Stroke prevention: medical interventions for everyday practice

Stroke
Transient ischaemic attack
Although many strokes are preventable, it can be challenging to assess the risk versus benefit of therapy in individual patients, particularly regarding anticoagulation. Patients with atrial fibrillation generally require anticoagulation to reduce the risk of stroke, yet patients at highest risk often remain undertreated. Early antiplatelet therapy after minor stroke or transient ischaemic attack reduces risk of recurrent stroke.
- Paroxysmal or permanent atrial fibrillation associated with a CHA2DS2-VASc score of one or more for men and two or more for women should prompt consideration of anticoagulation to reduce stroke risk.
- High-risk patients with atrial fibrillation remain significantly undertreated; older patients, despite having a high risk of falls, are nevertheless likely to benefit from anticoagulation.
- Perioperative bridging anticoagulation for patients with atrial fibrillation is not routinely recommended; direct oral anticoagulant drugs should be ceased 24 to 48 hours before procedures.
- Asymptomatic carotid atherosclerotic disease should be treated medically.
- Antiplatelet medication for secondary prevention has most benefit when given early after stroke or transient ischaemic attack.
Picture credit: © KO Studios
General practitioners play a central role in primary and secondary prevention of stroke. A large proportion of stroke is preventable, yet risk factor modification remains suboptimal, and individualising the balance of risk and benefit, particularly regarding anticoagulation, can be challenging. This review explores key strategies in the management of atrial fibrillation (AF) and carotid artery disease, as major causes of stroke, as well as the use of antiplatelet agents and potential barriers to optimal management.
Atrial fibrillation and stroke
AF is the most common chronic atrial arrhythmia diagnosed in patients with stroke.1 The risk of stroke is similar in both paroxysmal and permanent AF. A central message of this article is that more patients with AF need anticoagulation prescribed to reduce the risk of stroke. Although it is appropriate for low-risk patients to receive no intervention, older patients with comorbidities are suitable for anticoagulation but remain significantly undertreated. Aspirin no longer has a role in stroke prevention for patients with AF.
As a medical community, general practitioners, emergency physicians and hospital doctors need to be more vigilant about commencing appropriate anticoagulation in a timely manner. More anticoagulant medications have become available in recent years with the introduction of direct oral anticoagulants (DOACs), such as apixaban, dabigatran and rivaroxaban. The DOACs are also commonly known as NOACs, initially meaning ‘novel’ oral anticoagulants, then, when they were no longer novel, ‘nonvitamin K antagonist’ oral anticoagulants. However, there appears to be growing consensus that the acronym DOAC is more widely applicable and less likely to be misunderstood as meaning ‘no anticoagulants’.2 The term DOAC will be used here.
Prevalence of atrial fibrillation
The American College of Cardiology Foundation and American Heart Association estimate that the prevalence of AF in the USA ranges from 0.4 to 1.0%.3 However, more recent Swedish data found a prevalence of at least 2.9% of the adult population (aged 20 years or older) and suggest that the official US figures probably underestimate the magnitude of the problem by a factor of three to five.4 More than 80% of patients in the Swedish study had risk factors that would have made anticoagulation therapy beneficial.
In Australia, a longitudinal study from Adelaide indicated a prevalence of AF in hospital patients aged under 60 years of 1.73% for nonIndigenous people and 2.57% for Indigenous people.5 In patients aged 60 years or older, however, the prevalence was 9.26% and 4.61% for nonIndigenous and Indigenous patients, respectively.5
Undertreatment in atrial fibrillation
The data from Sweden raise several pertinent points:4
- 83% of patients with AF had an indication for anticoagulation, yet only 42% had purchased warfarin in the preceding six months
- paradoxically, those at the highest risk of stroke were the least likely to receive warfarin
- there was a decrease in the likelihood of receiving warfarin with increasing stroke risk
- in contrast, the likelihood of receiving aspirin increased almost linearly with increasing stroke risk.
Proposed explanations were that high-risk patients were considered too high risk for anticoagulants. Thus, aspirin was given instead, despite aspirin providing a weak protective effect and having bleeding risks similar to those from well-managed warfarin use. Warfarin was prescribed less often to patients aged over 80 years and less often to women than men, despite both increasing age and female sex being high-risk features of stroke.
Which anticoagulant for atrial fibrillation?
