Managing type 1 diabetes: new technology and its application

Diabetes type 1
Diabetes medicines
Insulin pumps, continuous glucose monitoring, smart glucose meters and phone apps are rapidly changing the way people with diabetes manage their blood glucose levels. General practitioners need to keep up with these innovations to feel comfortable managing people with type 1 diabetes both now and into the future.
- An understanding of how new devices for managing type 1 diabetes work and familiarity with the terminology used will help GPs support patients presenting with the common problems of hyperglycaemia and hypoglycaemia.
- Insulin pumps use only rapid-acting insulin and achieve the effect of long-acting insulin through constant delivery of rapid-acting insulin at varying rates across a 24-hour period.
- The common complication of insulin pump therapy of an occluded insulin delivery infusion set can be quickly corrected out of hospital if recognised and appropriately managed before diabetic ketoacidosis develops.
- Continuous glucose monitoring is now available for people using multiple daily injection insulin regimens as well as those using insulin pump therapy. It will be used increasingly by young people with type 1 diabetes because of new funding for those aged under 21 years.
- Smart glucose meters and phone apps can be used to calculate bolus insulin doses in people on multiple daily injection insulin regimens similarly to as in those using insulin pumps.
Picture credit: © BSIP/Belmonte/Diomedia.com Model used for illustrative purposes only
There have been considerable changes to the way insulin dosing is managed in people with type 1 diabetes in the past few years, including the uptake of insulin pump therapy and other impacts of this therapy, such as the use of smart meters and phone apps in calculating bolus insulin doses for people on multiple daily injection insulin regimens.
People with type 1 diabetes (and some with type 2 diabetes and cystic fibrosis-related diabetes) are increasingly using insulin pumps and continuous glucose monitoring. In 2012, more than 12% of the type 1 diabetes population in Australia, and up to 60% of young people (under 18 years) with type 1 diabetes, were using insulin pump therapy.1 From June 2017, continuous glucose monitoring sensors will be subsidised through the National Diabetes Supply Scheme for people with diabetes aged under 21 years, which will significantly increase their use. ‘Closed loop’ insulin pumps will become available in the next two to three years, fully linking insulin pump therapy and continuous glucose monitoring and beginning a new era in therapy for type 1 diabetes. Although management of insulin pump therapy requires a team approach by an endocrinologist, diabetes educator and dietitian, an understanding of how the devices work and familiarity with the terminology used will help GPs support patients presenting with the common problems of hyperglycaemia and hypoglycaemia.2
Insulin pumps
How do insulin pumps work?
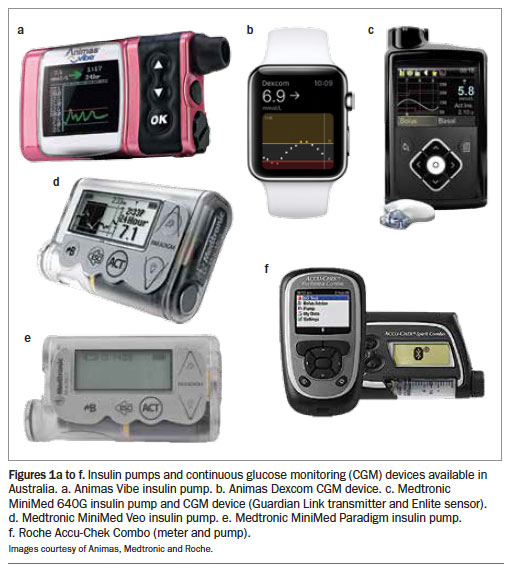
There are three main insulin pumps available in Australia at present, marketed by Medtronic, Animas and Roche (Figures 1a, c to f and Figure 2). All operate along the same principles. Insulin pumps use only rapid-acting insulin (aspart, lispro or glulisine; 100 IU strength).
{kind=link}
{kind=link}
Basal insulin delivery
The long-acting component of multiple daily insulin injection regimens is replaced by constant delivery of 0.025-unit aliquots of rapid-acting insulin into the subcutaneous tissue, divided equally over the hour depending on the programmed delivery rate. This way of delivering rapid-acting insulin is termed basal insulin delivery, and creates a reservoir of insulin in the subcutaneous tissue. The delivery rate is programmed into the pump and can be adjusted across the 24-hour period according to individual requirements. The insulin is delivered through an infusion set (a cannula inserted into the subcutaneous tissue), which is ideally changed by the person every three days to minimise the risk of line occlusion and maintain consistent delivery.
Basal rate changes take up to two hours to take effect and therefore intervals between basal rate changes should be a minimum of three hours to allow equilibration at the different basal rate.
