Ischaemic stroke in younger people: recognition and management

Dr Vuong is a Neurology Registrar at Monash Health, Melbourne. Professor Ma is Director of Neurology at Monash Health, Melbourne.
Professor Phan is Head of Neuroscience Research, Monash Health, Melbourne, Vic.
Stroke
Transient ischaemic attack

Up to a quarter of strokes occur in people under the age of 55 years, caused by either traditional cardiovascular risk factors or rarer conditions, including arterial dissection and illicit drug use. Despite young age, anyone with symptoms consistent with an acute stroke should be referred to the nearest emergency department with a stroke service. Long-term follow up of survivors is needed to ensure secondary stroke prevention.
- The incidence of stroke is rising in both younger and older patients.
- Traditional risk factors usually associated with strokes in older patients are also significant in the younger population.
- Stroke should be suspected in any patients with sudden onset of focal neurological signs, regardless of age.
- Patients suspected of having a stroke should be referred to hospitals that provide thrombolys is or clot retrieval therapy.
- Specialist consultation with a stroke neurologist is recommended for all patients with stroke.
- Long-term secondary stroke prevention is necessary to prevent recurrence.
Stroke is a significant contributor to mortality and morbidity in Australia, affecting 1.3% of the total population and ranking third in the annual leading cause of all deaths.1 Most (87%) strokes are ischaemic, caused by a clot obstructing an arterial vessel. Although stroke is traditionally thought of as a disease of older age, its incidence in younger people is increasing, with a wide range of possible underlying risk factors and aetiologies. Up to 25% of all strokes occur in younger adults, defined as people under the age of 55 years.2-4 Studies have shown up to a 42% increase in the incidence of strokes in the 18 to 54 years age group between the years 2003 and 2012 in the USA, with significant long-term implications for patients and their carers because of the higher disability-adjusted life years.5 It is of paramount importance to recognise and reduce the risk of stroke in younger patients.
This article discusses the causes and prevention of ischaemic stroke in younger people. It also provides an overview of acute stroke management and secondary prevention.
Acute management of stroke
Transient ischaemic attack versus ischaemic stroke
Transient ischaemic attack (TIA) and ischaemic stroke should be regarded as a continuum. Both involve obstruction of an arterial vessel supplying the brain, usually in the form of a blood clot. If the clot causing disability dissolves in a timely manner without resultant damage to brain tissue then the outcome is TIA. If not, the outcome is ischaemic stroke. Symptoms of a TIA last minutes, not 24 hours as previously written in textbooks, and a TIA cannot be diagnosed without brain imaging.
Patients who present with TIA and minor ischaemic strokes require urgent evaluation and commencement of antithrombotic therapy as recurrence is high within the first week if left untreated.6 Further, half of recurrences occur within 48 hours. Many hospitals have established TIA clinics to handle outpatient management of these patients.7
Acute stroke therapy
The treatment of acute ischaemic stroke changed significantly in 2015, when multiple randomised clinical trials showed evidence supporting thrombectomy.8 ‘Clot-busting’ drugs (alteplase and tenecteplase) are used when there are regions of salvageable brain tissue, whereas clot retrieval is used when a clot is lodged within a large vessel such as the internal carotid artery, middle cerebral artery or basilar artery. These treatments are time critical, and patients with focal neurological deficits (such as unilateral face, arm, speech or visual deficits) should be directed to call an ambulance for urgent assessment at a hospital.