Choosing the correct anticoagulant agent for a patient is important, with the initial consideration being whether they have valvular AF or nonvalvular AF. Valvular AF is defined as AF with:
- moderate to severe mitral stenosis (including rheumatic heart disease)
- a mechanical prosthetic heart valve.
It is recommended that these patients receive warfarin for anticoagulation. Patients with nonvalvular AF include all those with AF that does not meet these criteria.
For patients with nonvalvular AF and adequate renal function, the DOACs have the advantages of a reduced rate of intracerebral haemorrhage, similar (or in some cases reduced) risk of ischaemic stroke and convenience, given their reduced monitoring requirements and drug interactions.
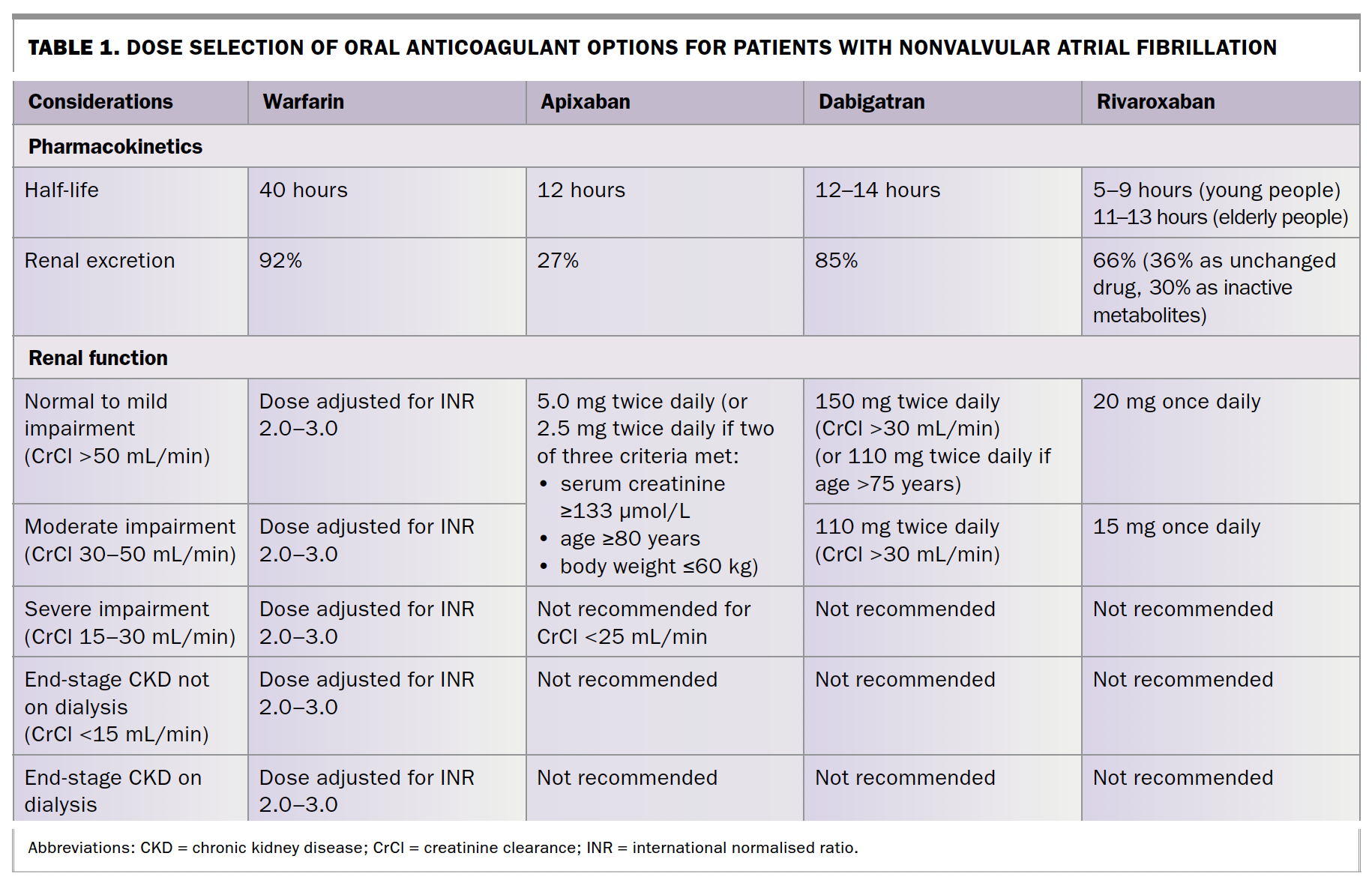
When choosing a DOAC, it is important to also choose the correct dose. Prescribing patterns indicate a tendency to reduce the dose inappropriately.6 The criteria for selecting DOAC doses are listed in Table 1. Inadequate doses subject the patient to a risk of bleeding without the full benefit of ischaemic stroke risk reduction.
