An updated guide to contraception Part 2: Long-acting reversible methods

Women's health
This second article in an updated three-part series on contraception covers long-acting reversible methods – hormonal and copper-bearing intrauterine devices and the contraceptive implant – which are associated with a lower risk of unintended pregnancy than shorter-acting contraceptive methods. The contraceptive injection is no longer considered a long-acting reversible method, but it continues to play an important role for some women and is included in this article.
- Long-acting reversible contraception (LARC) methods are highly acceptable and offer cost-effective, efficacious contraception.
- The contraceptive implant and intrauterine devices (IUDs) have similar high efficacies in both typical and perfect use.
- There are few absolute or relative contraindications to LARC methods and few serious risks associated with their use.
- Use of LARC has not been shown to have a long-term effect on fertility once the method has been stopped.
- The depot medroxyprogesterone acetate (DMPA) injection is no longer considered a LARC method, because of its lower typical-use efficacy and lack of immediate reversibility, but it continues to play an important role for some women.
- The efficacy of IUDs and the DMPA injection is not affected by the concurrent use of medications that induce liver enzymes.
- The benefits of LARC methods should be discussed with women who present for renewal of oral contraceptive pill or vaginal ring prescriptions.
Long-acting reversible contraception (LARC) methods, namely the intrauterine devices (IUDs) and the contraceptive subdermal implant, have several advantages over other contraceptive methods. LARC methods are highly effective and relatively inexpensive over time compared with combined hormonal methods, as well as having the benefit of ‘fit and forget’. One year after their initiation, the IUD (copper or levonorgestrel) and the etonogestrel (ENG) implant have a continuation rate of about 85%, compared with about 65% for depot medroxyprogesterone acetate (DMPA) injections and combined hormonal contraception.1 In addition, women using implants and IUDs have a 20 times lower risk of pregnancy compared with women using combined hormonal contraceptive methods.2 There is a high uptake of LARC methods by women who are given accurate advice about them.3 Their use in Australia increased from 3% in 20024 to 11% in 2013.5
This article, the second in an updated series of three, includes important information to consider when initiating LARC methods and DMPA injections, as well as some of the common clinical issues that arise during their use. Although the DMPA injection is no longer considered a LARC method due to its lower efficacy in typical use,6 resulting from the need to return for an injection every three months and its unpredictable reversibility, it is included here because it still plays an important role for some women. Other contraceptive methods are covered in other articles in the series. The first, published in the October 2018 issue of Medicine Today, covered aspects of contraception history taking and consultations on contraception choices and discussed the short-acting methods: the contraceptive pills and the vaginal ring. The third article, to be published in a subsequent issue, will cover other methods (barrier, permanent, fertility awareness-based, lactational amenorrhoea and withdrawal) and emergency contraception.
The Medical Eligibility Criteria (MEC) tables for contraceptive use are an internationally recognised system for categorising the risk of various contraceptive methods in women with specific medical conditions (Table 1).7 This categorisation is a useful guide for clinicians in the safe provision of contraceptive methods and is referred to throughout this article.
{kind=link}
Hormonal and copper IUDs
Two types of IUDs are available in Australia: copper and levonorgestrel (LNG). Standard and short-length copper IUDs are available, lasting either five or 10 years. The LNG IUD (marketed as Mirena) lasts for up to five years. Extended use until menopause can be considered for a woman in whom a copper IUD is inserted at the age of 40 years or older, or for a woman aged 45 years or older in whom an LNG IUD is inserted, because of decreasing fertility in this age group.8 Lower-dose hormonal IUDs with smaller frames (marketed in other countries as Kyleena, Jaydess or Skyla, lasting five, three and three years, respectively) may be encountered during consultations but are not yet available in Australia.
The LNG IUD is PBS listed. Although copper IUDs are not PBS listed, they remain cost effective at a cost of about $90, particularly the 10-year devices.
IUDs can be inserted in the primary care setting after the practitioner has completed competency-based training. Although medical indemnity provider requirements vary, additional premiums are generally not required. GPs inserting IUDs are responsible for ensuring they maintain their clinical competence. Insertion of fewer than 10 IUDs over a six- to 12-month period is associated with a higher perforation rate than insertion of greater numbers.9 It is recommended that an assistant be present during insertion and that all practitioners maintain the skills and equipment needed to deal with emergencies, specifically vasovagal reactions, which can occasionally be profound. Where insertion difficulties are predicted or encountered, referral to a gynaecologist or clinic with facilities for sedation or general anaesthesia should be considered.10 IUD removal is a simple procedure that can be performed by all GPs.
