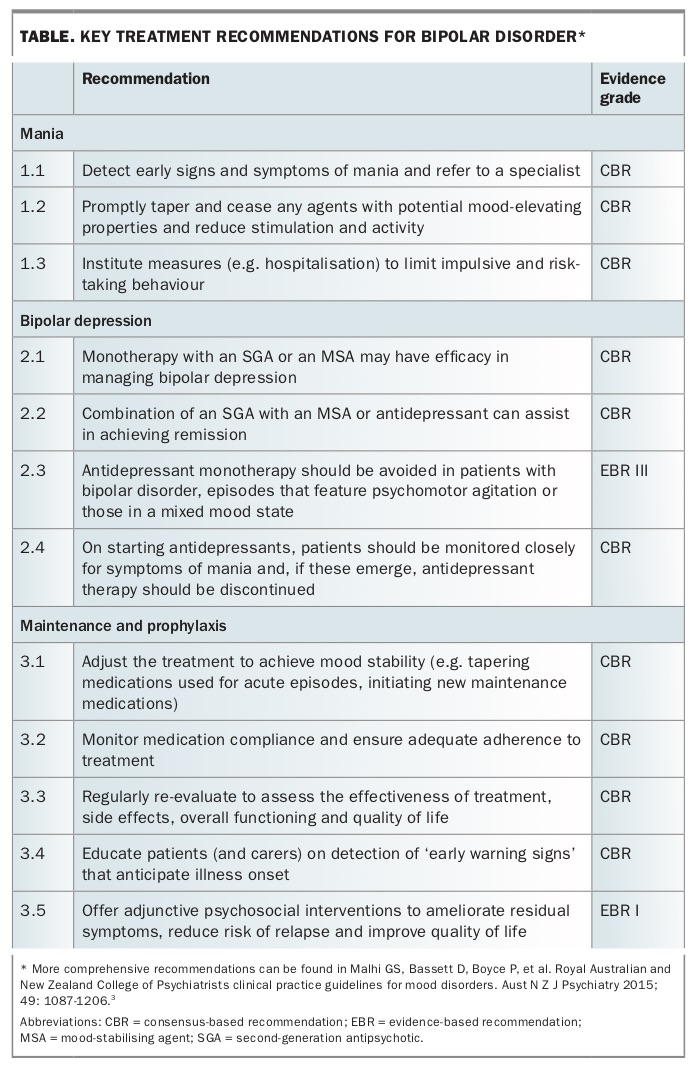
The main features of mania and its treatment are summarised in Box 2. The Table provides the key recommendations for the management of mania.
{kind=link}
{kind=link}
Continuation treatment
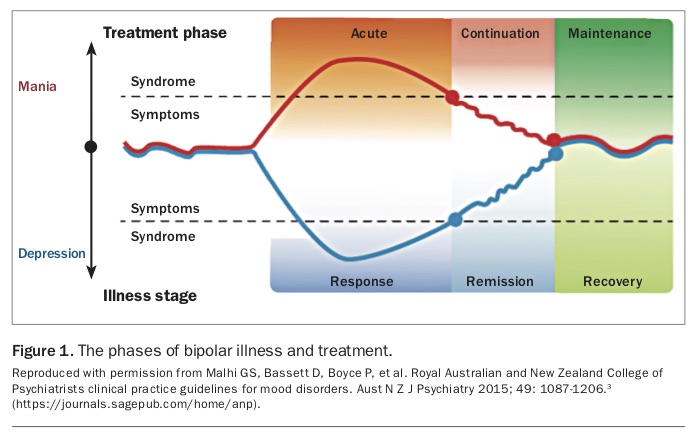
Once the acute symptoms of mania resolve, the focus of management shifts to the continuation phase (Figure 1).3 This phase of treatment usually commences in the inpatient unit and continues for some months after discharge from hospital until the patient has achieved a significant period of mood stability. The goals in this phase are to achieve optimal mood stability, prevent the recurrence of acute episodes and work towards full functional recovery.