{kind=link}
The impact of renal function
Impaired renal function is a common problem in patients with chronic disease, such as hypertension. Creatinine clearance should be calculated using the Cockcroft–Gault formula (not an estimated glomerular filtration rate, which is too inaccurate). Care needs to be taken with DOACs in patients with renal impairment, as accumulation of the drug secondary to poor excretion may increase bleeding risk.
Dabigatran and rivaroxaban may be used for patients with creatinine clearance of more than 30 mL/min, and apixaban for patients with a creatinine clearance of more than 25 mL/min. Below this level warfarin remains the drug of choice, although interestingly US and European licences allow DOAC use if creatinine clearance is more than 15 mL/min.
Patients with borderline renal function need close monitoring of creatinine clearance during acute illness to maintain safety when using anticoagulants.
Who should receive anticoagulants?
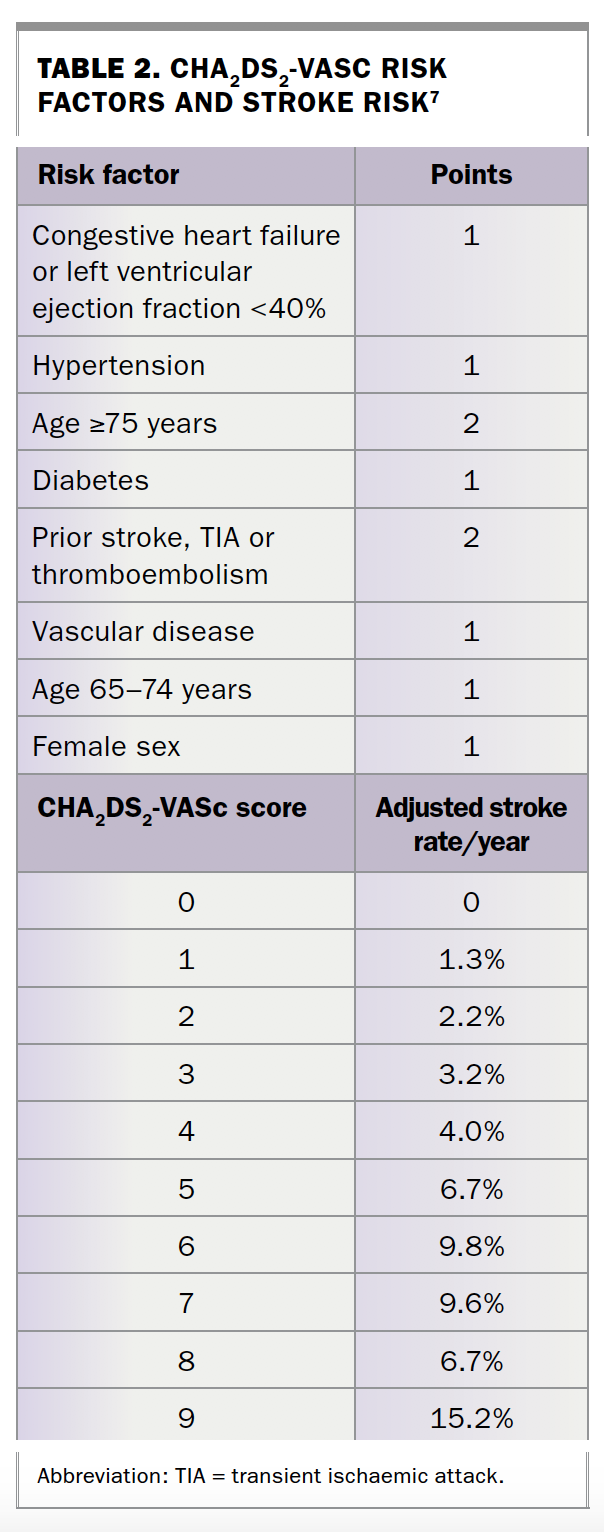
Paroxysmal and permanent AF should be considered as having similar risk profiles and therefore be treated equally. Two common risk scores to determine patients’ yearly stroke risk are CHADS2 and CHA2DS2-VASc (Table 2).7 Any CHADS2 points are an indication for anticoagulation. CHA2DS2-VASc is useful for more precise risk stratification of those with a CHADS2 score of 0, particularly older women, who are redistributed from the low-risk to high-risk category using this classification.