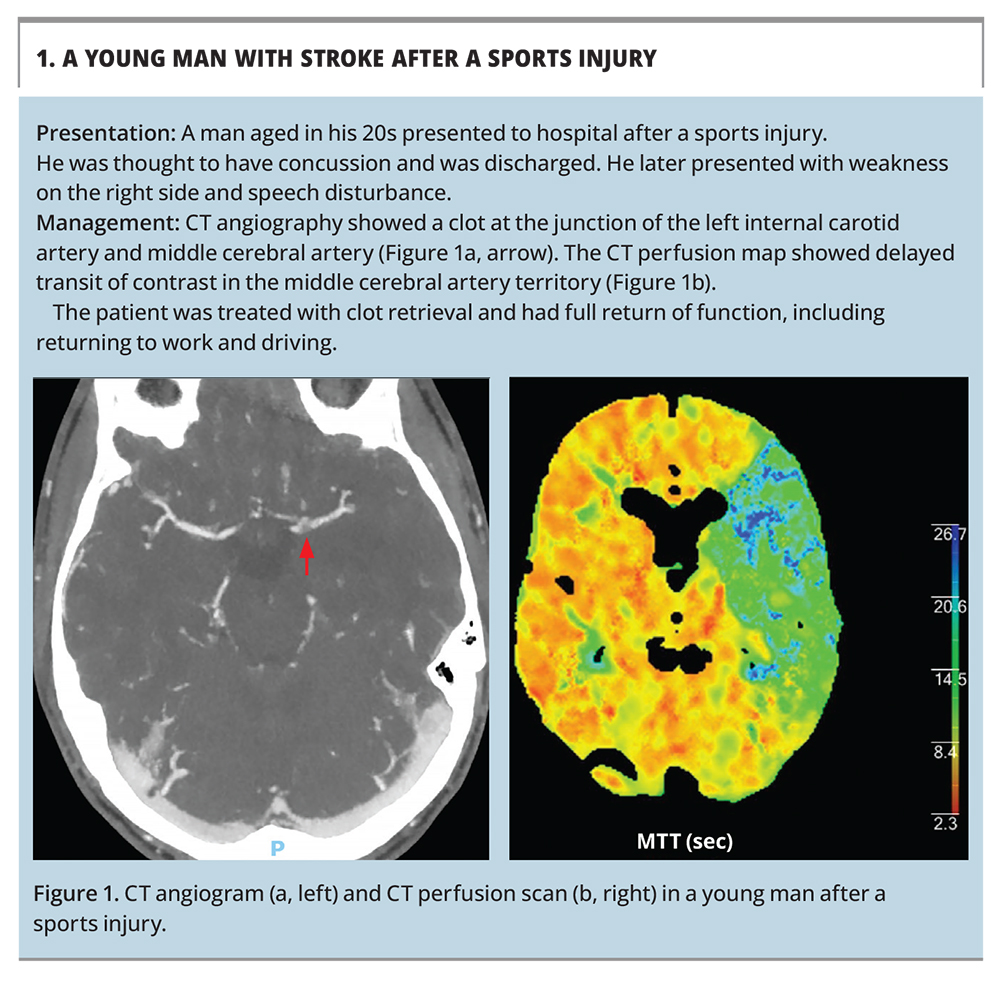
Because of the resources required to provide comprehensive stroke services (urgent brain imaging, urgent evaluation by an acute stroke team and stroke unit care), hospitals that provide these are likely to be teaching (public) hospitals in metropolitan cities. Ambulance officers are aware of these hospitals, and patients meeting stroke identification criteria are directed to these (Box 1 and Figure 1). Selected rural hospitals are connected to the major hospitals, providing clot retrieval by a telehealth service.9
{kind=link}
Stroke prevention in younger people
Modifiable risk factors
An important aspect of management of younger stroke patients is preventive therapy. Here, we discuss the approach to modification of traditional risk factors for ischaemic stroke as well as rarer causes of stroke that are more likely in a younger population.
Acute ischaemic stroke in older people has been recognised as the culmination of cardiovascular risk factors, such as hypertension, hyperlipidaemia, diabetes mellitus, tobacco smoking, obesity and alcohol use, physical inactivity and poor diet.5,10 The prevalence of metabolic syndrome and the subsequent development of cardiovascular risk factors are increasing in younger people. Several studies have provided evidence that these factors correlate with an increased susceptibility to ischaemic stroke overall and also stroke from other causes in these younger patients. In younger patients with stroke, studies show high rates of hypertension (35%), hyperlipidaemia (50 to 60%), type 2 diabetes (10%) and obesity (40%).11-14 Obesity is a prominent independent risk factor for stroke.15 Treatment of cardiovascular risk factors is important for primary prevention of stroke in younger people (aged less than 55 years), as well as addressing lifestyle risk factors.
