Peer Reviewed
Gastroenterology clinic
Is it childhood coeliac disease? Separating the wheat from the chaff

Dr McIntyre is a Paediatric Gastroenterologist at Mater Medical Centre, Brisbane, Qld.
SERIES EDITOR: Dr Katherine Ellard MB BS, FRACP, Honorary Secretary of the Gastroenterological Society of Australia (GESA).
The views published in this series are those of the authors and not necessarily indicative of those held by all members of the Digestive Health Foundation or GESA.
Recent articles on:
Coeliac disease
Coeliac disease
Recent articles on:
Digestive diseases
Digestive diseases
Abstract
Coeliac disease is relatively common in children and screening is recommended for those with possible symptoms or conditions that increase risk. The diagnosis should be confirmed before a gluten-free diet is begun.
Remember
- Coeliac disease is an immune-mediated systemic disorder that occurs in response to gluten protein, causing villous atrophy of the small bowel and consequently affecting nutrient absorption. It is estimated to affect approximately 1% of the Australian population and may be increasing in prevalence.1
- Coeliac disease should be suspected in children with symptoms such as chronic diarrhoea, reduced appetite, abdominal pain and bloating, poor growth, weight loss or delayed menarche.
- Other presentations in children include lethargy, unexplained iron deficiency, constipation, poor concentration and school failure, mood disturbance, neurological symptoms, dental enamel defects and recurrent mouth ulceration.2
- Rarer presentations in childhood include a characteristic skin rash (dermatitis herpetiformis), abnormal liver function test results or so-called ‘coeliac crisis’, with explosive watery diarrhoea, significant abdominal distension, electrolyte disturbance and hypotension.
- Symptom onset may be at any age, but gluten intake is required to trigger symptoms, and therefore infants who have not yet been exposed to gluten or older children who have been maintained on a gluten-free diet will not show symptoms of coeliac disease.
- Children with positive coeliac serological results should be referred to a paediatric gastroenterologist for further investigation.
Assessment
Who should be screened for coeliac disease?
- Universal screening for coeliac disease is not recommended.
- Screening is advised for children who have:
- symptoms potentially caused by coeliac disease (see above)
- associated conditions that increase the risk of coeliac disease, including type 1 diabetes, selective immunoglobulin (Ig) A deficiency, thyroid disease, trisomy 21, Williams syndrome and Turner syndrome
- first-degree relatives with coeliac disease (first-degree relatives of people with coeliac disease have a lifetime risk of developing the disease of approximately 10%, and should be counselled about this risk and screened).
Advertisement
How to screen for coeliac disease
Gluten challenge
- It is important that children have sufficient gluten intake before screening.
- Children who have a normal diet usually consume sufficient gluten and do not require a specific gluten challenge before testing. Children or infants who have been placed on a gluten-free diet before the diagnosis of coeliac disease is established require a gluten challenge before testing.
- The usual gluten requirement to avoid a false-negative result is 10 to 15 g of gluten per day for approximately three months, which can usually be achieved with two to three gluten-containing meals per day. One slice of bread or four tablespoons of pasta contain 2 to 3 g of gluten. Younger children may find it difficult to consume this amount of gluten, and so parents should be advised to try to include gluten-containing food in each meal.
Coeliac serological testing
- Initial screening for coeliac disease requires serological testing of blood, usually for:
- IgA antibodies to tissue transglutaminase (TTG)
- IgG antibodies to gliadin
- total IgA levels (as patients with IgA deficiency may have a false-negative TTG result).
- In individuals without IgA deficiency, the sensitivity and specificity of the TTG IgA test is approximately 95%, although it may be lower in young children.3
- Antigliadin IgG is not as sensitive or specific for coeliac disease as anti-TTG IgA and is mostly useful in patients with IgA deficiency.
- A positive anti-TTG result alone is not sufficient to diagnose coeliac disease, and children should not be started on a gluten-free diet on this basis. Instead, children with positive coeliac serological results should be referred to a paediatric gastroenterologist for further assessment.