{kind=link}
Guidelines, including those of the European Society of Cardiology, recommend that men with a CHA2DS2-VASc score of one or more and women with a score of two or more should receive anticoagulation unless there is a contraindication.8 Trials of warfarin versus placebo showed a relative risk reduction of ischaemic and haemorrhagic stroke of 64%, with a number needed to treat of 37 for one year to prevent one stroke, and 12 for patients with prior stroke or transient ischaemic attack (TIA).1 The absolute risk reduction depends on patients’ inherent risk, and patients with a low CHA2DS2-VASc score therefore benefit less from anticoagulation in absolute terms.
Low-risk patients
Young patients (aged under 65 years) with nonvalvular AF and a CHA2DS2-VASc score of 0 have low (but not zero) risk of stroke, and recommendations from the European Society of Cardiology are that it is reasonable to omit antithrombotic therapy in these patients. Their benefit from anticoagulation is low. However, not all patients with a score of 0 or 1 will have the same risk of stroke, so the merits of anticoagulation should be discussed with each patient.
Patients at high risk of thrombosis and bleeding
Older patients (aged 65 years or older) with multiple comorbidities can pose a challenge. Risk of bleeding often goes hand in hand with risk of thrombosis. Impaired renal function, hypertension, advanced age and a risk of falls increase the risk of bleeding, yet all these factors also increase the risk of stroke in patients with AF.
Although the risk of bleeding increases in older patients, the benefit from anti-coagulation is significantly higher than in other populations. There is added risk with the presence of comorbidities such as hypertension, previous stroke and older age. As noted, these patients are least likely to receive anticoagulation and thus are exposed to a high risk of stroke.
Falls risk and aversion to prescribing anticoagulation
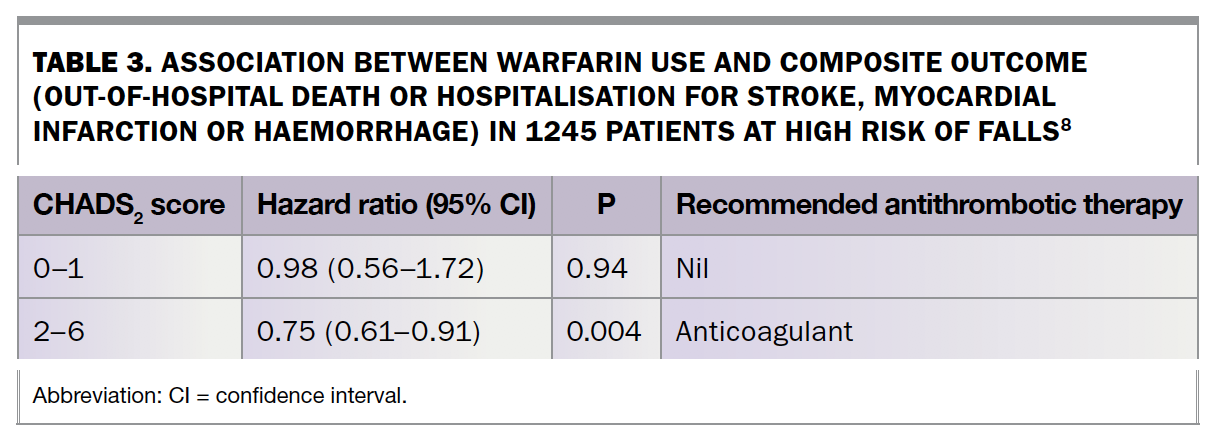
Practitioners will often withhold anticoagulation from patients because of a perceived risk of falls and traumatic intracranial bleeding. However, data clearly show that propensity to fall is not a contraindication to use of anticoagulation. Patients with a higher risk of falls also have a higher incidence of stroke and, after a stroke, their 30-day mortality is higher than in more mobile patients.9 Patients at high risk of falls and with a CHADS2 score of two or higher benefit from anticoagulation. Trials show a 25% relative risk reduction in the composite outcome of stroke, intracranial haemorrhage, myocardial infarction and death for these patients (Table 3).9
{kind=link}
Statistical analysis suggests that patients would have to fall up to 295 times in one year for the risks of subdural haemorrhage to outweigh the benefits of anticoagulation.10 However, it is worthwhile investigating the cause of falls and considering referral to a falls and balance clinic or a neurologist. Nonpharmacological precautions to limit the risk of falling include use of stable shoes, regular exercise, vitamin D supplementation, walking aids and discontinuation of unnecessary medications.9
Contraindications to anticoagulation
True contraindications to anticoagulation include active bleeding, bleeding that is not amenable to intervention (e.g. small bowel bleeding of unclear cause) and recent symptomatic and serious haemorrhage requiring hospitalisation or blood transfusion. Bleeding can be mitigated if the source of bleeding can be treated, such as with gastric or duodenal ulcers, with the avoidance of nonsteroidal medications or aspirin to reduce the rate of gastrointestinal ulceration, and with risk-reduction strategies such as Helicobacter pylori eradication. When anticoagulation is truly contraindicated, left atrial appendage closure may be considered as an alternative option to reduce stroke risk.