Other modifiable lifestyle risk factors for stroke include use of illicit drugs, including psychostimulants such as amphetamines and cocaine, and depressants such as heroin, and heavy or heavy episodic alcohol consumption. Compared with the general population, younger patients with stroke are more likely to have a history of tobacco smoking.5 The relative risk of stroke associated with smoking has been estimated at 2.9 for those under 55 years of age.16
Specific risk factors in women
Hypertensive disorders of pregnancy can cause ischaemic or haemorrhagic stroke in the antepartum and postpartum periods. This modifiable risk factor is best managed in conjunction with the obstetrics unit. Other rare causes of peripartum and postpartum strokes are discussed below.
Secondary stroke prevention
An important issue with secondary stroke prevention in younger people is medication adherence. It is important to follow up patients long term as risk-modifying medications need to be continued lifelong.
Antiplatelet therapy
Randomised trials of dual antiplatelet therapy with aspirin and clopidogrel (DAPT) versus aspirin alone in high-risk patients after a TIA or minor ischaemic stroke showed a reduction in stroke recurrence at 90 days among those assigned to DAPT.17 A caveat is that these patients were recruited within 24 hours of stroke onset. As such, patients with a TIA or minor stroke should be referred to hospital for urgent evaluation, although not necessarily admission. DAPT is recommended for 21 days, followed by monotherapy with aspirin if the patient is aspirin-naïve or clopidogrel if the patient was previously taking aspirin.17 Long-term DAPT is associated with an increased risk of bleeding that outweighs the benefit of secondary stroke prevention.
The role of combination aspirin and ticagrelor in secondary stroke prevention is not clear. A recent randomised trial showed a small reduction in stroke-related mortality at 30 days with aspirin and ticagrelor versus aspirin alone, but no difference in morbidity, and the combination was associated with significantly increased bleeding.18
Anticoagulation
Atrial fibrillation (AF) is less common in younger than older patients. However, younger adults with AF should be commenced on anticoagulation. Many randomised trials have shown the benefit of warfarin and newer direct oral anticoagulants (DOACs) for primary and secondary prevention of stroke in the setting of AF.19-22
Hypertension management
Long-term blood pressure management reduces the risk of recurrent TIA or ischaemic stroke. In general, a normotensive target (less than 140/90 mmHg) should be achieved, and the standard first-, second- and third-line antihypertensive therapies are recommended.23 The role of primary aldosteronism as a cause of hypertension and stroke is currently being evaluated.
Cholesterol-lowering therapy
A high-dose statin provides additional benefit to antiplatelet therapy in secondary stroke prevention. Current guidelines recommend a low-density lipoprotein (LDL) cholesterol target of less than 1.8 mmol/L for secondary stroke prevention to reduce the risk of major cardiovascular events, including stroke recurrence.24 This may be achieved by combining high-dose atorvastatin with ezetimibe, with alternatives including fenofibrate.
Carotid endarterectomy
Patients with an ischaemic stroke ipsilateral (on the same side) to a high-grade carotid stenosis (defined as 70 to 99% using North American Symptomatic Carotid Endarterectomy Trial [NASCET] criteria) requires prompt specialist management for consideration of carotid endarterectomy (CEA).25 The benefit of CEA is greatest if it is performed within the first two weeks after stroke onset and decreases if it is performed over the ensuing three months. By contrast, the risk of complications is highest if CEA is performed within 48 hours of stroke onset. The decision to proceed with CEA or insertion of a carotid artery stent is complex and requires consensus between the stroke unit and vascular surgeon, balanced by the patient’s comorbidities and vascular anatomy, and the complication rates of the unit performing the procedure. Patients with significant comorbidities or active coronary artery disease may not benefit from such intervention.
Patients without stroke or with a stroke in the contralateral hemisphere to a carotid artery stenosis are deemed to have asymptomatic carotid artery disease. These patients have an annual risk of stroke of about 1% with either surgery or best medical therapy. As such, routine CEA has no added benefit for patients with asymptomatic carotid artery disease. Attention should be paid to optimising medical therapy and lifestyle modifications.