Mechanisms of action and efficacy
Both types of IUD act by inhibiting sperm migration to the upper genital tract, inhibiting ovum transport and preventing implantation. In addition, the LNG IUD causes endometrial changes (including atrophy), thickens cervical mucus (preventing sperm penetration) and prevents or delays ovulation in some users, especially during early use. Annual failure rates are estimated to be 0.1% for the LNG IUD and 0.5% for the copper IUD.11 The T-shaped devices appear to be the most effective of the copper devices.12 The efficacy of copper IUDs is slightly lower in women aged 18 to 29 years compared with women in older age groups.11
Initiating IUDs
Both types of IUD can be initiated at any age and used until menopause. Nulliparity is not a contraindication. An Australian study in a family planning clinic setting found that, although 20% of insertions in nulliparous women were rated as difficult, almost 90% of nulliparous women had a successful insertion.13 Use of IUDs in adolescents in Australia remains relatively low, but they are recognised by the American College of Obstetricians and Gynecologists as a first-line adolescent contraceptive method,14 and demand in this age group appears to be increasing in Australia.
Insertion of IUDs should occur at a time when pregnancy can be confidently excluded, although a copper IUD may be used for emergency contraception after unprotected intercourse, before implantation of a fertilised ovum. The ‘quick start’ method of initiation, which can be used for the contraceptive implant and DMPA injection, cannot be used for IUDs because of the potential for an adverse effect on an ongoing pregnancy.
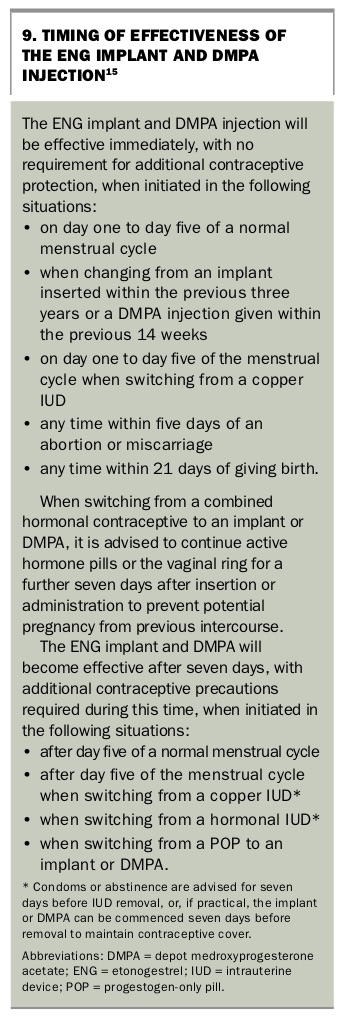
The copper IUD is always immediately effective after insertion. The LNG IUD is immediately effective when inserted on day one to day seven of a normal menstrual cycle and at other specified times, as outlined in Box 1. In most other situations, it will be effective after seven days.
{kind=link}
Contraindications
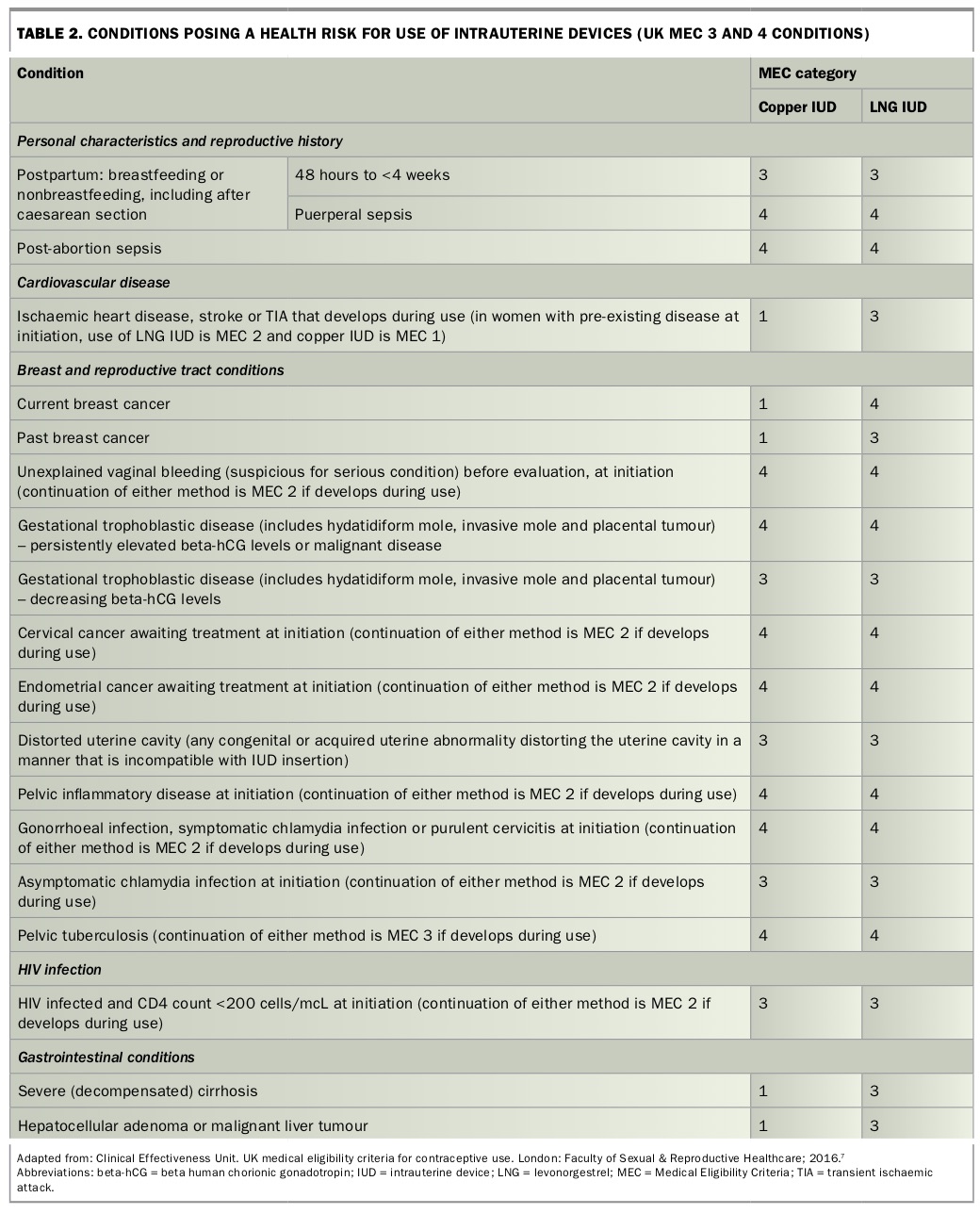
There are few MEC 3 or 4 contraindications to the use of IUDs (Table 2). The most important considerations are undiagnosed abnormal vaginal bleeding, significant distortion of the uterine cavity, cervical infection, current or recent pelvic inflammatory disease and, for women considering an LNG IUD, current or past breast cancer.
{kind=link}
Choosing between a copper and hormonal IUD
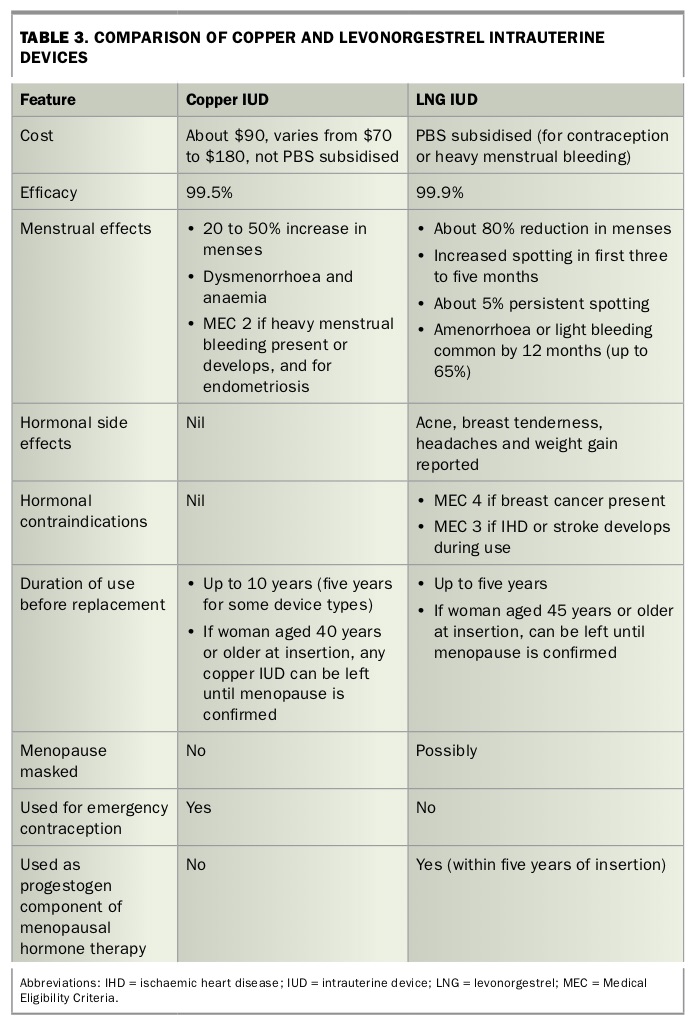
The differences between copper and hormonal IUDs that can assist women in choosing between the two types are outlined in Table 3.