Ceasing anticoagulation before surgery
The Bridging Anticoagulation in Patients who Require Temporary Interruption of Warfarin Therapy for an Elective Invasive Procedure or Surgery (BRIDGE) trial published in 2015 was helpful in addressing the question of whether bridging anticoagulation (e.g. low-molecular weight heparin) is necessary before surgery in patients with AF taking warfarin.11 It found that discontinuing warfarin without bridging anticoagulation was noninferior to bridging anticoagulation.11 Avoiding bridging anticoagulation was associated with an almost threefold reduction in risk of major bleeding and with significantly less minor bleeding. There was no significant difference in myocardial infarction, venous thromboembolism or death. The net clinical benefit favoured a strategy of forgoing bridging anticoagulation.
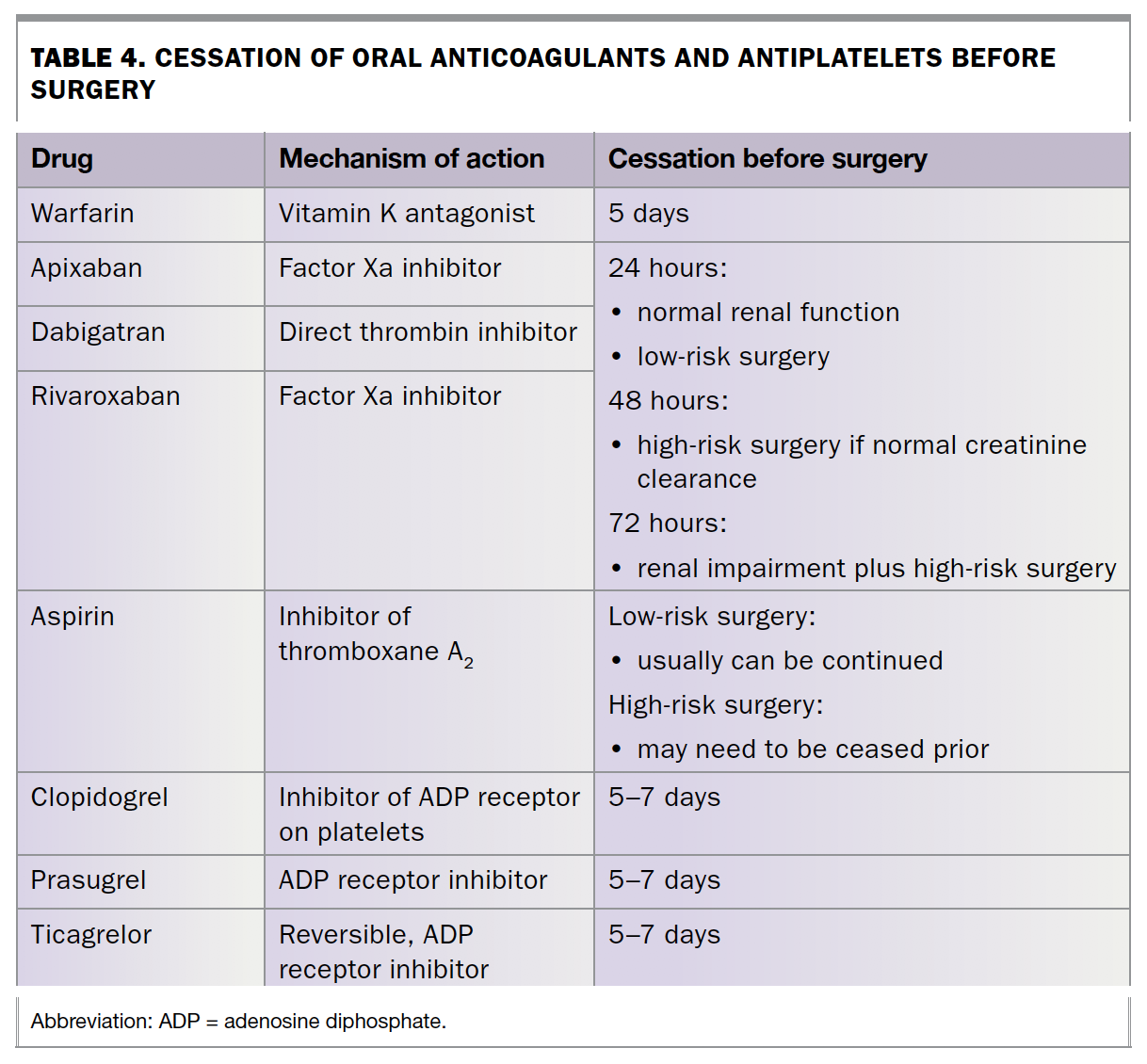
An important consideration in anti-coagulation cessation before surgery or other procedures is that the newer anticoagulant drugs, DOACs, do not need to be stopped five to 10 days beforehand. Stopping DOACs 24 to 48 hours prior is sufficient in most patients (Table 4) and reduces the time at risk without anticoagulation.
{kind=link}
The decision regarding bridging anticoagulation should be made in conjunction with the interventionist or surgeon and, in more complex cases, with advice from a haematologist.
Carotid artery disease and stroke
Carotid atherosclerosis is a major cause of ischaemic stroke. Although haemodynamically insignificant plaque can cause distal thromboembolism, the risk is higher for patients with more than 50% stenosis and particularly those with more than 70% stenosis.12 If carotid occlusion (or trickle flow) has developed without causing a severe stroke, this indicates good collaterals (alternative blood supply routes), and the risk of subsequent stroke is sufficiently low that intervention is not warranted. Intensive medical therapy with antiplatelet agents, a high-potency statin and medication to lower blood pressure (to a target of less than 140 mmHg systolic) is indicated for all patients with carotid stenosis.
Symptomatic carotid stenosis