Specific stroke aetiologies and management
Arterial dissection
Dissection or tear within an arterial vessel wall is a common cause of stroke in younger people, with registry studies suggesting it accounts for up to 15% of stroke cases in this age group.26 Although neck trauma is a known cause of arterial dissection, a history of trauma may not be present. Patients who present with stroke-like symptoms with a history of recent neck manipulation or neck pain should be evaluated for a dissection. However, spontaneous dissection also occurs.
Diagnosis of arterial dissection requires CT initially, followed usually by MR angiography with specific MR sequences to detect abnormalities in the vessel wall. Routine MR brain studies do not target this area and can miss this common diagnosis. Patients with arterial dissection are treated with antiplatelet therapy; surgery is not recommended, and management at a tertiary stroke service is usually required.
Fibromuscular dysplasia (FMD) is a noninflammatory, nonatherosclerotic vascular disease of small to medium-sized arteries. Controversy remains as to whether isolated, asymptomatic FMD increases the risk of ischaemic stroke. Carotid web is a form of FMD with an abnormal shelf-like projection of intimal fibrous tissue into the carotid bulb. Early reports suggests that patients with a stroke secondary to a carotid web have an increased risk of stroke recurrence despite best optimal management (five of 30 patients).27 Further clinical trials are required to determine the best form of stroke preventive therapy in this small subset of patients.
Genetic causes
Genetic causes of stroke account for a small proportion of stroke presentations in younger people. Fabry disease is a rare X-linked inherited lysosomal storage disorder caused by a mutation in the alpha-galactosidase A gene. Recent studies of young patients with cryptogenic strokes have shown that Fabry disease accounts for about 1% of this cohort.28 Patients with this disease tend to have affected family members and other features, such as renal failure or neuropathy.
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a genetic disorder caused by a mutation in the NOTCH3 gene. Patients present with recurrent episodes of stroke, migraines, psychosocial changes and ultimately cognitive impairment.29
Mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes (MELAS) is a rare maternally inherited mitochondrial genetic disorder. Patients present with stroke-like episodes, often after a seizure, at a young age, with accompanying encephalopathy and early onset dementia. This condition can mimic stroke, but the imaging abnormalities differ; multiple vascular territories are usually involved, abnormalities are often bilateral and most commonly affect the parieto-occipital and parietotemporal lobes.
Patent foramen ovale
A patent foramen ovale has been considered a potential cause of stroke through paradoxical embolisation from the venous circulation. Patent foramen ovale can be diagnosed by a transthoracic echocardiogram with a bubble study. Intervention for patent foramen ovale is limited to selected patients; current guidelines recommend closure of a patent foramen ovale in patients under the age of 60 years with cryptogenic stroke and a paradoxical right-to-left shunt. A complete workup for other stroke aetiologies, such as large artery disease and cardioembolic mechanisms, is also a required.
Post-hoc analysis of a recent trial showed that patients with cryptogenic stroke and a patent foramen ovale assigned to rivaroxaban had better outcomes than those assigned to aspirin. Closure of a patent foramen ovale carries a 6% risk of AF. There is no role for prophylactic closure of patent foramen ovale in patients without strokes or for management of patients with migraine.
Vasculitis, vasculopathy and reversible cerebral vasoconstriction syndrome
Primary angiitis of the central nervous system (PACNS) is often described in textbooks as an unusual cause of ischaemic stroke. However, the unintended consequence is that screening for PACNS is frequent; this search is rarely fruitful. A common trigger is an imaging report of beading of the cerebral vessels on CT or MR angiography; however, this has many possible causes (see below). The diagnosis of PACNS requires a brain biopsy. A 10-year retrospective analysis of over 7000 patients presenting to a tertiary stroke centre in Australia identified one patient (0.02%) with definite central nervous system angiitis.30
Temporal (giant cell) arteritis is another possible cause of stroke in the older age group. However, in our experience, stroke is not a first presentation of this condition. More often, patients are diagnosed with temporal arteritis because of constitutional symptoms, fatigue, jaw claudication and vision problems. Stroke can occur later during the course of this disease rather than as presenting symptom.