{kind=link}
Examination and investigations
A bimanual and speculum examination is performed before inserting an IUD, noting the position and size of the uterus, the presence of abnormal discharge and any abnormalities that might interfere with IUD insertion or require investigation. This can be done on the day of insertion, when appropriate.
There are no recommendations for routine pre-IUD investigations in asymptomatic women who have a normal examination. A cervical screening test should be performed if due, and screening for chlamydia and gonorrhoea should be considered for women who are at risk of sexually transmitted infections (STIs), particularly women under the age of 30 years.15
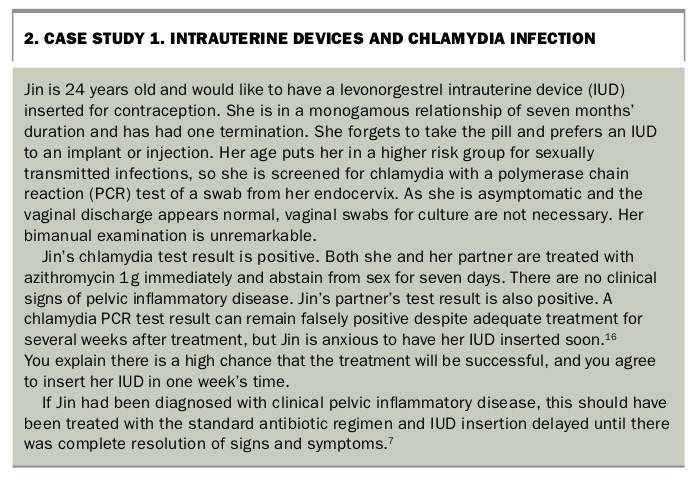
Women with a history of abnormal vaginal discharge or who are clinically assessed as having bacterial vaginosis on examination require investigation before IUD insertion. Bacterial vaginosis requires treatment before or at the time of IUD insertion. Asymptomatic women diagnosed with chlamydia or gonorrhoea should, where possible, be treated before insertion (see Case Study 1 in Box 2).16 For a woman diagnosed with pelvic inflammatory disease, insertion should be deferred until treatment is completed and her symptoms have completely resolved.15
{kind=link}
Women choosing to use a hormonal IUD who have heavy menstrual bleeding require appropriate investigation before insertion, including measurement of serum ferritin levels and a transvaginal ultrasound on day five to day 10 of the cycle to check endometrial thickness and exclude hyperplasia malignancy and other serious conditions. The woman should be reviewed six months after insertion to ensure symptoms have resolved.17
Benefits
The copper and LNG IUDs have several advantages over other contraceptive methods, as they are fit-and-forget methods that provide cost-effective, highly efficacious and long-acting contraception. Both are rapidly reversible on removal and do not affect lactation or infant development.18,19 Their efficacy is not reduced by liver enzyme-inducing medications or malabsorption conditions, and they can be good alternatives for women unable to use oestrogen-containing contraception.20
The LNG IUD is associated with a significant decrease in heavy menstrual bleeding and a reduction in dysmenorrhoea, which can be useful for the management of endometriosis-associated pain.21,22
The copper IUD is the only highly effective reversible nonhormonal method; it can be used as emergency contraception when inserted within five days of unprotected intercourse and will then provide ongoing contraception for up to 10 years.23
Side effects
Expulsion
There is an overall risk of IUD expulsion of about 5%, with the highest risk within the first year of use.10 Women should be advised to check for the presence of the IUD threads monthly (after menstruation if it occurs).
Bleeding patterns
Up to 65% of women using the LNG IUD will have amenorrhoea or light bleeding by 12 months of use.24,25 Unscheduled light bleeding is common during the first three to six months for women using either type of IUD, particularly for LNG IUD users, who may experience daily light bleeding for about three to four months, after which improvement can be expected.26 Copper IUD users can expect heavier, more prolonged menstrual bleeding, which may be more painful. It is important to provide information at the time of insertion about how to manage heavier bleeding with NSAIDs or tranexamic acid.