{kind=link}
Although this phase of management will often take place under the supervision of a psychiatrist or a community mental health team, the GP once again has a central role, especially for patients in rural and remote areas where access to specialist care is limited. The GP is ideally placed to work with the patient (and family) to ensure that the patient achieves, and maintains, a healthy lifestyle, a stable sleep-wake cycle and a healthy diet and does not engage in risky behaviour or activities that are likely to lead to relapse, especially substance and alcohol misuse; key aspects of a BPS-L approach. As shift work can destabilise circadian rhythms, it should ideally be limited, if possible, until a sustained period of mood stability has been achieved and strategies have been put in place to deal with the changing sleep-wake cycle. Attention to diet is especially important if the patient is taking an SGA that can cause increased appetite and weight gain and put the patient at risk of a metabolic syndrome.
Psychoeducation for the patient and his or her carers, including identification of early warning signs (or symptoms) of relapse, is an important intervention at this stage of management.5 Enquiring about any early warning signs at regular consultations with the patient is essential so that emergent symptoms can be promptly treated, to avoid relapse.
Pharmacological aspects of management at this stage include the withdrawal of any medications, such as benzodiazepines, that had been used to manage acute behavioural and cognitive disturbance. Medications need to be rationalised, and the dose of adjunctive medications, especially SGAs, should be gradually tapered down, with the aim of maintenance monotherapy with a mood stabiliser. Although this is the ideal management strategy, many patients with BD will require more than one mood-stabilising agent (e.g. lithium and sodium valproate6) or a mood stabiliser in combination with an SGA (olanzapine, quetiapine or aripiprazole) or the anticonvulsant lamotrigine3 – making use of the relapse-prevention properties of SGAs and lamotrigine.
Once a patient has achieved a period of at least six months of mood stability with continuation treatment, management transitions to long-term maintenance therapy.
Clinical recommendations for the management of bipolar depression
Bipolar depression (an episode of major depression in a patient with BD) is generally more difficult and complicated to treat than MDD, and the outcomes are often not as good. This is partly because no medications have been specifically developed to treat this phase of BD, and conventional antidepressant medications are not as efficacious for bipolar depression as they are for MDD.7,8 Antidepressants also have the potential to trigger manic symptoms and can lead to ‘cycle acceleration’ (increased frequency of episodes) and possibly precipitate mixed episodes (a coexisting combination of manic and depressive symptoms). If antidepressants are to be used, as they often are in clinical practice, they should only be prescribed in conjunction with a medication that has antimanic properties (e.g. lithium, SGAs), and the patient should be carefully monitored in case of an emergent manic switch.
Bipolar depression is best managed using a different approach than that used to treat MDD.9 Patients should be offered adjunctive evidence-based psychological therapies, such as cognitive behavioural therapy, as part of a BPS-L approach to managing this highly impairing phase of BD, especially when psychosocial factors are the trigger for the episode of bipolar depression.
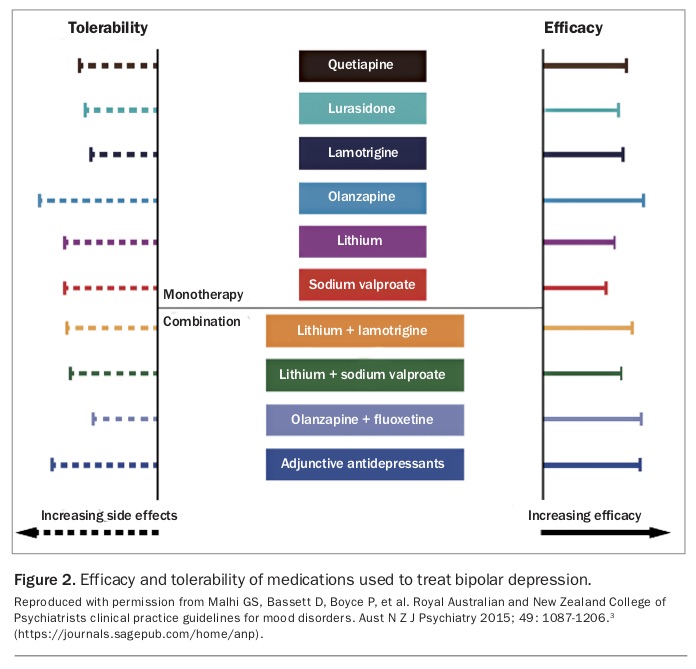
Pharmacological treatment can be separated into monotherapy or, more commonly, combination approaches. Monotherapy can seem somewhat counterintuitive, as the recommended medications are the same as those used to treat mania. However, in practice, a trial of monotherapy is often necessary to first identify those patients who can be managed with a single agent. The SGAs (in rank order of efficacy and tolerability) quetiapine, lurasidone (approved and PBS subsidised only for the treatment of schizophrenia) and olanzapine have the strongest evidence base (Figure 2). Lithium, lamotrigine and sodium valproate can also be administered as monotherapy, as they have proven efficacy in treating bipolar depression. Lamotrigine is considered the preferred mood stabiliser for individuals with a predominant depressive pole of illness.