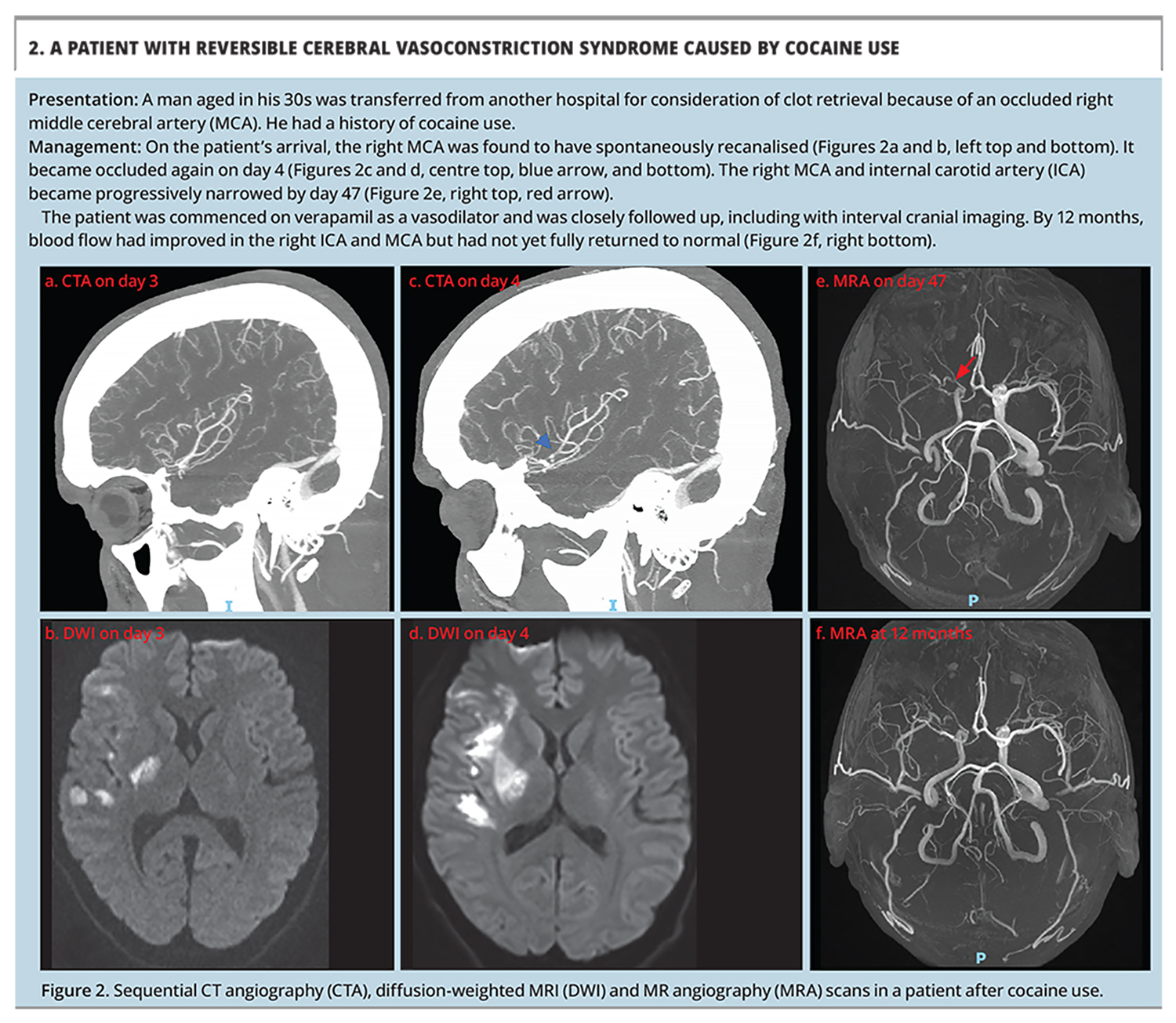
Reversible cerebral vasoconstriction syndrome (RCVS) is caused by multifocal vasoconstriction of intracranial arteries, leading to the appearance of beading or stenosis on CT or MR angiography, which resolves spontaneously (Box 2 and Figure 2). These scans have been mislabelled as vasculitis in the past. In younger patients with stroke, RCVS is most commonly seen after use of vasoactive substances, including cannabis, and in patients with hypertensive disorders of pregnancy.31 Acute treatment comprises vasodilative pharmacotherapy with nimodipine or verapamil. Long-term management comprises avoidance of triggers to prevent recurrence. Corticosteroids are not recommended to treat patients with RCVS.
