Acute stroke: preventing stroke and managing complications
GPs are ideally placed to identify patients with modifiable risk factors for stroke and to institute prevention strategies, including lifestyle changes and antihypertensive and anticoagulation therapy when appropriate. GPs can also help reduce morbidity in stroke survivors through recognising and managing complications such as depression, sexual dysfunction and fatigue.
- Stroke is a leading cause of death and disability in Australia.
- All patients with suspected stroke and ongoing symptoms should be sent immediately to a hospital emergency department, and all with transient neurological deficits should be urgently referred to a transient ischaemic attack clinic.
- Stroke can be categorised by noncontrast CT as ischaemic or haemorrhagic; ischaemic stroke is more common and may be due to small-vessel disease, cardioembolism or extracranial atherosclerosis.
- Antihypertensive therapy, statins and, if atrial fibrillation is not detected, antiplatelet therapy form the mainstays of secondary prevention; if atrial fibrillation is detected, anticoagulation is required.
- Lifestyle modification is a key component of stroke prevention: all patients should be encouraged to increase consumption of fruit and vegetables and reduce salt intake; those who are sedentary should be encouraged to increase physical activity.
- GPs are ideally placed to identify common complications in stroke survivors, such as depression, fatigue and sexual dysfunction, and to initiate treatment or refer as appropriate.
Stroke is a leading cause of death and disability in Australia. The role of the GP is crucial in implementing strategies that reduce the prevalence of stroke through identifying patients who are at high risk of developing cerebrovascular disease and initiating therapies that modify risk. Finally, GPs can reduce morbidity associated with stroke through identification and management of poststroke complications.
In this review, we summarise key points about stroke epidemiology, investigation, primary and secondary prevention, and management of common poststroke complications.
Significance of stroke
Stroke is a major source of morbidity and mortality. The World Stroke Organization estimates that stroke currently has a global point prevalence of 80 million and accounts for 5.5 million deaths annually.1
In Australia, the Stroke Foundation estimates there are about 500,000 stroke survivors, making stroke one of the leading causes of acquired disability and death.2 Furthermore, stroke is estimated to cost Australian tax payers $5 billion per year.2
About 72% of stroke burden is due to modifiable risk factors, such as hypertension, dyslipidaemia and impaired glucose tolerance, and about 66% of stroke is due to behavioural factors such as smoking and physical inactivity.1 These proportions underscore the importance of public health initiatives and primary health care in stroke prevention.
Stroke presentation and stroke mimics
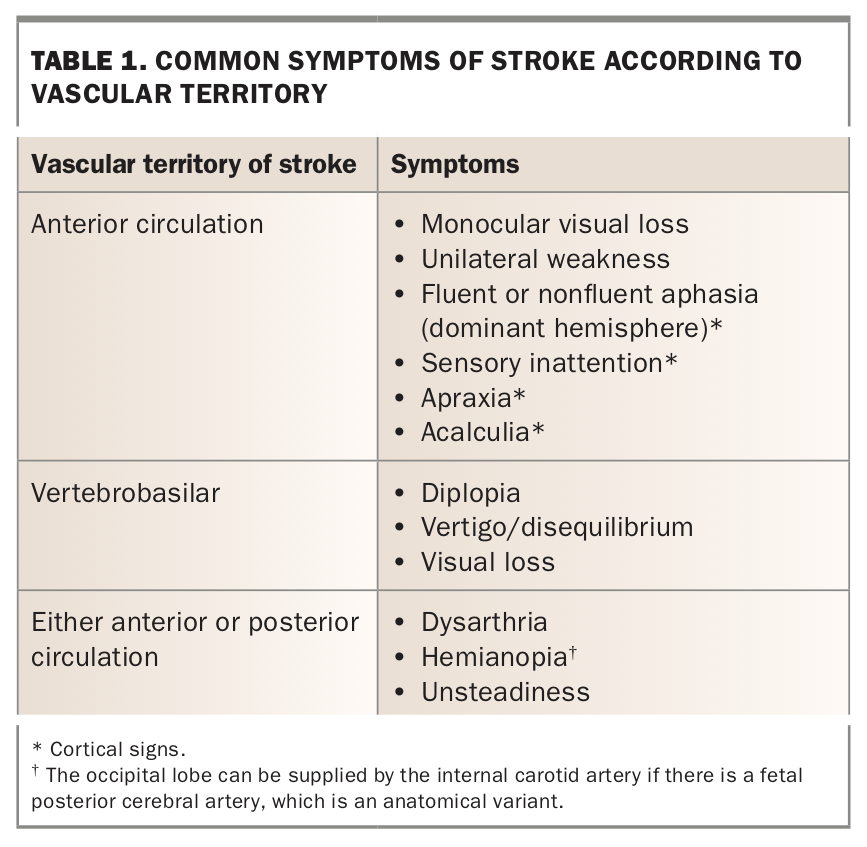
Stroke is a phenotypically heterogeneous disease in which presentation depends on the size of the lesion and the vascular territory affected. The common presentations according to vascular territories are characterised in Table 1. In general, strokes are characterised by the presence of negative symptoms, such as weakness, which reach maximum intensity over seconds. A transient ischaemic attack (TIA) is defined as the presence of stroke-like symptoms that fully resolve within 24 hours. A proportion of TIAs are later reclassified as stroke when tissue damage is visible on subsequent neuroimaging (usually MRI).