Symptomatic stenosis more than 50% should prompt consideration of carotid endarterectomy.12 To date, carotid stenting has consistently been associated with increased periprocedural stroke risk in all trials, although it may be performed as part of an acute treatment with endovascular thrombectomy for large vessel occlusion stroke.13 As the risk of stroke is highest in the first few days after symptom onset (either TIA or stroke), investigation and referral for surgery is urgent. Once six weeks have elapsed without symptoms, the stroke risk returns to about the same level as in patients with asymptomatic stenosis.
Asymptomatic carotid stenosis
A key change in recommendations in recent years has been to avoid endarterectomy in patients with asymptomatic stenosis, as the risk of stroke during intensive medical therapy is felt to be lower than the upfront periprocedural risk of stroke.14 The key factor in determining whether endarterectomy is required is the presence of focal neurological symptoms referable to the ipsilateral hemisphere. ‘Dizziness’ and other nonfocal symptoms do not indicate a ‘symptomatic’ carotid stenosis, and carotid imaging is not recommended for the investigation of such symptoms.
Antiplatelet medications
Which agent and when to prescribe?
Deciding which antiplatelet to prescribe is often not as important as when an antiplatelet is prescribed, or for how long. Aspirin has been shown to be the most effective antiplatelet agent when given early after TIA or stroke, with most of the benefit seen in the first 12 weeks.15
The risk of recurrent stroke is up to 10% in the week after a TIA or minor stroke. Urgent medical treatment (antiplatelet, lipid-lowering agent, blood pressure control) seems to reduce that risk by as much as 80%, but many patients delay seeking medical attention, often for several days or weeks, even when they make a correct self-diagnosis.15
TIA or minor stroke requires urgent treatment, with aspirin being the first-line antithrombotic therapy. The options for antiplatelet therapy include:
- aspirin
- aspirin–dipyridamole
- clopidogrel
- aspirin plus clopidogrel (short term only).