{kind=link}
Viral infection, particularly with varicella zoster virus (VZV), can be associated with vasculopathy resulting in stroke. This can occur in the acute phase in children or the late phase in young adults.32 These patients are best evaluated in hospital or a specialist clinic, as investigations including lumbar puncture are often required to confirm the diagnosis.
Since the COVID-19 pandemic began, a frequent question has been whether infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) can cause stroke. Our experience and that around the world is that patients with stroke after COVID-19 also have traditional risk factors. A survey in 54 centres in North America found a COVID-19 prevalence of 1.3% among 8163 patients presenting with stroke.33
Pregnancy-associated stroke
Among pregnant patients with stroke, ischaemic stroke accounted for 43% of cases (down from 87% among other patients with stroke), intracranial haemorrhage for 42% (increased from 12%) and cerebral venous sinus thrombosis for 17% (increased from less than 1%).31 Hypertensive disorder of pregnancy was present in 17%, 38% and 12% of women with ischaemic stroke, haemorrhagic stroke and cerebral venous sinus thrombosis, respectively.31
Cerebral venous sinus thrombosis
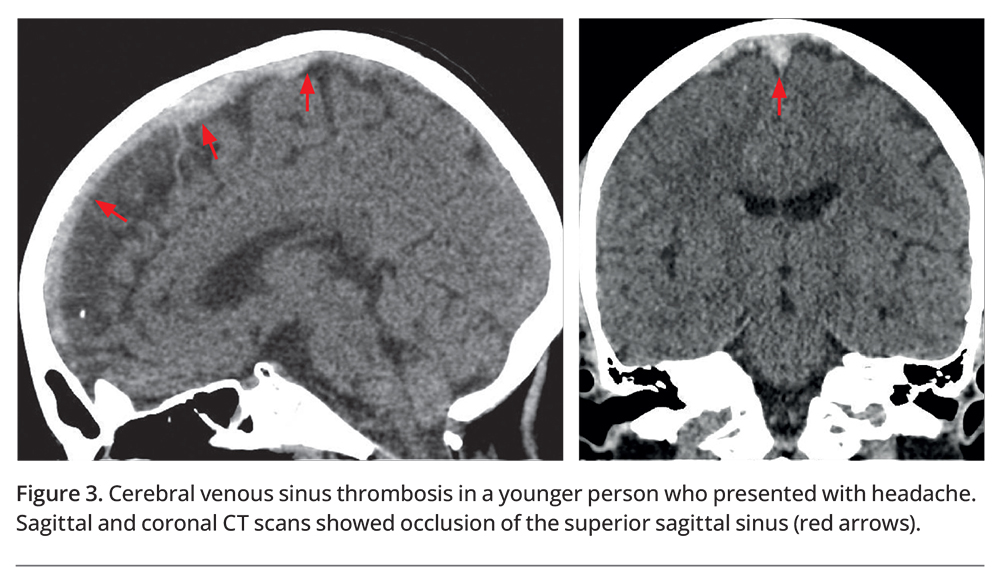
Cerebral venous sinus thrombosis (CVST) is an uncommon but important diagnosis to consider in young patients and particularly during pregnancy. In rare cases, CVST has also been linked with COVID-19 vaccination. CVST involves thrombus within the venous sinus thrombosis with subsequent venous infarction or haemorrhage caused by raised back pressure (Figure 3). The presentation of CVST is variable; however, most patients have a combination of a headache plus focal neurological deficits and seizures.
{kind=link}
Conclusion
Younger patients can have strokes, caused by either traditional risk factors or rarer conditions. Despite young age, anyone who presents with symptoms consistent with an acute stroke should be referred to the nearest emergency department with a stroke service to determine if they are eligible for hyperacute stroke therapies. After a stroke, patients need close follow up to ensure adherence with medications for stroke prevention, which should be continued lifelong. MT
COMPETING INTERESTS: Professor Phan has received honoraria for lectures from Genzyme, Bayer, BMS, Pfizer and Boehringer Ingelheim. Dr Vuong, Professor Ma: None.