Combined oral contraceptives: the GP consultation

Women's health
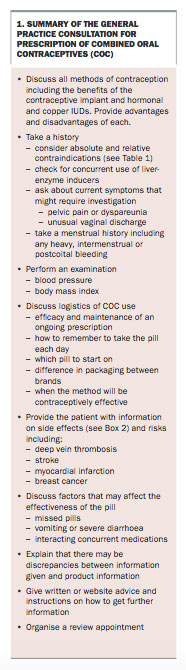
The consultation with a woman requesting contraception is most often straightforward. However, some important details must be considered to decide on the most appropriate type.
The uptake of the combined oral contraceptive (COC) is about 33% among Australian women using contraception.1 This article focuses on the GP consultation for women who have chosen to initiate or continue a particular type of contraceptive. Although this consultation is often straightforward, several issues need to be considered (Box 1).
{kind=link}
Which contraceptive method is suitable?
For women initiating contraception, all methods should be discussed including long-acting reversible contraceptives (LARCs) such as the contraceptive implant, the hormonal intrauterine system and copper intrauterine devices (IUDs).
LARCs are affordable and effective contraceptive methods that have few contraindications and high satisfaction and continuation rates.2-4 They are particularly suitable for women who find daily pill taking and/or maintaining a filled prescription difficult, or if concealment from other household members is important. If the patient wishes to continue discussing the prescription of a COC the consultation should include the following information.
Advantages of COCs
COCs are readily accessible, easily reversible, provide predictable withdrawal bleeds and allow women to manipulate their cycles to skip withdrawal bleeds. They decrease the occurrence of acne and can be used in the management of women with heavy menstrual bleeding, dysmenorrhoea, symptoms of endometriosis, polycystic ovarian syndrome or premenstrual dysphoric disorder.5-16 Women taking COCs have a reduction in their risk of endometrial, ovarian and bowel cancers, as well as functional ovarian cysts and benign ovarian tumours.17-21
Disadvantages and risks of COCs
COCs have relatively high failure rates with typical use.22 There is a regular cost associated with their purchase, which is significantly higher for non-PBS formulations. The use of COCs is associated with rare but serious risks, including the risk of venous thromboembolism (VTE) and a possible increased risk of stroke and myocardial infarction.23-25 There is a small increase in the risk of cervical cancer and possibly breast cancer.26,27 COCs do not provide any protection from sexually transmitted infections so condoms are recommended for this purpose.
Contraindications to use of COCs
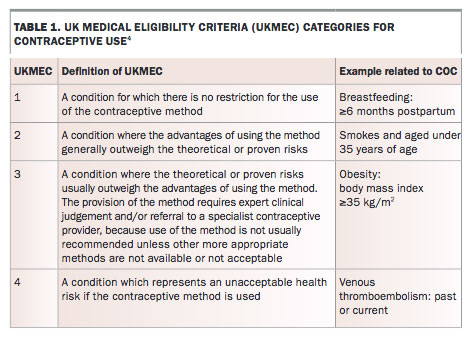
The UK Faculty of Sexual and Reproductive Health (FSRH) medical eligibility criteria (MEC) system for contraceptive use provides a framework for matching a woman’s medical and personal history with her chosen contraceptive (Table 1).4
{kind=link}
Personal history
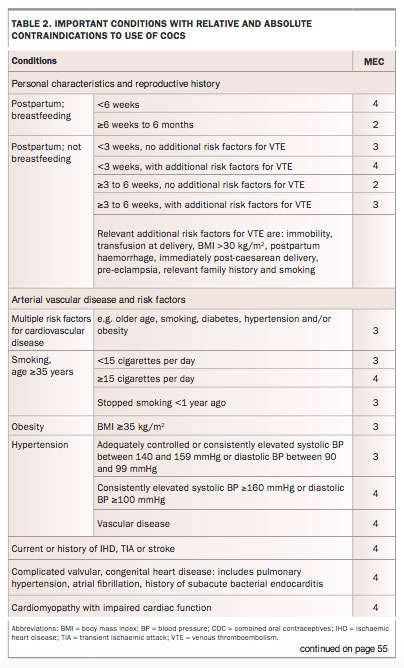
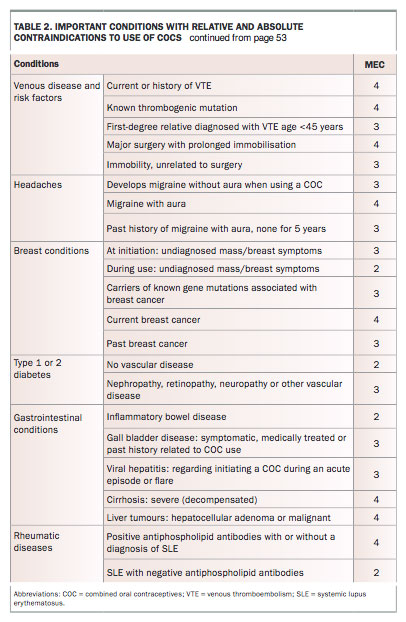
Risk factors for, or a past history of, VTE, arterial vascular disease, hormonally-related cancers and severe liver disease are important contraindications to consider when prescribing a COC (Table 2 and Table 2 cont.).
