Insulin degludec plus insulin aspart: a combination insulin with ultra-long action

Diabetes type 1
Diabetes type 2
Insulin degludec is a modified human insulin with an ultra-long duration of action (more than 42 hours). The TGA recently approved a combination insulin containing insulin degludec plus insulin aspart for patients with type 1 or type 2 diabetes who require basal and prandial insulin, and it was PBS listed on 1 August 2018. What do GPs need to know about this insulin and its use in patients with diabetes?
Update
Shortly after this article went to print, insulin degludec/insulin apart 70/30 became available on the PBS. The online version and the full text PDF of this article (see link above) have been updated.
Individuals with long-term type 2 diabetes have progressive pancreatic beta-cell failure, and many will require insulin. Conventionally, insulin may be introduced as a once-daily basal insulin, prandial insulin analogues, premixed insulin (containing a fixed proportion of soluble rapid-acting insulin analogue and intermediate-acting insoluble protamine-bound insulin) or basal-bolus multiple daily injections. Both the initiation and intensification of glucose-lowering therapy, in particular insulin, is often delayed in patients with type 2 diabetes (described as clinical inertia).1 A number of barriers to injectable therapy have been identified, including inconvenience, needle burden and weight gain. However, above all the fear of hypoglycaemia associated with more intensive insulin therapy has an impact on both clinicians and patients and may limit the reduction in glycated haemoglobin (HbA1c) achieved.2,3
Currently available premixed insulins may enable greater improvement in HbA1c than basal insulin (insulin glargine) alone. However, they result in a higher risk of hypoglycaemia and weight gain and are relatively inflexible in dose timing and titration.1,4 The long-acting basal insulin analogues, insulin glargine and insulin detemir, cannot be combined with a fast-acting insulin analogue in the same syringe, and are therefore not suitable as premixed insulin. Therefore, currently available premixed insulin analogues contain either insulin lispro or insulin aspart as the fast-acting component, combined with protaminated insulin as the basal component. Protamine is added to protract the absorption of insulin monomers, but the duration of action of premixed insulin is less than that of insulin glargine, and its absorption and glucose-lowering effect are more variable.5,6
To address these deficiencies, a new insulin combination, insulin degludec/insulin aspart (IDegAsp) 70/30, has been developed that may facilitate earlier introduction of insulin and a more intensive titration regimen.
What is insulin degludec/insulin aspart?
IDegAsp 70/30 is a relatively new combination insulin that contains 70% insulin degludec, a modified human insulin with an ultra-long duration of action (in excess of 42 hours), along with 30% rapid-acting insulin aspart. Insulin degludec is not currently available in Australia as an individual drug.
Insulin degludec has a fatty diacid side chain that allows the formation of stable dihexamers and long multihexamers in the subcutaneous tissue after injection, from which monomers slowly dissociate. As well as an ultra-long duration of action and a half-life of more than 25 hours, this leads to reduced within-patient variability compared with insulin glargine U100.7,8 These pharmacokinetic characteristics are associated with clinically relevant reductions in HbA1c, fasting blood glucose levels and risk of hypoglycaemia.9-12