Pelvic pain and unacceptable menstrual bleeding patterns, including amenorrhoea in LNG IUD users and increased bleeding in copper IUD users, are the most common reasons for discontinuation.27,28
Pregnancy
Although the overall risk of pregnancy in women using IUDs is extremely low, a pregnancy that does occur has a higher risk of being ectopic, compared with pregnancies in women not using an IUD.11
If pregnancy does occur, it is important to determine its location with a transvaginal ultrasound and remove the IUD as soon as possible, provided the woman is in the first trimester. An IUD must always be removed before medical termination of pregnancy and for a continuing pregnancy if possible; if an IUD is not removed, there is a high risk of second-trimester miscarriage, infection or premature delivery.29,30 As the pregnancy progresses, the threads are drawn upwards, making them difficult to locate.
Pelvic infection
In the first 20 days after IUD insertion, there is a small increased risk of procedure-related pelvic inflammatory disease, which may be related to an undiagnosed STI.31 After the first 20 days, the risk of pelvic infection relates to the user’s risk of STIs rather than the presence of the IUD. Apart from procedure-related infection, women with an IUD are at no higher risk of pelvic inflammatory disease than women without an IUD.32 Treatment for pelvic inflammatory disease should be initiated, with review for a response after 48 to 72 hours; if the symptoms have abated, the IUD can be left in place. Prompt specialist referral is required for women who are not improving by this time, to assess the possibility of a rare but serious infection. Pelvic inflammatory disease requires a minimum of two weeks of antibiotic therapy, and follow up and recall systems should ensure that complete resolution occurs.
Hormonal side effects
Although systemic levels of LNG are very low, hormonal side effects, including acne, headache, mood changes, breast tenderness and weight gain, have been reported by some users of the LNG IUD.27 There is a higher systemic exposure to LNG during the first few months of use, and most hormonal symptoms appear to settle over time.33 There is no evidence of a causal link between LNG IUD use and weight gain.34
A Danish national database study found an increased risk of a diagnosis of depression and first prescription of an antidepressant medication in women, especially adolescents, using hormonal methods of contraception, including hormonal IUDs, although a causal association could not be determined.35 Although mood disorders are not a contraindication, IUD users should be advised to return for review should symptoms occur or worsen.
An increased risk of simple ovarian cysts has also been reported, but most are asymptomatic and resolve spontaneously, as for women without an LNG IUD.36
Other side effects
Some male partners report discomfort during intercourse because of IUD threads. This is best avoided by cutting the threads just long enough to sweep behind the cervix (about three to four centimetres from the external os). If the discomfort persists, it may be necessary to cut the threads flush with the os, with the understanding that this will make it harder to check for the presence of the device and may make removal more difficult. Some IUD users experience an increase in vaginal discharge.37
Serious risks
Perforation
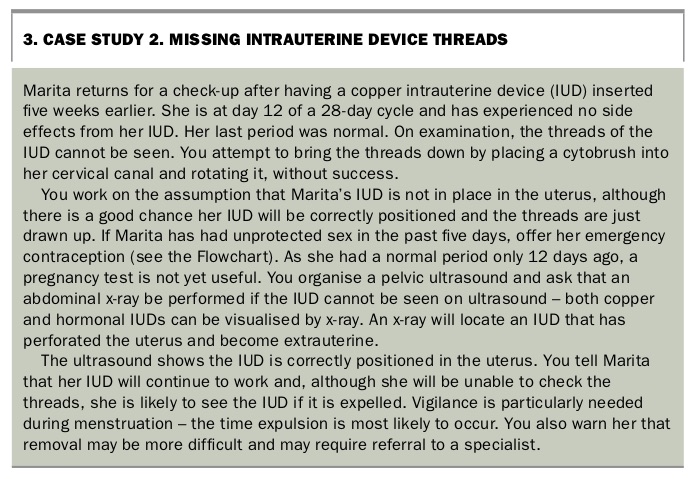
Perforation of the uterus occurs in about two per 1000 IUD insertions, with increased rates during breastfeeding and in the first six months after giving birth.38 Although perforation usually presents soon after insertion, it can be asymptomatic, with delayed detection even years later, so it is essential that it is considered in all cases of ‘missing threads’ (see Case Study 2 in Box 3).9 Laparoscopic removal of the IUD under general anaesthesia may be required in cases of perforation.
{kind=link}
Special situations and management of complications
Missing threads
The management of a woman in whom the threads of the IUD cannot be seen is discussed in Case Study 2 in Box 3 and summarised in the Flowchart.
Infections
The management of a woman wanting to use an IUD who tests positive for chlamydia is discussed in Case Study 1 in Box 2.16
Contraceptive implant
The contraceptive subdermal implant is a progestogen-only contraceptive. The only contraceptive implant available in Australia is a single ethylene vinyl acetate rod that slowly releases the progestogen ENG (Figure). The implant (marketed as Implanon NXT) is listed on the PBS. It lasts for up to three years, after which it needs to be removed and, if desired, replaced. Clinicians also need to be aware of two-rod implant systems (Jadelle and Sinoplant) that are available in other countries (including New Zealand), which release levonorgestrel over a five-year time frame.