Coeliac HLA-DQ typing
- Coeliac disease is associated with specific variants of the human leukocyte antigens HLA-DQ2 and HLA-DQ8.
- Coeliac HLA-DQ genotyping can be useful in patients with possible coeliac disease who are on a gluten-free diet but have not had coeliac disease confirmed. Negative results for HLA-DQ2 and HLA-DQ8 make the diagnosis of coeliac disease extremely unlikely.
- A positive HLA-DQ2 or HLA-DQ8 result alone does not make the diagnosis of coeliac disease, and the patient should undergo serological testing after adequate gluten exposure (see ‘Gluten challenge’ above). Approximately 55% of the Australian population are positive for coeliac HLA types.4
- If an asymptomatic child is positive for HLA-DQ2 or HLA-DQ8 but has negative serological results despite adequate gluten intake then it may be recommended that they have repeat serological testing every three years while they remain asymptomatic or gastrointestinal endoscopy if they develop symptoms.5 However, this approach might lead to overinvestigation, given the high prevalence of HLA-DQ2 and HLA-DQ8 types in the community.
Upper gastrointestinal endoscopy
- Children with positive coeliac serological results should be referred to a paediatric gastroenterologist for consideration of upper gastrointestinal endoscopy and small bowel biopsy.
- Children with negative serological results but symptoms suggestive of coeliac disease should also be referred to a paediatric gastroenterologist or paediatrician with an interest in coeliac disease for further advice.
- Under certain circumstances, an endoscopy and small bowel biopsy may be avoided, but this should be on the advice of a paediatric gastroenterologist after review of the child and discussion with the parents.6
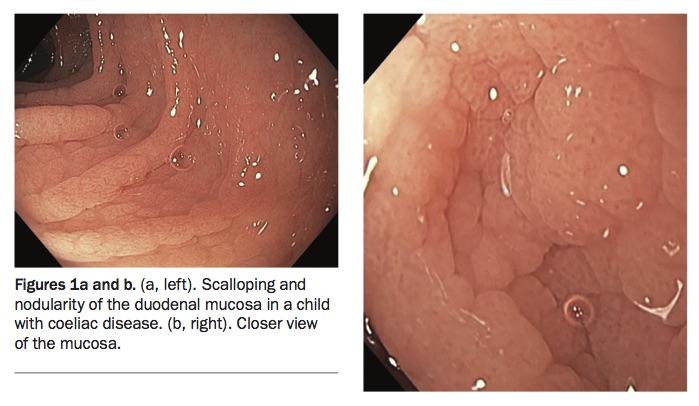
- Endoscopic changes in the small bowel suggestive of coeliac disease include scalloping, nodularity, loss of mucosal folds, villous atrophy and mosaic pattern (Figures 1a and b). However, these changes lack specificity and sensitivity, and a biopsy of the duodenum should be undertaken.
{kind=link}
Biopsy changes
- Small bowel biopsy specimens from children with coeliac disease show a variable degree of inflammation and villous atrophy.
- The standard assessment tool is the modified Marsh grading system (types 0 to 4) as follows.
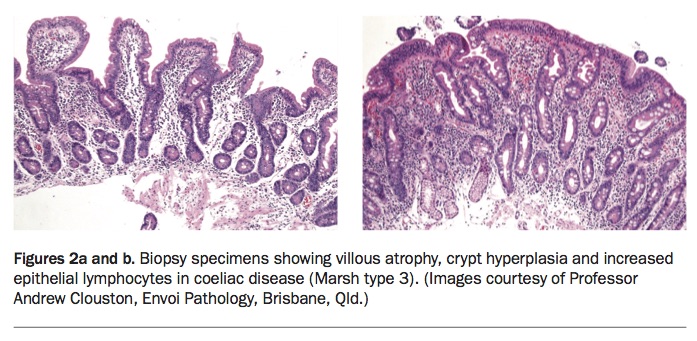
- Marsh type 3 (villous atrophy with crypt hyperplasia and increased intraepithelial lymphocytes [IEL]) is characteristic of coeliac disease (Figures 2a and b). Marsh type 4 (hypoplastic or completely atrophic mucosa) is not usually seen in children.