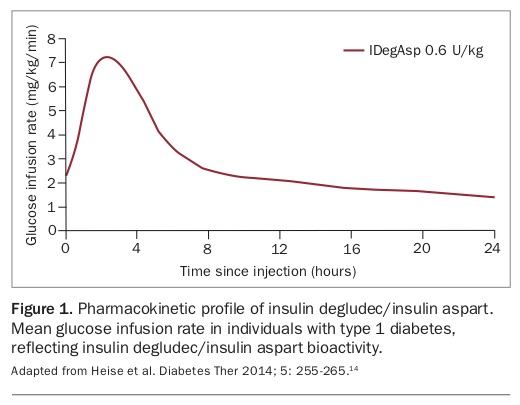
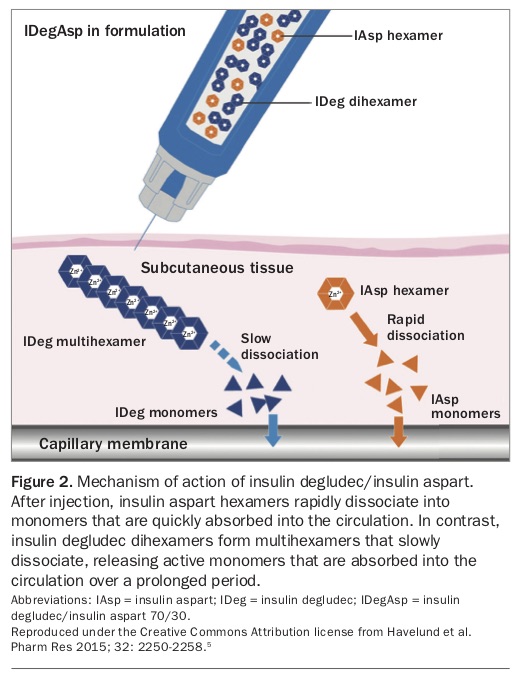
The combination of insulin degludec and insulin aspart in solution contains dihexamers of insulin degludec and hexamers of insulin aspart that do not interact, enabling each insulin to have a distinct pharmacokinetic profile and thus distinct prandial and basal glucose-lowering effects (Figure 1).13,14 These effects are more pronounced than with biphasic insulin aspart 30 (BiAsp 30).13 Following injection, the insulin degludec dihexamers form a subcutaneous depot of stable multihexamers, which slowly disassemble into active monomers, providing basal insulin coverage.15-17 Concurrently injected insulin aspart hexamers quickly dissociate into monomers that are rapidly absorbed to enable prandial glucose lowering (Figure 2).5
{kind=link}
{kind=link}
IDegAsp has a profile that is closer to physiological, allowing individuals to be more flexible with the time of insulin administration.18 The protracted absorption and action of insulin degludec lead to blood glucose levels with consistently lower variability compared with insulin glargine, which translate into a lower risk of hypoglycaemia.1,8 The onset of prandial glucose lowering is within 14 minutes.1 Furthermore, after dosage changes in IDegAsp, steady state is achieved after three days, with no further accumulation of insulin, reducing the possibility of insulin ‘stacking’ and subsequent hypoglycaemia.1
What is the evidence?
IDegAsp in type 2 diabetes
Several randomised controlled trials have compared IDegAsp 70/30 twice daily with BiAsp 30. These studies were designed to achieve the same HbA1c in both arms, an important consideration when comparing the two therapies, as insulin doses were not titrated to achieve a lower HbA1c in the IDegAsp treatment arm. These studies showed lower fasting glucose levels and significantly less hypoglycaemia, including nocturnal and severe hypoglycaemia, in the IDegAsp arm.19-21 These benefits were seen in both insulin-naïve and insulin-experienced patients, and in patients using insulin in conjunction with oral hypoglycaemic agents including metformin. The non-inferiority of HbA1c in patients receiving IDegAsp compared with BiAsp 30 was shown with a lower total insulin dose and less weight gain.20,22 Meta-analyses have confirmed reduced overall hypoglycaemia with IDegAsp compared with BiAsp 30, even in individuals with tight glycaemic control (HbA1c less than 53mmol/mol [7%]).21,23
Some randomised controlled trials comparing IDegAsp with insulin glargine U100 also showed reduced hypoglycaemia rates in the IDegAsp groups, reduced postprandial spikes and lesser nocturnal glucose fluctuations.24-27 At the time of writing, there is no direct comparison of IDegAsp with a basal-bolus regimen of insulin detemir plus mealtime insulin aspart in patients with type 2 diabetes. A phase III study of IDegAsp twice daily compared with insulin degludec once daily and mealtime insulin aspart did not find a significant difference between the two groups in mean HbA1c; however, IDegAsp was associated with reduced hypoglycaemia and weight gain.28 Future studies are required to determine whether IDegAsp can be used three times daily. At present, if additional insulin is required then mealtime insulin aspart can be added to the twice daily IDegAsp dosing schedule.