{kind=link}
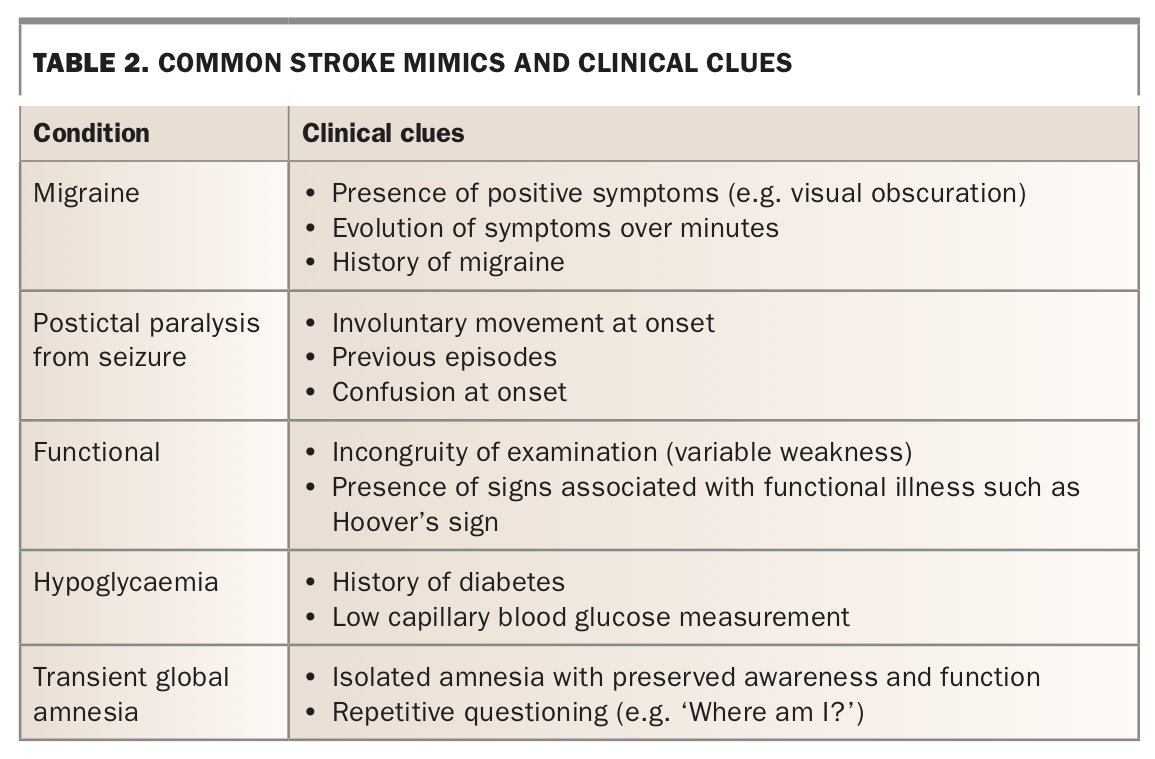
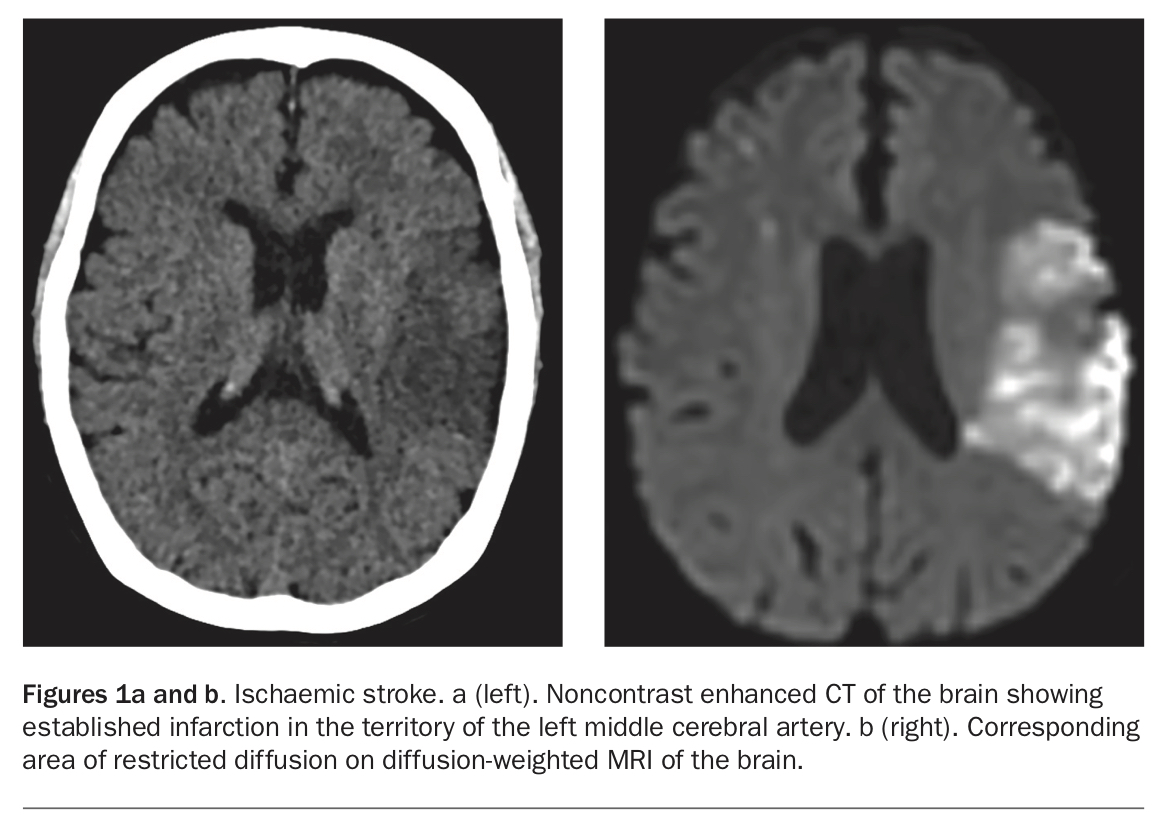
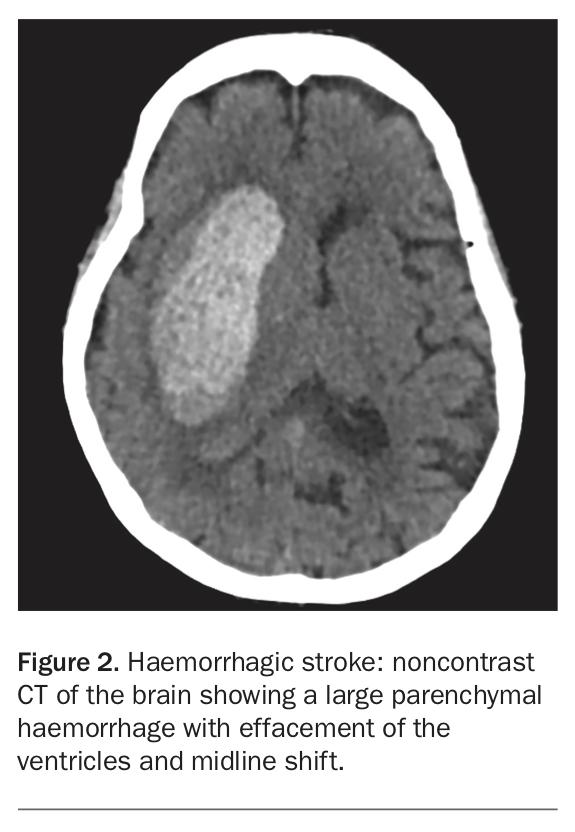
Some patients admitted to stroke units or seen at stroke clinics have an alternative diagnosis. These conditions are referred to as stroke mimics (Table 2). MRI can help clinicians differentiate stroke from stroke mimics and can provide insight into the likely mechanism of stroke for both ischaemic and haemorrhagic stroke types (Figure 1 and Figure 2).
{kind=link}
{kind=link}
Patients with suspected stroke require an urgent and comprehensive assessment to determine eligibility for reperfusion therapies such as intravenous alteplase, which is licensed for use up to 4.5 hours after symptom onset, or endovascular clot retrieval. GPs have a crucial role in identifying patients who present with possible stroke or TIA. All patients with suspected stroke and ongoing symptoms should be sent immediately to a hospital emergency department by ambulance with ‘lights and sirens’. The ambulance can pre-notify the emergency department to facilitate prompt assessment of the patient on arrival. As some hospital emergency departments do not offer a thrombolysis service, ambulance services will bypass these hospitals in favour of a stroke centre where possible. All patients with transient neurological deficits should be urgently referred to a rapid access TIA clinic, where available. If no rapid access clinic is available or an appointment cannot be organised within one week then evaluation in a hospital emergency department is safest.
