Constipation in children

Constipation
Children's health
Constipation in children is usually functional, but it is important to seek red flags and rule out any underlying medical condition. Management of functional constipation includes encouraging a healthy diet and toileting routine as well as medical therapy to disimpact and then help to maintain regular defaecation of soft stool.
Constipation is a common problem in children of all ages.1 Defined as a delay or difficulty in defaecation that is present for two weeks or longer, constipation can cause significant distress to the child and their family.1 Here we review the topic in the primary care setting.
Remember
- Most children with constipation have functional constipation, where no underlying medical condition is identifiable.
- The Rome criteria for the diagnosis of functional constipation can be a useful guide in establishing the diagnosis.2
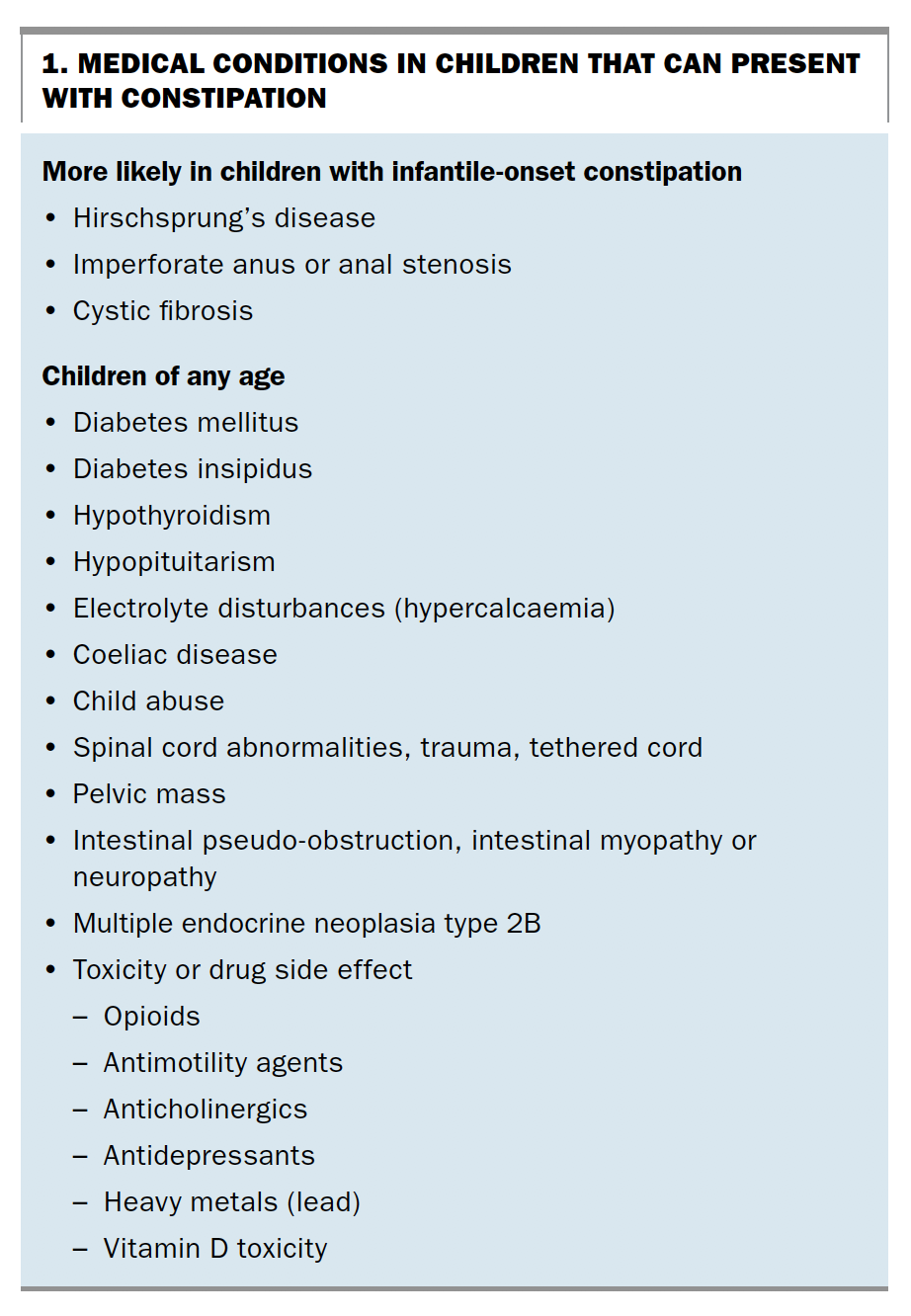
- It is important to rule out other medical conditions that can present with constipation (Box 1).
- In exclusively breastfed babies, infrequent defaecation up to once in every 10 days is not unusual.
- Constipation commonly presents when solids are introduced, during toilet training and at the start of daycare or school.
{kind=link}
Assessment
History and examination
- Take a detailed history documenting stool frequency, consistency, size and any painful defaecation, soiling or rectal bleeding.
- Toilet training and psychosocial history are also important to identify stressors that may be contributing to functional constipation.
- Physical examination includes an abdominal examination and inspection of the perianal and sacrolumbar regions. Neurological examination should focus on the lower limbs and perineum to rule out spinal cord pathology.