IDegAsp in type 1 diabetes
The pharmacodynamic profile of IDegAsp has been confirmed in individuals with type 1 diabetes, including older patients.13,29,30 The safety and effectiveness of IDegAsp plus additional insulin aspart has been shown when compared with traditional basal-bolus therapy in patients with type 1 diabetes. In a 56-week study of adults with type 1 diabetes randomly allocated to receive IDegAsp or insulin detemir plus insulin aspart, IDegAsp was associated with lower nocturnal hypoglycaemia rates and lower total insulin dose.31,32
In whom and how is IDegAsp used?
The TGA has approved IDegAsp 70/30 for use by adult patients with diabetes mellitus requiring basal and prandial insulin. The Pharmaceutical Benefits Advisory Committee has recommended that IDegAsp 70/30 be subsidised on the PBS, and it was PBS listed on 1 August 2018.
IDegAsp 70/30 is available in a 3mL disposable pen (100 units/mL). It can be administered once or twice daily with the main meal or meals, defined as the main carbohydrate-containing meals. The insulin dosage should not be titrated more often than once weekly (due to the long half-life of IDegAsp). Titration should be based on fasting plasma glucose measurements from the preceding three days. It is important to note that this differs from the titration schedule for premixed insulin, where the recommended frequency is twice weekly.
IDegAsp provides flexibility with the time of injection, with a dose able to be administered at the next mealtime if an earlier dose is missed. The label states that IDegAsp 70/30 is to be dosed in accordance with individual patients’ needs. A dose given before the evening meal is titrated based on the expected pre-breakfast blood glucose level the following day, and a dose given in the morning is adjusted based on the expected blood glucose level before the evening meal.
For patients switching to IDegAsp from other insulin preparations, a conservative starting dose should be 60 to 70% of total daily insulin requirements, administered with the main meal of the day. However, if the indication for switching insulin is to minimise hyperglycaemia then no dosage reduction is required. For patients switching from a basal-bolus regimen to twice-daily IDegAsp, the previous total daily dose can be divided in two and administered with the two main carbohydrate-containing meals. Supplemental fast-acting insulin may be needed before the remaining meal.23,24
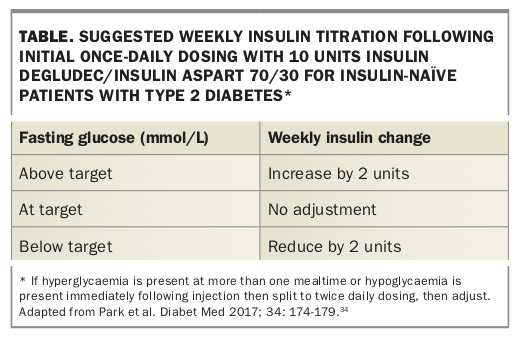
In insulin-naïve adults with type 2 diabetes, a safe pragmatic approach is to start with 10 units of IDegAsp 70/30 once daily, administered with the major carbohydrate-containing meal, and to titrate the dose as described above and in the Table.33,34 It is important to note that fasting glucose targets need to be individualised.
{kind=link}
What are the side effects of IDegAsp?
Adverse reactions reported with IDegAsp in patients with type 1 or type 2 diabetes include nasopharyngitis, upper respiratory tract infection and headache. Serious events include hypoglycaemia, as is the case with all insulin preparations.35
Conclusion
IDegAsp 70/30 is a clinical alternative to premixed insulins for patients with either type 1 or type 2 diabetes. It has some advantages over existing mixed analogue insulins, with reduced hypoglycaemia and improved glucose variability. It is approved for clinical practice. It is important to consider each patient individually before commencing insulin. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.