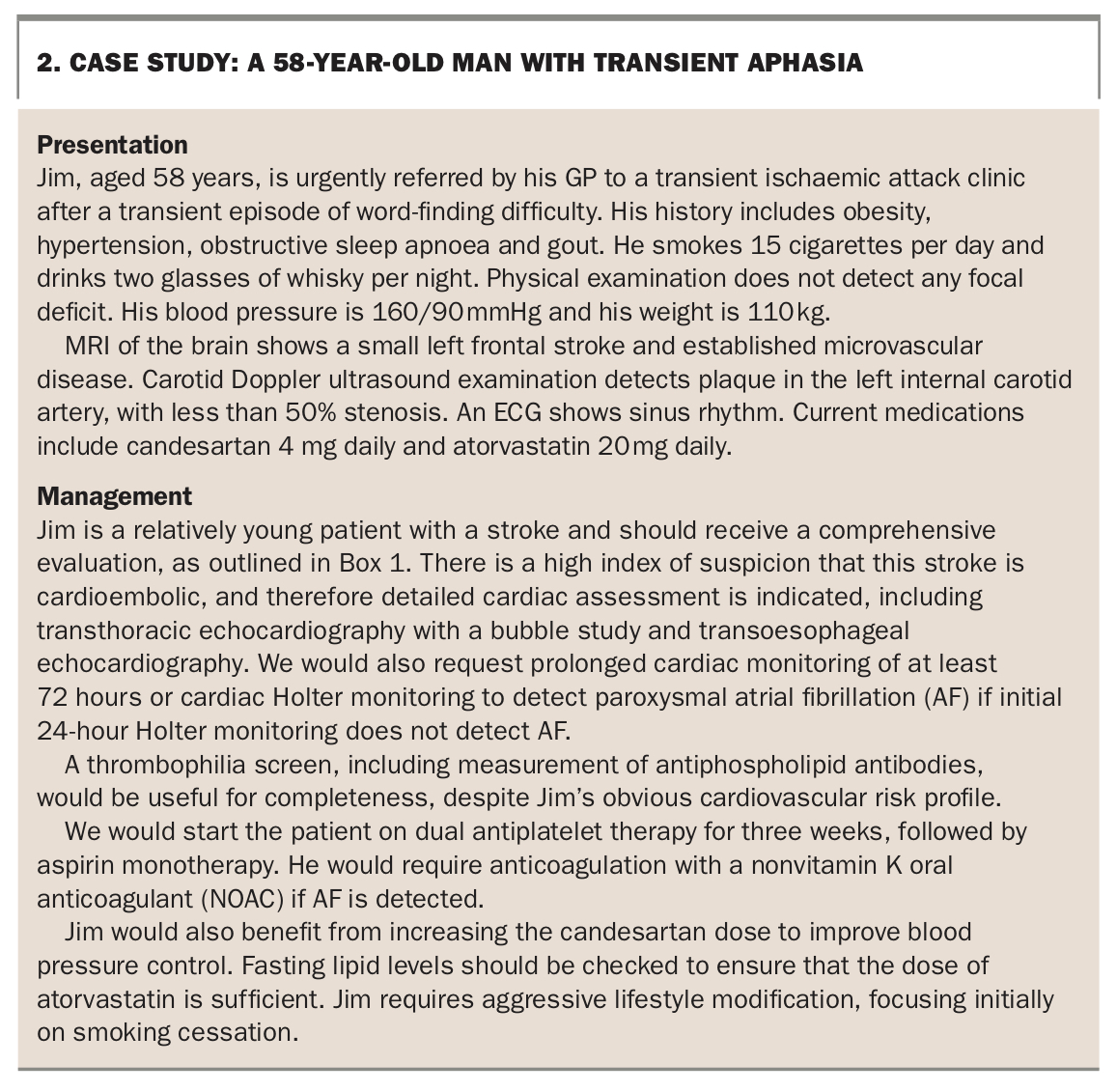
Essential investigations for all patients and useful additional investigations for selected patients are listed in Box 1.3 A case scenario of a patient with symptoms suggesting a TIA is described in Box 2.
{kind=link}
{kind=link}
Classification of stroke: ischaemic or haemorrhagic?
Strokes can be differentiated into:
- ischaemic strokes, caused by interruption of arterial blood supply
- haemorrhagic strokes, caused by ruptured blood vessels.
The distinction is crucial as management differs. Evaluation is based on initial noncontrast CT of the brain (see Figure 1a and Figure 2 for a comparison). The following discussion refers to ischaemic stroke unless otherwise specified.
{kind=link}
Types of ischaemic stroke
Ischaemic stroke can be further subclassified according to the presumed aetiology. The major categories of ischaemic stroke are embolic stroke, lacunar stroke and stroke associated with large vessel disease.
Embolic strokes
Embolic strokes are derived from the heart. The various cardiac causes of embolic stroke are listed in Box 3. The most common cause is atrial fibrillation (AF). Embolic strokes are usually suspected when there are cortical deficits on clinical examination, such as aphasia. Alternatively, embolic stroke may be apparent on imaging if there are strokes in multiple vascular territories or cortical involvement. Embolic stroke can result in devastating strokes, and epidemiological studies suggest that the proportion of strokes that are embolic is increasing.4
Lacunar stroke
Lacunar strokes (lacunes) are small, subcortical or brainstem infarcts caused by occlusion of small perforating vessels (end-arteries that lack a collateral blood supply). The occlusion is usually the consequence of small vessel disease, characterised pathologically by lipohyaline change with superimposed microatheroma.5 The process is usually accelerated by chronic hypertension, diabetes or dyslipidaemia.
Lacunar strokes are usually smaller than embolic strokes but can be severely disabling if they affect white matter tracts, such as the internal capsule, which would result in contralateral hemiplegia. Lacunar strokes are not associated with cortical deficits. About 20 lacunar syndromes have been characterised, including pure motor hemiparesis, pure sensory, pure sensorimotor hemiparesis, ataxic hemiparesis and clumsy-hand dysarthria syndrome, depending on the affected white matter tracts.5
Stroke associated with large vessel disease
Stroke associated with large vessel disease is typically associated with atheroma of the extracranial vessels, such as the proximal internal carotid artery, carotid bulb or aortic arch, but also include arterial dissection. Carotid Doppler ultrasound examination can visualise the carotid bulb and proximal internal carotid artery and detect any atheroma causing haemodynamically significant stenosis, regarded as a stenosis greater than 70% of the arterial lumen. Ultrasound examination can also provide information on plaque morphology.