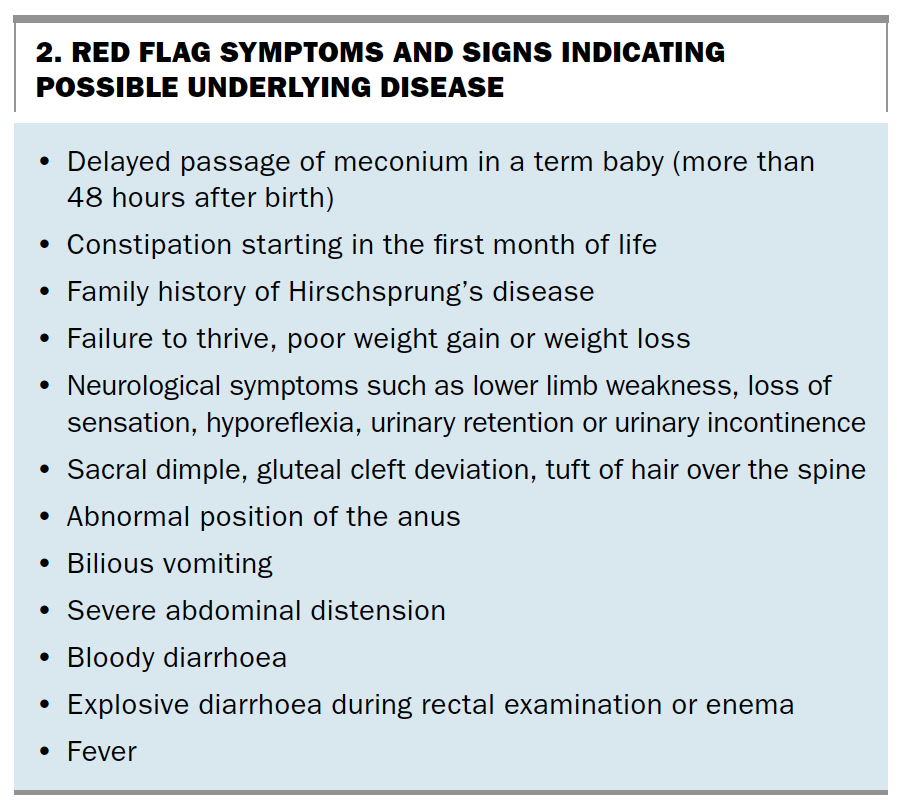
- Actively seek red flag signs and symptoms that could indicate underlying disease (Box 2).
{kind=link}
Digital rectal examination
- Most children with constipation can be diagnosed and managed without undergoing digital rectal examination, which is often traumatising for them.
- However, careful perianal inspection should not be omitted from the assessment.3
Abdominal x-ray
- Abdominal x-ray is not routinely indicated for diagnosis and management of children with constipation.
- Most patients with constipation, including children, can be diagnosed through careful history taking and examination. Reducing unnecessary radiation exposure in children is especially important.3
- Abdominal x-ray may be useful when the history and examination are inconsistent with the clinical diagnosis.3
- Sacral agenesis can be detected on abdominal x-ray and may be useful in the diagnosis of Currarino syndrome. This rare autosomal dominant disorder is characterised by the triad of sacral vertebral defect, presacral mass and anorectal malformation. Patients with this syndrome have abnormal perianal examination findings.4
Management
Diet and behaviour modification
- Encourage the child to eat a normal healthy diet. There is no evidence that increased fibre intake is useful in the management of childhood constipation.3
- Introduce a toileting routine that capitalises on the gastrocolic reflex. Ask parents to encourage their child to sit on the toilet for five minutes after meals, without any distractions from technology or books.
- Ask parents to encourage their child to defaecate when they notice stool-withholding behaviour.
- Input from a psychologist may be helpful, especially in children with severe anxiety around defaecation.
Medical therapy
- The aim of medical therapy is to disimpact and then maintain regular defaecation of soft, easy-to-pass stools. This breaks the vicious cycle of painful defaecation that reinforces stool-withholding behaviour in children.
- Following disimpaction, the recommended approach is maintenance therapy with a stool softener for six months, after which the therapy can be slowly withdrawn.3 Polyethylene glycol is the recommended first-line treatment for childhood constipation.3,5
- Osmotic laxatives, such as lactulose and polyethylene glycol, and lubricant laxatives, such as liquid paraffin, are safe for prolonged use. The recommended dose in children is 1 to 2 mL/kg/day for lactulose and 0.2 to 0.8 g/kg/day for polyethylene glycol 3350.3
- Liquid paraffin is contraindicated in patients at risk of aspiration.
- Bulking agents can exacerbate constipation and are not recommended for children.
- Prolonged use of stimulant laxatives is discouraged because of a potential risk of colorectal cancer. There is also a risk of structural damage to the surface epithelial cells.6
- Enemas may be needed in children with severe faecal impaction. Avoid phosphate enemas because of the risk of electrolyte imbalance and renal failure. Microenemas containing sodium citrate, sodium lauryl sulfoacetate and sorbitol can be used in an outpatient setting.
Conclusion
Most children with constipation have functional constipation, which can be managed with a combination of education, diet and behaviour modifications, and medications. It is important to rule out other medical conditions that could be causing the constipation in the first instance, and red flag symptoms and signs should be actively investigated. There is a high risk of constipation recurring. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.