- Marsh type 1 (IEL alone) and type 2 (IEL with crypt hyperplasia) should be interpreted on a case-by-case basis with consideration given to gluten exposure and serological and HLA typing results.
{kind=link}
Management
Initial management
- Following histological confirmation of the diagnosis of coeliac disease, the child should begin a gluten-free diet with support from a qualified paediatric dietitian. The diet must be continued lifelong.
- A lactose-free diet may be needed temporarily until the small bowel mucosa recovers and lactase levels return to normal.
- Coeliac Australia is a useful resource for parents of children with coeliac disease (https://www.coeliac.org.au).
Advertisement
Monitoring
- Regular monitoring with checking of dietary adherence, symptoms, growth and micronutrient status and physical examination is necessary.
- Anti-TTG antibodies should be checked six to 12 months after the child starts a gluten-free diet.
- Normalisation of anti-TTG antibodies takes longer than 12 months in 75% of children, especially those with the highest initial antibody levels or the most severe mucosal injury at diagnosis.7
- Continued abnormal anti-TTG antibodies should prompt review by a dietitian to identify any nonadherence to a gluten-free diet. If a source of gluten cannot be found in the diet then repeat endoscopy may be required.
Noncoeliac gluten sensitivity
- Noncoeliac gluten sensitivity is a diagnosis applied to children who have reproducible symptoms in response to gluten ingestion but negative serological and biopsy results for coeliac disease.
- The pathophysiology of noncoeliac gluten sensitivity is unknown. In some cases, symptoms may be due to IgE-mediated wheat allergy. In these circumstances, symptoms are typical of IgE-mediated allergy, such as itching, swelling, wheeze, rash or anaphylaxis. These patients should be assessed by an allergist.
- Other children may present with symptoms such as recurrent abdominal pain and diarrhoea. It is unclear whether this is a response to gluten or to associated fermentable compounds found in grain products. If coeliac disease is excluded then it is reasonable to manage these children with a short-term gluten-free diet and periodic reintroduction of gluten to test tolerability.8
Conclusion
- Coeliac disease is a relatively common disease in childhood. Serological testing should be performed when there is clinical suspicion, and children with positive results should be referred to a paediatric gastroenterologist.
- A gluten-free diet should not be commenced without confirmation of the diagnosis. MT
COMPETING INTERESTS: None.
References
1. Anderson RP. Coeliac disease is on the rise. Med J Aust 2011; 194: 278-279.
2. Khatib M, Baker R, Ly E, et al. Presenting pattern of pediatric celiac disease. J Pediatr Gastroenterol Nutr 2016; 62: 60-63.
3. Giersiepen K, Lelgemann M, Stuhldreher N, et al; ESPGHAN Working Group on Coeliac Disease Diagnosis. Accuracy of diagnostic antibody tests for coeliac disease in children: summary of an evidence report. J Pediatr Gastroenterol Nutr 2012; 54: 229-241.
4. Anderson RP, Henry MJ, Taylor R, et al. A novel serogenetic approach determines the community prevalence of celiac disease and informs improved diagnostic pathways BMC Med 2013; 11: 188.
5. Coeliac Working Group of the British Society of Paediatric Gastroenterology Hepatology and Nutrition (BSPGHAN). Guideline for the diagnosis and management of coeliac disease in children. Available online at http://www.bspghan.org.uk (accessed October 2017).
6. Husby S, Koletzko S, Korponay-Szabo I. ESPGHAN guidelines for the diagnosis of coeliac disease in children and adolescents. An evidence-based approach. J Pediatr Gastroenterol Nutr 2012; 54: 136-160.
7. Gidrewicz D, Trevenen CL, Lyon M, Butzner JD. Normalization time of celiac serology in children on a gluten-free diet. J Pediatr Gastroenterol Nutr 2017; 64: 362-367.
8. Meijer C, Shamir R, Mearin M. Celiac disease and non-celiac gluten sensitivity. J Pediatr Gastroenterol Nutr 2015; 60: 429-432.
Get full access
Buy this article
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.
Already a subscriber? Login here.