CT angiography is an alternative imaging technique and is incorporated into acute stroke assessments in emergency departments. CT angiography has the additional benefits of visualising the intracranial vessels and can therefore identify large vessel occlusions. However, it carries risks associated with radiation and contrast exposure.
Risk factors and stroke prevention
The major modifiable risk factors for developing stroke include physical inactivity, poor diet and nutrition, hypertension, obesity, diabetes mellitus, smoking, dyslipidaemia and AF. Lifestyle modification is a key component of both primary and secondary prevention of stroke, as is antihypertensive therapy for patients with hypertension, and anticoagulation for patients with AF. Other mainstays of secondary prevention include statins and antiplatelet agents (in the absence of AF).
Physical inactivity
A sedentary lifestyle is associated with adverse health effects, including increased mortality, cardiovascular morbidity and elevated risk of stroke. Studies have shown that physically active men and women have a 25 to 30% reduction in stroke compared with the least active individuals.6,7
There is no ceiling effect on the health gains of physical activity; the more active a person is, the better the health outcomes. However, the greatest benefits are reached within 2.5 to 5 hours of moderate intensity cardiac exercise per week plus two hours of strengthening exercise. Moderate intensity activity includes walking at a speed of at least 6.5 km per hour, playing a doubles tennis match or pushing a lawn mower without a propulsion system. As a rule of thumb, if you can have a normal conversation while exercising then you are not reaching the level of moderate intensity.
Diet and nutrition
A large and diverse body of evidence implicates several aspects of diet, including sodium intake, in the pathogenesis of hypertension, which itself is a major modifiable risk factor for ischaemic stroke. The American Heart Association (AHA) concludes that several aspects of diet can lead to elevated blood pressure.8 Dietary risk factors associated with elevated blood pressure are multifaceted.
Fruit and vegetable intake
A meta-analysis found a strong inverse relationship between the number of daily servings of fruit and vegetables and subsequent stroke.9 Analysis of the Nurses’ Health Study and the Health Professionals Follow-Up Study reported a reduction in relative risk of participants in the highest quintile for fruit and vegetable intake compared with those in the lowest quintile.10 Analysis of the Nurses’ Health Study reported that increased intake of flavonoids, found in citrus fruits, was associated with a reduced risk of ischaemic stroke.11
Mediterranean diet
A randomised, controlled trial of the Mediterranean diet in 7447 individuals at high cardiovascular risk showed that those eating an energy-unrestricted Mediterranean diet supplemented by nuts (walnuts, hazelnuts and almonds) and olive oil had a lower risk of stroke compared with control participants.12
Sodium and potassium intake
Meta-analyses have shown an association between sodium intake and stroke risk, presumably mediated through an increase in blood pressure.13,14 Potassium supplementation reduces stroke risk.15-17 A small trial suggested that consuming potassium-enriched salt reduced mortality from cardiovascular disease.18
Red meat
A meta-analysis of prospective studies concluded that intake of fresh, processed and total red meat was associated with an increased risk of ischaemic stroke.19
Dietary recommendations
The AHA guidelines recommend a reduced intake of salt and increased intake of potassium. A diet rich in fruit, vegetables and low-fat dairy products is recommended to lower blood pressure. A Mediterranean diet supplemented with nuts may be considered in lowering risk of stroke.
Hypertension
In its seventh report, the US Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure defined hypertension as systolic blood pressure (SBP) greater than 140 mmHg and diastolic blood pressure (DBP) greater than 90 mmHg.20 Hypertension is the single greatest risk factor for stroke (ischaemic or haemorrhagic), and the relationship between blood pressure and stroke is graded and independent of other risk factors.21 The risk of hypertension increases with age, and consequently more than two-thirds of people aged over 65 years have hypertension.20
Compelling evidence from a meta-analysis of 23 randomised trials showed that antihypertensive drug treatment reduced the risk of stroke by 32% compared with controls.21 The benefit is not specific to a particular class of antihypertensive agents.21 However, atenolol has been associated with greater variability in systolic blood pressure, which limits the efficacy of secondary prevention.22 For this reason, we recommend avoiding beta blockers for single-agent treatment of hypertension.
A meta-analysis shows that more intensive control of blood pressure (target SBP less than 130 mmHg) reduces the risk of stroke more than less intensive control (SBP 130 to 139 mmHg).23 The ACCORD trial, which recruited patients with diabetes at high cardiovascular risk, suggested that more intensive blood pressure control (target SBP less than 120 mmHg) conferred additional reduction in risk of stroke, which was a pre-specified secondary outcome.24 However, it is worth noting that the ACCORD trial was terminated early because of increased mortality observed in the treatment arm.
The AHA guidelines recommend regular blood pressure screening and appropriate treatment of hypertension, including lifestyle modification and pharmacological therapy. If patients develop pre-hypertension (SBP 120 to 139 mmHg or DBP 80 to 90 mmHg) then lifestyle modification is appropriate. However, patients with hypertension should be prescribed treatment to achieve a blood pressure below 140/90 mmHg. ACE inhibitors have recently been linked with an increased risk of lung cancer, causing concerns especially in former smokers.25 Otherwise, the choice of agent is influenced by patient characteristics and medication tolerance.