{kind=link}
Mechanism of action and efficacy
The ENG implant effectively inhibits ovulation and thickens cervical mucus. It has an estimated failure rate of 0.05% in both typical and perfect use.39 This means that fewer than one in 1000 women will have a pregnancy during each year of use.
Initiating implants
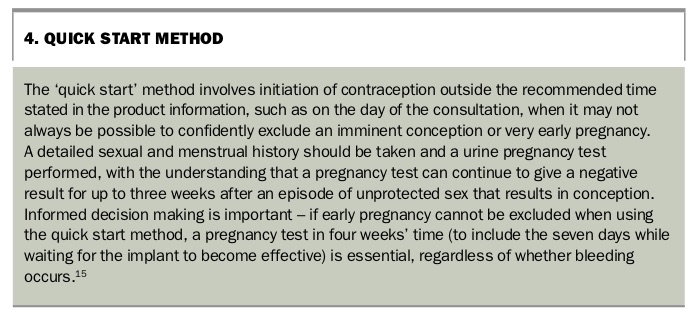
An implant is effective immediately if inserted on day one to day five of a normal menstrual cycle. It can be initiated at other times using the quick start method (Box 4), which requires seven days of use before contraceptive protection is achieved.40 There are no reports of teratogenicity with the implant, but an unintended pregnancy is best diagnosed early to enable consideration of all options, whether that be to continue with the pregnancy and access antenatal care or to terminate the pregnancy.
{kind=link}
Contraindications
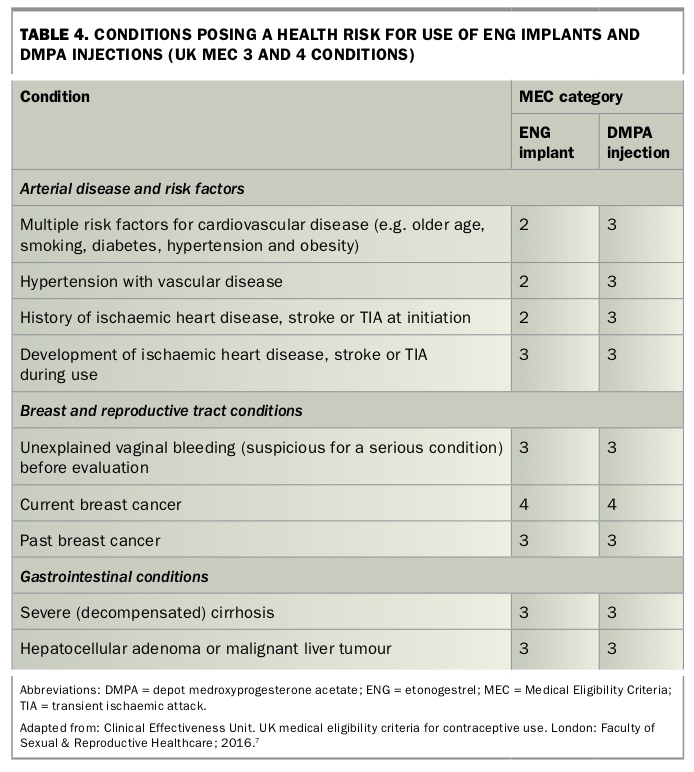
There are few absolute or relative contraindications (MEC 3 or 4) to use of the implant, and it can be used by most women of reproductive age from menarche until menopause, with the exception of women with current or past breast cancer (MEC 4 and 3, respectively) (Table 4).7
{kind=link}
The continued use of the ENG implant is relatively strongly contraindicated (MEC 3) in women who develop arterial disease during use. For example, consideration should be given to removal in a woman who experiences a myocardial infarction or stroke while using an ENG implant.
Drug interactions
Liver enzyme-inducing medications, which include several antiepileptics, antiretrovirals and the herbal remedy St John’s wort, reduce the effectiveness of the ENG implant.41,42 It is recommended that women taking these medications use either an intrauterine contraceptive method or the DMPA injection.20
Examination and investigations
In well women commencing use of the ENG implant, a blood pressure check is the only examination necessary, although a baseline measurement of body mass index (BMI) is useful for documentation of weight gain as a perceived side effect.15 No other routine investigations are necessary.