Bolus insulin delivery
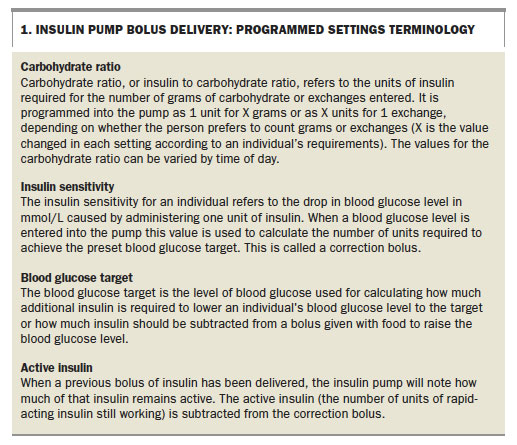
Delivery of additional insulin by the pump, a bolus dose to correct an elevated blood glucose level or to match food intake, is initiated by the patient. The bolus amount is calculated by the pump (‘bolus calculator’) based on pre-programmed settings that include a carbohydrate ratio (also known as the insulin to carbohydrate ratio), a sensitivity setting, a duration of action to determine the amount of ‘active insulin’ remaining after a previous bolus, and a blood glucose target to correct the blood glucose level (Box 1).
{kind=link}
Duration of insulin action is usually set at two to four hours, and preset targets for blood glucose are usually set between 5 and 6.5 mmol/L, depending on individual goals.
The person using the pump can ‘override’ or change the advised bolus dose and can also deliver a ‘manual bolus’ of their own choosing. A manual bolus or alteration of a recommended dose may be necessary to prevent hypoglycaemia associated with physical activity or for correction of ketosis in sick day management. For the latter, additional insulin may be required to manage ketosis because the pump may not allow administration of additional bolus insulin when giving repeated correction bolus doses to clear ketones (see also section on ‘Sick day management’).
Circumstances requiring temporary changes in basal delivery
Insulin pumps have the advantage that the basal delivery can be changed at short notice. Unlike with the long-acting insulins detemir and glargine that are given every 12 to 24 hours, altered basal insulin delivery by a pump will impact blood glucose levels two hours later.
Basal delivery is altered using temporary basal rates. In general, it is easiest to change basal delivery as a percentage increase or a percentage reduction to remain in keeping with an individual’s existing basal requirements. Considering reduced and increased basal deliveries:
- reduced basal delivery can be used to prevent exercise-induced hypoglycaemia or to allow for prolonged physical activity over a day, such as at work; usually reductions of 20 to 50% are required
- increased basal delivery is useful for managing increases in blood glucose level that can result from a significant reduction in usual activity and, importantly, in sick day management or following a period of line occlusion resulting in hyperglycaemia.
Temporary basal rates can be set for one to 24 hours; the rate will return to the normal basal delivery at the end of the time period set.
Management of line occlusion causing hyperglycaemia
There was an initial concern when insulin pumps were introduced that there would be an increase in episodes of diabetic ketoacidosis caused by line occlusion (the complete absence of insulin in the subcutaneous space within three to four hours of the blockage leading to a rapid rise in blood glucose level with prompt development of ketosis). This has not been borne out in practice, with most studies showing a reduction in ketoacidosis with pump use. Unpublished data from the young adult diabetes service at Westmead Hospital, Sydney, have shown that reduced diabetic ketoacidosis presentations in insulin pump users depend on the provision of after-hours phone support to assist with trouble shooting in the event of pump failure or infusion set occlusion.
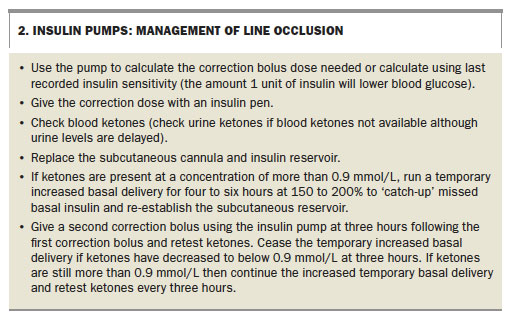
People who use pumps are educated in the management of line occlusion and to suspect line occlusion if a high blood glucose level does not correct after a standard correction bolus. Unfortunately, the insulin pump will not alarm unless a line is completely occluded, and partial occlusion causes incomplete insulin delivery. If the line has occluded, recommended management is to use an insulin pen injection of rapid-acting insulin to re-administer the correction bolus (Box 2). Unlike ketosis due to illness, ketosis due to a line occlusion rapidly corrects on resuming insulin.
{kind=link}
Sick day management
Insulin pumps have the significant benefit in sick day management of enabling temporary increased basal delivery to manage diabetic ketosis. Provided the person is not repeatedly vomiting and can maintain hydration status, they can effectively run their own insulin infusion to correct ketosis.
If the ketone level is between 1.5 mmol/L and 3.0 mmol/L and the blood glucose level is more than 15 mmol/L then the pump basal delivery should be increased to 150 to 200%, depending on the level of blood glucose, until ketosis is resolved. Blood glucose and ketone levels should be tested every three hours and additional correction boluses administered as necessary.