{kind=link}
{kind=link}
Common MEC 4 (absolute contraindications) include:
- migraine with aura in the previous five years
- smoking 15 or more cigarettes per day and over the age of 35 years
- less than six weeks postpartum in breastfeeding women.
Common MEC 3 (relatively strong contraindications) include:
- a body mass index of 35 kg/m2 or more
- controlled hypertension
- smoking up to 15 cigarettes per day and over the age of 35 years.
Family history
A history of VTE of any cause in a first-degree relative at the age of 45 years or younger is an MEC 3 for the use of COCs. Other aspects of family history such as early-onset arterial disease may prompt further risk assessment.
Medications
An IUD or depot medroxyprogesterone acetate is recommended in women taking long-term liver-enzyme inducers. These medications render COCs potentially less effective and include several anticonvulsants and antiretrovirals, as well as St John’s Wort. For women who prefer to take a COC, a higher hormonal dose is recommended but it is important to note that the 50 µg ethinyl oestradiol pills available in Australia contain insufficient progestogen for this purpose. See the FSRH advice for more detailed advice on this higher dosing regimen.28 Antibiotics, apart from rifabutin and rifampicin, do not reduce the effectiveness of COCs.
General history
Ask the patient if she has experienced any abnormal bleeding, discharge or pelvic pain. Although a COC can be initiated, further investigation might be warranted.
Examination and investigations
The only routine recommended examination for a women requesting a prescription for a COC is measurement of blood pressure and calculation of body mass index (BMI). No routine investigations are required, although the consultation can present an opportunity to discuss chlamydia testing, cervical cancer screening, and lipids and glucose testing.
Prescribing for specific populations
Young women
Young women assessed by you to be mature minors can consent to a prescription of a COC. Assess whether there is a risk of harm or abuse from sexual activity and follow relevant mandatory reporting legislation. Confidentiality and its limitations should be discussed and the young person can be seen alone for some of the consultation.
From a medical perspective, there is no lower age limit for prescribing COCs if a young woman has started menstruating.29
Postpartum
Breastfeeding
In breastfeeding women, the use of COCs is contraindicated (MEC 4) until they are at least six weeks postpartum. A recent change to guidelines, supports the use of COCs between six weeks and six months postpartum (MEC 2), although other options including progestogen-only methods may be preferable.4 Once a woman reaches six months postpartum, the use of COCs is unrestricted (MEC 1).
Non-breastfeeding
Restrictions for using COC in non-breastfeeding women are related to VTE risk, which is highest in the three weeks postpartum (Table 2 and Table 2 cont.). There are no restrictions (MEC 1) after six weeks postpartum.
After an abortion
Women should be advised to start with an active pill the day after a first or second trimester surgical or medication abortion (day after misoprostol tablets). The COC will be immediately effective.