Benefits
The ENG implant is a highly effective and cost-effective contraceptive, with minimal action required on the part of the user (Box 5). As a nonoral method, it can be useful for women with inflammatory bowel disease or other malabsorptive conditions. It reduces dysmenorrhoea, and some women may find the possibility of amenorrhoea desirable.43 The implant is also an option for women with medical contraindications to, or unacceptable side effects from, oestrogen-containing contraceptives, including a history of venous thromboembolism.
{kind=link}
Insertion and removal of implants are well within the scope of all GPs, although completion of a short training course to ensure correct placement and removal techniques is a necessary requirement or expectation of most medical indemnity providers.44
Side effects and disadvantages
Many side effects are attributed to the ENG implant, but evidence for a causal association is limited. Headaches, mood changes including emotional lability, weight gain, breast tenderness and loss of libido have been reported by users.45 A Danish national database study found an increased risk of depression and first prescription of an antidepressant medication in women, especially adolescents, using hormonal methods of contraception, including implants, although a causal association could not be determined.35 Although mood disorders are not a contraindication to use of an implant,7 users should be advised to return for review should symptoms occur or worsen.
It is important to inform women initiating the ENG implant that their bleeding pattern will change from their usual menstrual cycle and to provide
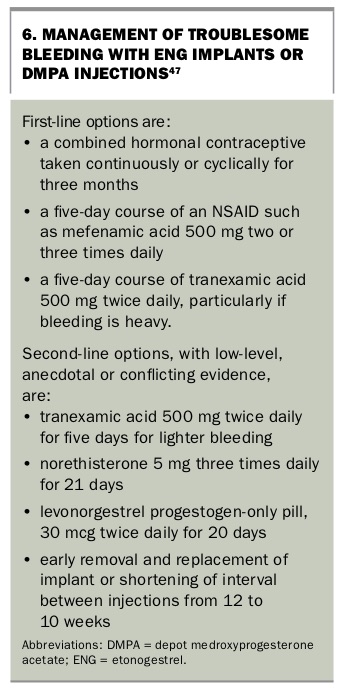
specific information on the range of expected bleeding patterns. The bleeding pattern can vary from amenorrhoea in about 20% of women to frequent bleeding (more than five episodes per 90 days) or prolonged bleeding (an episode lasting more than 14 days) in 25%.46 It is not possible to predict which pattern of bleeding may occur for a woman, and patterns may even change between implants, so it can be useful to explore the woman’s attitudes to unpredictable bleeding before initiation. At the time of insertion, users should also be provided with information about strategies for managing troublesome bleeding, should it occur (see Box 6 and Case Study 3 in Box 7).47
{kind=link}
{kind=link}
Weight gain is a frequently reported side effect of the ENG implant,43,45 although consistent causal evidence of an effect is lacking.34,48 Users may develop acne; however, acne may be improved in users in whom it is pre-existing.43
Insertion and removal of the ENG implant may cause scarring and local reaction and carry a small risk of infection. Deep insertion may sometimes occur, in which case specialist intervention is required for removal. Removal of impalpable implants should only be attempted under ultrasound guidance because of the risk of damage to surrounding neurovascular structures.
Serious risks
Available evidence does not suggest an increased risk of venous thromboembolism with ENG implants,49 and progestogen-only contraceptive methods do not appear to increase the risk of cardiovascular disease, even in smokers.50,51
Management of special situations
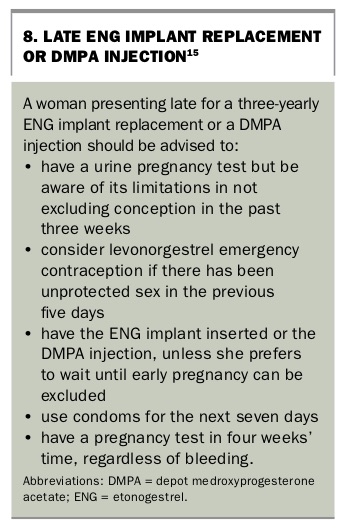
Late for implant replacement
The management of a woman presenting late for a three-yearly ENG implant replacement is summarised in Box 8.