If the blood ketone level is more than 3.0 mmol/L then advice should be obtained from the person’s usual endocrinologist or they should be referred to the local emergency department. If there is ketosis with a low or normal blood glucose level then the person should be advised to use an oral rehydration drink, sport drink or any other sugared drink that is tolerated and to sip it regularly to keep blood glucose levels above 5 mmol/L while the increased basal rate is continued until the ketosis is resolved. The increased basal rate is required for as long as ketosis persists, to prevent progression to diabetic ketoacidosis. Normal basal rates can be resumed when the ketone level falls to below 0.9 mmol/L and then blood sugars should be managed with the correction bolus.
If a person is repeatedly vomiting or if the ketosis has not improved in 12 hours or has increased to more than 3.0 mmol/L then immediate referral to hospital is required.
Continuous glucose monitoring
Continuous glucose monitoring (CGM) uses a sensor electrode in the subcutaneous tissue separate from the insulin pump delivery site, which is linked to a transmitter that sends a Bluetooth signal to the insulin pump to display the current glucose level (Figures 1b and c and Figure 2). The Medtronic insulin pumps if paired with continuous glucose monitoring can stop insulin delivery when the blood glucose level is low and can alarm for high and low blood glucose levels; the Medtronic 640G pump can also suspend before ‘low’.The Animas pump can be paired with the Dexcom continuous blood glucose monitoring system, with the glucose level similarly displayed on the insulin pump, and can also be linked to a smart phone; however, with this system there is no interaction with the pump insulin delivery and there are no alarms for low blood glucose levels. There is a 10-minute lag between changes in venous blood glucose levels and sensor (interstitial fluid) glucose levels and the differences between the two readings will be greatest when blood glucose concentrations are changing rapidly.
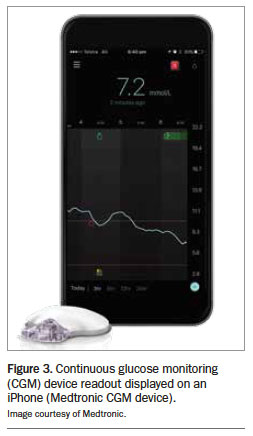
Both Animas and Medtronic have CGM systems that can be used by people on multiple daily injection regimens, with the signal sent to a smart phone and/or reader that the user wears (Figure 3).
{kind=link}
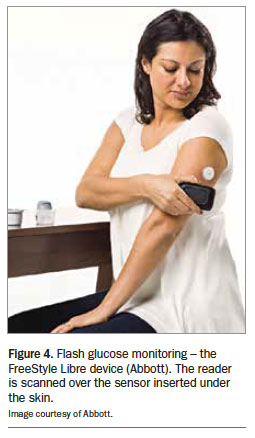
Flash glucose monitoring is now also available. This technology can provide a continuous retrospective CGM read-out when a sensor inserted just below the skin is scanned with a reader every eight hours. Although it cannot alert individuals to low blood glucose levels in the absence of a device reading, flash glucose monitoring does not require fingerstick testing to calibrate (as it is factory calibrated) and makes it easier for people with diabetes to perform glucose testing more frequently. The device available in Australia is the Freestyle Libre (Figure 4). Testing blood glucose more than four times a day has been shown to lower glycated haemoglobin by 9 mmol/mol (0.9%).3
{kind=link}
The principal benefits of flash monitoring and CGM are to detect unrecognised hypoglycaemia and enable the individual to address hyperglycaemia by administering correction doses of insulin more frequently. The information can be used to guide adjustments in regular insulin doses to prevent recurring hypo- and hyperglycaemia.
Smart glucose meters and phone apps
Smart glucose meters and phone apps can allow the concept of bolus dosing used with insulin pumps to be applied to people with type 1 diabetes on multiple daily injection insulin regimens. With these devices, they can calculate rapid-acting insulin doses to match food intake and correct blood glucose levels to set targets, provided they are using long-acting insulins (detemir or glargine).
A smart glucose meter allows the person to check their blood glucose level and enter the amount of carbohydrates they plan to eat. The meter will then advise a dose of rapid-acting insulin. Smart meters can also include active insulin in the calculation. These meters are devised to reduce the burden of diabetes care, removing the need to ‘guess’ doses of insulin required, but do require users to test blood glucose levels before all meals to be able to use the bolus calculator.
Phone applications are also available to assist in calculating bolus doses for meals.
Conclusion
Understanding the new technology being used by people with type 1 diabetes is important as it is rapidly changing the way they manage their blood glucose levels. Health professionals need to keep up with new innovations to feel comfortable managing people with type 1 diabetes both now and into the future. MT
References
- Phelan H, Clapin H, Bruns L, et al. The Australasian Diabetes Data Network: first national audit of children and adolescents with type 1 diabetes. Med J Aust 2017; 206: 121-125.
- Xu S, Alexander K, Bryant W, et al. Healthcare professional requirements for the care of adult diabetes patients managed with insulin pumps in Australia. Intern Med J 2015; 45: 86-93.
- Pfützner A, Weissman J, Mougiakakou S, Daskalaki E, Weis N, Ziegler R. Glycemic variability is associated with frequency of blood glucose testing and bolus: post-hoc analysis results from the ProAct study. Diabetes Technol Ther 2015; 17: 392-397.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.