{kind=link}
Although monotherapy is preferable, patients often require combinations of medications. These include lithium, sodium valproate or lamotrigine in combination with an antidepressant, or an SGA in combination with an antidepressant. Referral to a psychiatrist is recommended if patients do not respond to these approaches, as treatments such as electroconvulsive therapy would be the next step in management.
The key recommendations for the management of bipolar depression are provided in the Table. Treatment at this stage should involve a specialist, alongside management in primary care.
Clinical recommendations for the long-term management of bipolar disorder
The aims of maintenance treatment are to prevent relapse or recurrence of manic and depressive symptoms, optimise full functional recovery, build resilience and provide long-term prophylaxis using a BPS-L approach. Developing a strong and trusting doctor-patient relationship is fundamental to this, so that the patient has confidence in reporting any potential signs of relapse. Encouraging patients with BD to maintain a healthy lifestyle is an important intervention, as substance misuse and a chaotic lifestyle (with an unstable sleep-wake cycle) can be major factors in triggering a relapse.
Psychotherapeutic approaches are essential and should be integrated into management. All patients and their carers should be offered psychoeducation about BD and its treatments. Good-quality information should be made available to them; a guide extracted from the RANZCP Clinical practice guidelines for mood disorders can be downloaded from the Your Health in Mind website (www.yourhealthinmind.org/mental-illnesses-disorders/bipolar-disorder) for this purpose. Patients and their families need to be taught how to closely monitor the patient’s mood, recognise early warning signs and know what strategies to use if early warning signs emerge; especially how to promptly seek assistance. Families and carers are important allies in long-term management, as they may be the first to recognise early warning signs.
Long-term pharmacological management principally involves maintaining treatment with an effective prophylactic mood stabiliser. This entails regular reviews of the patient to check for the presence of any depressive or manic symptoms, ask about and manage any side effects and ensure medication adherence. Patients with BD need to be advised that they will have to continue taking mood-stabilising and prophylactic medication indefinitely to prevent future episodes of illness; this is an essential component of psychoeducation.
In the initial stage of long-term treatment, the medications used during the continuation phase should be reviewed and those that are no longer necessary discontinued. The choice of long-term maintenance medication depends, in part, on the predominant polarity of illness. Lithium is the preferred mood stabiliser, especially for those with manic episodes, whereas lamotrigine can be considered for those with a predominantly depressive polarity. Although lamotrigine is not PBS listed for the treatment of BD, the cost of a private prescription is affordable. The choice of medication requires balancing the benefits and side effects of each.