Obesity
Obesity is associated with increased stroke risk as well as hypertension and diabetes mellitus. Obesity is defined as a body mass index (BMI) greater than 30 kg/m2. Abdominal obesity is defined as a waist circumference greater than 102 cm in men and greater than 88 cm in women.26 Abdominal obesity can also be assessed with the waist-hip ratio. For every 0.01 unit increase in waist-hip ratio, there is a 5% increase in risk of cardiovascular disease.27
Abdominal body fat has proven to be a stronger predictor of stroke risk than BMI.28,29 Mounting evidence shows a graded positive relationship between stroke and obesity independent of other cardiovascular risk factors. Prospective studies of the relationship between adiposity and stroke showed a 40% increase in stroke mortality with each 5 kg/m2 increase.30 A meta-analysis that included more than 2.2 million participants found an increased relative risk of ischaemic stroke of 1.2 for overweight people, increasing to 1.24 for those with obesity.31
The effects of weight reduction on stroke risk have not been studied extensively. A study that followed up 4000 patients over 10 to 20 years compared those who achieved weight loss through surgery versus those who received usual care. It found a significant reduction in diabetes, myocardial infarction and stroke in the weight-loss surgery group.32
Diabetes mellitus
People with diabetes mellitus have an increased susceptibility to atherosclerosis and increased prevalence of atherogenic risk factors, notably hypertension and dyslipidaemia. Diabetes is an independent risk factor for stroke.33 Diabetes doubles the risk of stroke and about 20% of patients with diabetes die of stroke. There is a stepwise increase in stroke risk in patients with either impaired glucose tolerance or diabetes compared with individuals who are normoglycaemic.34
Stroke risk can be reduced in patients with diabetes mellitus. The Steno-2 study showed that patients with type 2 diabetes and microalbuminuria benefit from intensive therapy consisting of behavioural risk-factor modification, use of a statin, ACE inhibitor or angiotensin-receptor blocker and an antiplatelet drug.35 The risk of cardiovascular events was reduced by 60% with intensive therapy; there was also a reduction in stroke rates.
Despite this, there is no convincing evidence that intensive glycaemic control alone reduces individual stroke risk. A meta-analysis that included nearly 60,000 patients did not show a significant reduction in stroke risk with intensive glycaemic control.36
In patients with type 1 or type 2 diabetes, the AHA recommends controlling blood pressure to a target of 130/80 mmHg. The AHA also recommends considering treating adults with diabetes mellitus with a statin.37
Smoking
Cigarette smoking is a potent risk factor for ischaemic stroke, and there appears to be a dose-dependent response.38 A meta-analysis of 32 studies estimated that the relative risk (RR) for ischaemic stroke is 1.9 for smokers compared with nonsmokers.39 Epidemiological studies have not found a dose-response relationship, meaning complete cessation is required to reduce stroke risk.40
Counselling in combination with drug therapy using nicotine replacement, bupropion or varenicline should be offered to active smokers to help them quit smoking.
Dyslipidaemia
Most studies have found that a high total cholesterol level is a risk factor for ischaemic stroke. The Multiple Risk Factor Intervention Trial (MRFIT) of 350,000 men showed an increase in RR of death from ischaemic stroke associated with increasing cholesterol level.41 The Women’s Pooling Project and the Women’s Health Study both found a direct relationship between cholesterol level and ischaemic stroke.42,43
Statin therapy
Treatment with statins (inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A [HMG-CoA] reductase) reduces risk of stroke in patients with or at high risk of atherosclerosis.44,45 A meta-analysis that included over 90,000 patients showed that statins reduced the risk of all strokes by about 21%.45 Another meta-analysis found that each 1 mmol/L reduction in LDL-cholesterol level was associated with a 21.1% reduction in stroke.46 A recent multicentre study showed an additional benefit in stroke risk reduction with aggressive lipid lowering to a target LDL-cholesterol level of 1.8 mmol/L.47
Adverse effects of statins
The safety of statins merits discussion with patients, as long-term adherence to statin therapy is not optimal.48,49 There is a public perception that statins are poorly tolerated, with a high risk of muscle pain, which may be partly due to negative media coverage.50 Healthcare professionals also seem to overestimate the risk of side effects of statins, as indicated in a multinational survey of statin prescribers, who estimated that 6% of their patients were statin intolerant, largely because of myalgia.51 Interestingly, in randomised clinical trials, where participants were blinded to treatment, the incidence of muscle symptoms without an elevated creatine kinase (CK) level was less than 1%, and of muscle symptoms with a raised CK level was even less (0.1%).52 Most importantly, there was no significant difference in prevalence of symptoms between the treatment groups.52 This suggests that muscle symptoms in the community may be due to a ‘nocebo’ (negative placebo) effect rather than the pharmacological effect of the drug.
Statins can be associated with myopathy with elevated CK levels. However, in patients with myopathy it is important to consider other causes rather than to assume the statin is responsible. For example, statin-associated myopathy with elevated CK levels may also be precipitated by drug interactions (see Box 4). If the CK level is more than 10 times the upper limit of normal then the statin should be stopped immediately. Immune-mediated necrotising myopathy is rare, with an estimated incidence of 2 to 3 patients per 100,000 treated with statins, and is partially reversible with statin discontinuation.53
It is important for GPs to reassure patients who develop muscle symptoms without elevated CK levels that it may be coincidental and to encourage them to continue statin therapy.