Older women
The COC can be appropriate for medically eligible women over the age of 40 years but VTE and arterial vascular risk factors need careful consideration. Additionally, the COC can control appropriately investigated heavy menstrual bleeding and perimenopausal symptoms. Progestogen-only methods or IUDs are safer options for women over 50 years of age.30
Important points to cover
Efficacy and maintaining a supply
Although the COC is considered 99.7% effective with perfect use,31 the typical use probability of failure in the first 12 months is 7 to 10%.22 Efficacy should be explained to patients in a meaningful way, such as if 100 women take the pill for one year, about seven of them will become pregnant. It can be useful to discuss ways of remembering to take the pill, including phone reminders or apps and keeping the pill handy. Inform women how they can obtain an emergency supply from a pharmacy if they run out.32
Side effects and risks
When prescribing a woman a COC, inform them of the risks as outlined above.
Evidence about side effects with COC use is limited (see Box 2 for a list of reported side effects). Unscheduled bleeding is common initially and usually settles with time. Withdrawal bleeding may not occur, particularly with pills containing oestradiol or oestradiol valerate.33,34 Many side effects, including mood changes, lowered libido and weight changes, may be attributed to the pill but evidence is limited. It is recommended to persist with a COC for at least three months to allow side effects to settle.
{kind=link}
Prescribing and when to start
Traditionally, COCs are started on days one to five of menstruation to ensure the woman is not pregnant. It will be immediately effective if starting with an active hormone pill. However, COCs can be started at any other stage in the cycle (‘quick start’ initiation) but will not become effective until seven days of active hormone pills have been taken. If an early pre-existing pregnancy is not excluded when quick starting the pill, advise the woman to have a urine pregnancy test four weeks after initiation, noting that a false-negative test may occur if unprotected intercourse has occurred within the previous three weeks.
Packaging varies between formulations, and in a consultation swatches available from pharmaceutical companies can be used to demonstrate the difference between active and inactive pills, which pill to start with and when the woman will be covered for contraception. Pills packaged to start with an active pill are generally easier to manage.
Usually, the patient should be given an initial prescription for four months of COC. However, a prescription for up to a 12 months’ supply can be considered for women with a low risk of arterial disease who may find it difficult to attend for earlier initial review. At review after the first four months, 12 months can be prescribed if the woman is normotensive and problem free.
Factors affecting efficacy
Missed pills
Missed pill rules are governed by the principal that ovulation may occur if there are more than seven consecutive days without hormone pills and that a pill is not considered missed until it is more than 48 hours since the last pill was taken (Flowchart).35
Vomiting and severe diarrhoea
Vomiting within two hours of taking a pill or very severe diarrhoea should be managed as for missed pills.
Providing information
Written information or links to relevant websites, especially in relation to missed pill rules, should be provided with a prescription for a COC. State or territory-based family planning services can usually offer women advice over the phone and product information might differ from some of your advice.
Skipping withdrawal bleeds
Extended or continuous use of active pills with skipped inactive pills is mostly chosen for convenience.36 These regimens can minimise withdrawal bleeding and provide relief from hormonal withdrawal symptoms including premenstrual syndrome, headaches and pelvic pain.37,38 Women with endometriosis will also benefit from an extended regimen.39 Women may choose to tri-cycle three pill packs in a row or continuously take the pill for up to 12 months or more at a time. A prepackaged extended cycle pill is available with 84 consecutive combined hormonal pills followed by seven 10 µg ethinyl oestradiol pills and another pill is available with an electronic dispensing device. These preparations allow for flexible timing of withdrawal bleeds and are available in Australia as alternative choices for women wishing to skip withdrawal bleeds.
Review and repeat pill consultations
At each repeat consultation for COC prescription, the patient should have her blood pressure measured, BMI calculated, if indicated, and any problems including side effects investigated. Specifically enquire about abnormal bleeding. Smoking, personal and family history can be updated and new medications added to the records. Discuss if she has missed any pills and review the patient’s understanding of the missed pill rules and what to do in the case of vomiting or severe diarrhoea. The benefits of switching to a LARC can be discussed if appropriate.
Conclusion
Information on personal risk factors, family history and concurrent medications is important for safe prescribing of COCs. The patient’s understanding of the consequences of missed pills should be checked at each visit. The consultation can be an opportunity to promote safe sex and chlamydia and cervical cancer screening, and to provide information about other contraceptive choices including LARCs. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.