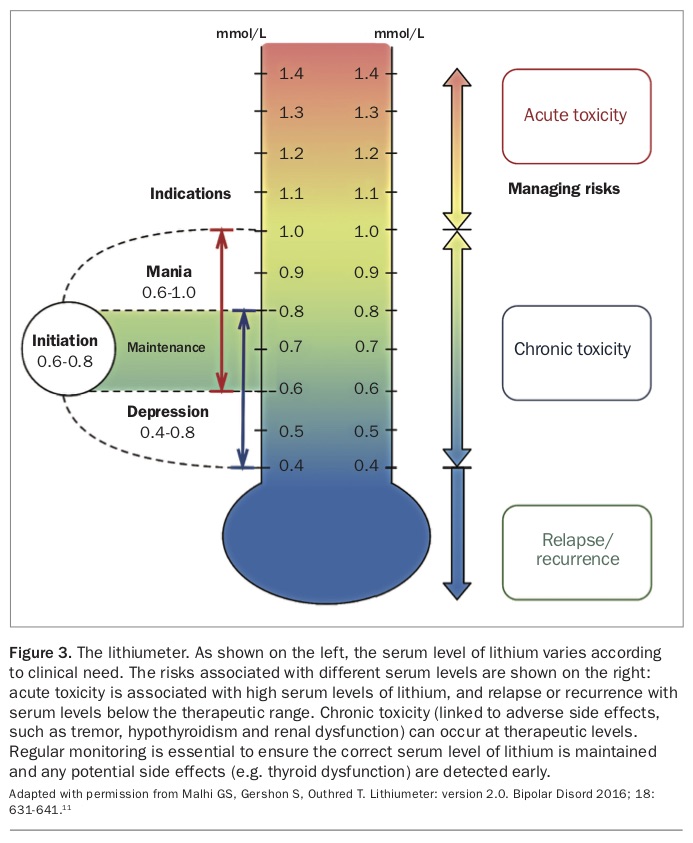
Lithium remains the gold standard in achieving mood stability and long-term prophylaxis. As a first-line treatment, lithium provides excellent efficacy in terms of relapse prevention and protection against suicide. Should relapses occur, it may also reduce the severity and frequency of these episodes. Managing lithium treatment requires patient engagement, as there is a need for regular monitoring of serum lithium levels (to maintain a therapeutic level of between 0.6 and 0.8 mmol/L) and adjustment of oral dosing to ensure tolerability and limit the risk of toxicity. As lithium can induce hypothyroidism or hyperparathyroidism and can affect renal function, the patient’s thyroid function, serum calcium level, electrolytes, urea and estimated glomerular filtration rate should also be routinely monitored.10 Details on adjusting the dose of lithium and the frequency of monitoring can be found using the ‘lithiumeter’ (Figure 3).11 In essence, monitoring should initially take place weekly, then monthly and, when a stable serum lithium level has been achieved, every three months.
{kind=link}
Other maintenance treatments can be added to lithium if necessary; some patients require the addition of an anticonvulsant or an SGA to achieve mood stability. If the patient is taking an SGA, regular monitoring for potential metabolic side effects is essential. The maintenance dose of the SGA will be lower than the dose used in the acute phase, and careful tapering of the SGA dose is required to maintain efficacy and minimise side effects, especially weight gain.
To ensure successful long-term management, it is imperative that physicians work with the patient to develop a strategy for medication adherence, while minimising any adverse effects. A collaborative discussion with patients and their carers regarding the benefits and negative consequences is necessary at the outset of treatment and whenever a significant change to management is being considered.
Typically, the emergence of symptoms is gradual, and they increase in number and severity over a period of days. It is therefore important that both patients and physicians are able to detect early warning signs and anticipate the onset of episodes of illness and adjust treatment accordingly. Reviewing patients more frequently at times of predictable stress, or at the times of year when relapses have occurred in the past, may allow for the identification of imminent relapse.
The key recommendations for the maintenance management of BD are provided in the Table.
Conclusion
The RANZCP Clinical practice guidelines for mood disorders provide updated and relevant information for clinicians regarding the BPS-L management of BD.3 The full guidelines contain clinical algorithms concerning the acute, continuation and maintenance phases of treatment and provide clear guidance to ensure the optimal management of lithium therapy. The advice provided in the clinical practice guidelines should equip clinicians to navigate the complexities of managing all phases of BD. MT