Atrial fibrillation
AF is associated with a four- to five-fold increase in stroke caused by stasis-induced thrombi in the left atrial appendage, even in the absence of cardiac valvular disease. The diagnosis of AF is an important opportunity for primary prevention because this dysrhythmia is often diagnosed before stroke in many patients.
CHA2DS2-VASc score and stroke risk
After the diagnosis of AF has been established, an estimate of the individual’s risk of stroke can be calculated using the CHA₂DS2-VASc score. This score assigns:
- one point each for congestive heart failure (C) and hypertension (H)
- two points for age 75 years and over (A₂)
- one point for diabetes mellitus (D)
- two points for prior stroke or TIA (S₂)
- one point each for vascular disease (V), age 65 to 74 years (A) and female sex (Sc).54
A score of 0 corresponds to a stroke risk of 0.5 to 1.7% per year, one point to a moderate risk (1.2 to 2.2% per year) and two or more to a high risk (1.9 to 7.6% per year).
Anticoagulation
Anticoagulation is indicated if a patient has at least one risk factor (other than female sex), unless there is a strong contraindication to anticoagulation.55 Anticoagulation can be achieved using warfarin or a nonvitamin K oral anticoagulant (NOAC; also known as a direct oral anticoagulant [DOAC]). NOACs licensed in Australia include dabigatran, apixaban and rivaroxaban.
NOACS are preferred over warfarin as they do not necessitate routine INR checks and have fewer drug interactions and a lower risk of intracerebral haemorrhage than warfarin. However, all NOACs are excreted by the kidneys and are contraindicated in patients with advanced renal disease. NOACs are not licensed for treating patients with valvular AF, which currently refers to those with moderate to severe mitral stenosis or mechanical heart valves.56
Cardiac occluder devices
Cardiac occluder devices can be considered for patients with AF who cannot tolerate long-term anticoagulation or have a high risk of complications of anticoagulation.57 These devices reduce the risk of embolus formation by occluding the left atrial appendage. Pooled data from the PROTECT AF and PREVAIL studies suggests that the WATCHMAN occluder device has similar efficacy to warfarin at five years, with an additional reduction in bleeding complications and mortality.58
Other secondary prevention strategies for stroke
Antiplatelet therapy
Antiplatelet therapy is indicated for all patients with ischaemic stroke or TIA who do not have AF when brain imaging has excluded haemorrhage. Aspirin and clopidogrel are both licensed for secondary prevention of stroke and TIA in Australia.
A meta-analysis of three trials concluded that short-term dual antiplatelet therapy with 100 mg aspirin and 75 mg clopidogrel confers an additional 30% reduction in stroke recurrence in high-risk patients with TIAs or minor strokes compared with monotherapy.59 This benefit is apparent within the first three to 12 weeks of use. However, prolonged dual antiplatelet therapy is associated with increased bleeding complications.60 Therefore, it should not be continued beyond three months in the absence of another indication.
Some practitioners recommend three weeks of dual antiplatelet therapy for most high-risk patients with TIAs.
Closure of patent foramen ovale
There is evidence that closure of a patent foramen ovale reduces recurrent stroke risk in young patients with cryptogenic stroke. The benefit is evident if they have embolic strokes, large right-to-left shunts or an atrial septal aneurysm.61 The benefit is reduced if the patent foramen ovale is small or there is a coexisting indication for long-term anticoagulation. The procedure is associated with an increased risk of new-onset AF (pooled RR, 4.33; 95% CI, 2.37 to 7.89), but most cases are thought to be transient.62
Carotid endarterectomy
Carotid endarterectomy should be considered in patients with stroke or TIA who are found to have a severe ipsilateral carotid stenosis. Data from the landmark North American and European trials proved the effectiveness of endarterectomy in patients with severe stenosis, defined as 70 to 99% compared with medical treatment.63,64 The magnitude of the benefit of endarterectomy for symptomatic patients with 50 to 69% stenosis remains uncertain.65
Complications in stroke survivors
Poststroke depression
Depression affects one-third of stroke survivors at any one time after stroke, with the highest risk in the first year.66 The pathophysiology is thought to be multifactorial, including inflammation, alteration in neurotrophic factors and changes in neurotransmitter levels. The strongest predictors of poststroke depression include physical disability, stroke severity, pre-existing depression and pre-existing cognitive impairment.67-69
Poststroke depression is associated with poor functional outcomes, reduced quality of life, higher rates of health care use and higher mortality rates.70-73 There are no randomised trials that have shown that antidepressants improve poststroke depression; however, a meta-analysis suggested benefit.74
Sexual dysfunction
Poststroke sexual dysfunction is often overlooked. Libido may be reduced by poststroke depression, fatigue, medications and concerns over body image (e.g. facial weakness). The Stroke Foundation provides information that may be useful for patients. Psychological assessment and support may be required.