There is a small benefit of using clopidogrel alone or aspirin–dipyridamole compared with aspirin alone. Trials examining dual antiplatelet therapy (aspirin plus clopidogrel) for long-term secondary prevention failed because of excessive bleeding complications. A single randomised controlled trial in China showed reduced stroke recurrence with short-term (21 days) dual antiplatelet therapy (aspirin plus clopidogrel) followed by clopidogrel alone.16 However, the benefit was predominantly seen in patients with intracranial atherosclerosis, which is uncommon in western populations. In another trial, ticagrelor was not found to be superior to aspirin in reducing the rate of stroke, myocardial infarction or death at 90 days.17
How long to prescribe for?
How long antiplatelet medications should be prescribed for is an important consideration. After TIA or stroke, a single antiplatelet agent is typically prescribed for the rest of the patient’s life. If the mechanism of stroke is AF, an anticoagulant should be prescribed in place of an antiplatelet drug. Patients are more commonly prescribed dual antiplatelet medications after cardiac stenting (due to the risk of in-stent thrombosis) than after stroke. Patients who are taking dual antiplatelet medications and an anticoagulant, often for AF, have increased risk of bleeding.
It is important to determine how long a patient should continue taking dual antiplatelets. The duration of dual antiplatelet prescription is typically:
- 12 months after coronary artery stenting
- six months for carotid artery stenting
- one to three months for stroke patients with atherosclerotic vascular disease.
Duration should be decided in consultation with the treating specialist, but prolonged use of dual antiplatelets (longer than six to 12 months), especially if concurrent anticoagulation is being used, confers significant bleeding risk without necessarily conferring ongoing benefit.
Key steps in the management of TIA and minor stroke
TIA and minor stroke present a major opportunity to prevent disabling stroke. The key investigations are carotid and brain imaging and an ECG looking for AF. An antiplatelet agent (usually aspirin) can be commenced as soon as brain imaging has excluded haemorrhage, unless AF has been diagnosed, in which case anticoagulation can be commenced in place of an antiplatelet agent. Anticoagulation can be commenced immediately in the case of TIA and after a few days for minor stroke.
A high-potency statin (e.g. 80 mg atorvastatin or 40 mg rosuvastatin) can be commenced immediately after TIA or minor stroke. Blood pressure-lowering medication can be commenced or intensified to achieve a systolic blood pressure consistently less than 140 mmHg. Whether lower blood pressure targets are beneficial in stroke patients is the subject of ongoing trials. Paroxysmal AF can be difficult to detect and longer-term monitoring, or at least opportunistic pulse checks at every visit, is worthwhile.
The risk of stroke in patients with symptomatic carotid stenosis is highest in the first few days after symptoms appear, and carotid imaging is recommended as soon as possible (certainly within 48 hours). This may be best achieved through immediate referral to the local hospital emergency department or TIA clinic, depending on local resources.
For the purposes of identifying candidates for endarterectomy and commencing appropriate medications, a carotid Doppler ultrasound and CT brain scan are adequate. Risk stratification scores (e.g. ABCD2) are not recommended to triage the urgency of investigation, because they miss high-risk features such as AF and symptomatic carotid stenosis. Diagnostic accuracy is therefore the best approach to prioritise investigations. Clinical features of common TIA mimics are well described,18 and specialist assessment can also be helpful when available.
The Stroke Foundation has recently updated the NHMRC-approved Australian Clinical Guidelines for Stroke Management (www.informme.org.au/guidelines).
Conclusion
Stroke prevention is the cornerstone of reducing rates of stroke in the community. Primary prevention includes the detection of AF and prescription of anticoagulation to those patients who will benefit, using risk scores such as CHA2DS2-VASc. Higher-risk patients with AF continue to be undertreated and risk experiencing large disabling strokes. The use of antiplatelet medication for secondary prevention has most benefit if given early after stroke or TIA. Asymptomatic carotid atherosclerotic disease should be treated medically, whereas symptomatic carotid disease should prompt urgent treatment, primarily carotid endarterectomy. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.