Poststroke fatigue
There are several definitions of poststroke fatigue. A definition borrowed from publications on multiple sclerosis describes fatigue as ‘a subjective lack of physical and/or mental energy perceived by individual or caregiver to interfere with usual or desired activities’.75 A systematic review estimated the incidence of poststroke fatigue defined in this way as ranging from 23 to 34% after minor stroke or TIA.
Poststroke fatigue is associated with decreased participation in physical activities and reduced quality of life.76,77 Important risk factors for poststroke fatigue include physical impairment and comorbid conditions such as congestive cardiac failure and obstructive sleep apnoea.78,79 Medications such as sedatives, antidepressants and hypnotics can also contribute to poststroke fatigue.
Management of fatigue is directed at identifying comorbid conditions and rationalising medications, as well as involving physiotherapists and occupational therapists. A graded exercise program may help decrease poststroke fatigue.80
Driving restrictions
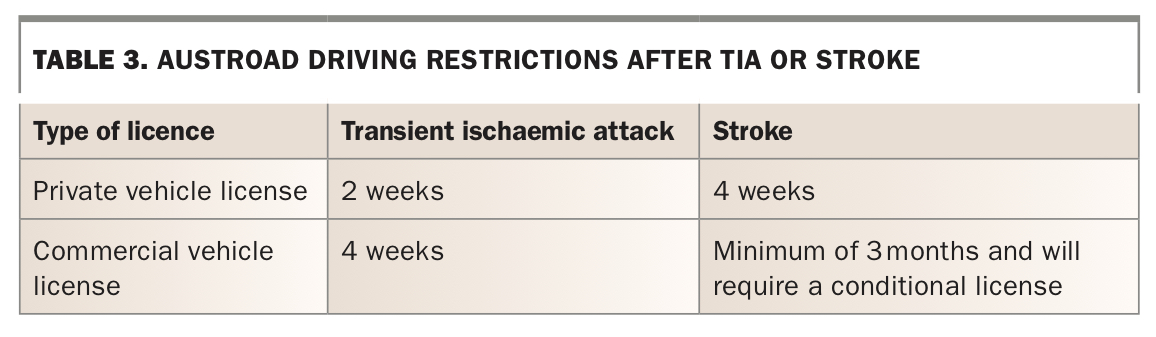
The Roads and Maritime Services guidelines on driving restrictions after stroke or TIA are summarised in Table 3. The duration of driving restrictions may be extended indefinitely if there is persisting disability that impairs the ability to drive. A fitness to drive assessment may be required to determine a person’s suitability to drive, particularly if there are cognitive deficits that are difficult to appreciate in the consulting office.
{kind=link}
Conclusion
Stroke is a leading cause of disability in Australia. There are several well-characterised modifiable risk factors, including hypertension, dyslipidaemia, diabetes, AF and smoking. GPs can identify these conditions and initiate and monitor appropriate evidence-based treatment with resulting benefits for both individuals and the community. GPs can also help mitigate the morbidity associated with stroke through timely recognition and management of stroke sequelae, such as poststroke depression, sexual dysfunction and fatigue. MT
COVID-19 and stroke
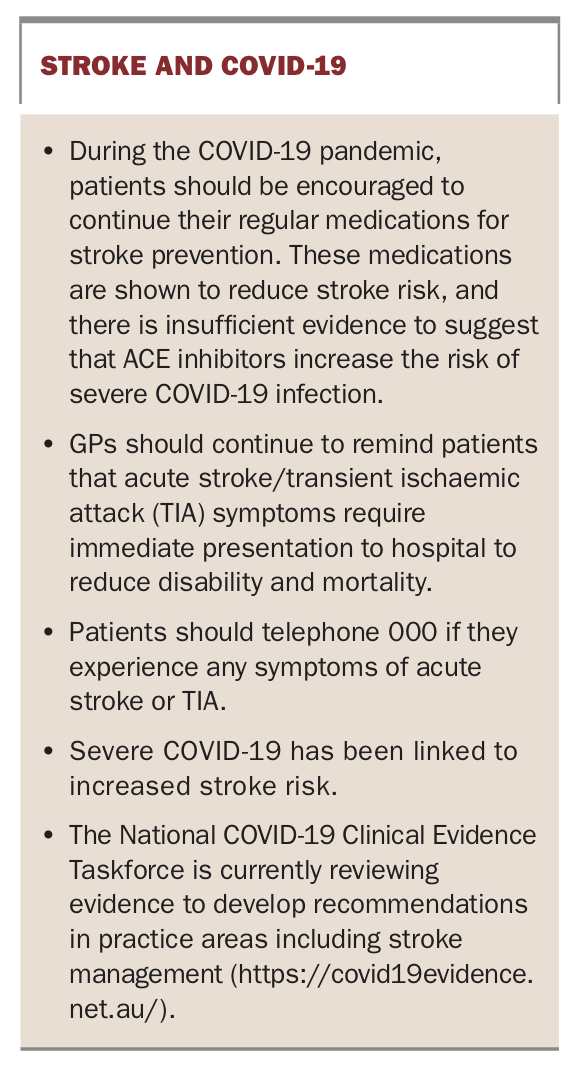
Advice from the authors of this article on managing patients with stroke during the COVID-19 pandemic is provided in the Box.
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.