{kind=link}
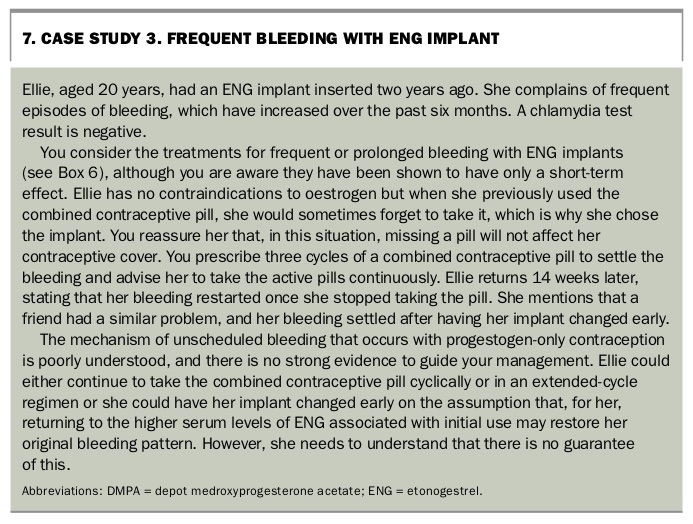
Frequent or prolonged bleeding
The management of a woman with an ENG implant presenting with frequent bleeding is discussed in Case Study 3 in Box 7, and treatment options for frequent or prolonged bleeding are outlined in Box 6.47
Contraceptive injection
The contraceptive injection (marketed as Depo-Provera or Depo-Ralovera) is a progestogen-only method delivering DMPA 150 mg as an intramuscular injection every 12 ± 2 weeks. It is PBS listed. It works by inhibiting ovulation and thickening the cervical mucus.
Although over 99% effective in perfect use, it is less effective than the implant and IUDs in typical use because of the need to return to the clinic for repeat injections, with up to four in 100 users becoming pregnant during the first year of use.6 A lower-dose subcutaneous formulation of medroxyprogesterone acetate, which can be self-injected every 12 weeks, is available in other countries and removes the need for regular clinic attendance.52
Initiation
The injection is effective immediately if initiated on day one to day five of a normal menstrual cycle, as well as in specific other circumstances (Box 9). Although it is preferable to exclude early pregnancy before administration, DMPA can be initiated using the quick start method, even when there is a small risk of an undetectable early pregnancy, if the woman could be put at higher risk of an unintended pregnancy as a result of a delayed start (Box 4).40 There are no reports of teratogenic effects if an injection is inadvertently given in early pregnancy.53 It takes seven days for the injection to become effective using the quick start method, and a pregnancy test four weeks after initiation is essential. Women who present late (more than 14 weeks) for a repeat injection can be managed as summarised in Box 8. They can be given the option of an immediate injection using quick start, rather than a deferred injection with a urine pregnancy test performed after three weeks of abstinence or protected intercourse (see Case Study 4 in Box 10).
{kind=link}
{kind=link}
{kind=link}
Contraindications
Like all hormonal methods, DMPA is MEC 4 and 3, respectively, for women with current or past breast cancer. It is also MEC 3 (risks outweigh the benefits) in women with multiple cardiovascular risk factors, including a history of ischaemic heart disease, stroke or transient ischaemic attacks (Table 4).7 DMPA is not a first choice for women at risk of bone density loss, including those using long-term steroids or with immobility issues.15,20
Drug interactions
DMPA is not affected by concurrent use of liver enzyme-inducing drugs and may be a contraceptive of choice in this instance.
Examination and investigations
A blood pressure check is the only examination required at initiation and annually, although a baseline BMI measurement may be useful, as weight gain is a recognised side effect of DMPA. Routine bone density testing is not recommended, but annual review of risk factors for bone loss is advised. Measurement of lipid levels is recommended for women with cardiovascular risk factors who are considering this contraceptive method.
Benefits
DMPA is highly effective and relatively cost-effective. It can be used by women with malabsorptive conditions and may be useful for those with endometriosis and heavy menstrual bleeding, given its effect on reducing dysmenorrhoea and menstrual blood loss, with at least 50% of women using DMPA becoming amenorrhoeic.55,56
The concept of reproductive coercion is increasingly recognised within the spectrum of intimate partner violence and includes situations in which the use of contraception may need to be hidden from a partner.57 As DMPA can be easily concealed from others, it may be the most appropriate choice in this context.
Side effects and disadvantages
Headache, mood changes, breast tenderness and loss of libido have been reported by users.55 Use of DMPA appears to be associated with weight gain in some users, especially adolescents who are already overweight. Studies suggest that early weight gain predicts later increases, with continuing weight gain for the 20 to 25% of women who gained more than 5% of body weight in the first six months.58-60
Once given, the effect of the DMPA injection cannot be immediately reversed. There can be a delay in return to fertility of up to 18 months after DMPA discontinuation, but there is no evidence of long-term reduction in fertility in past users.61
Although irregular spotting or bleeding can occur, at least 50% of users are amenorrhoeic by 12 months of use.55 Management of troublesome bleeding is outlined in Box 6.
Use of DMPA is associated with about a 7% mean reduction in hip and spine bone density compared with nonusers over a period of four years.62 This effect is considered reversible in adult users;63 the limited information available for adolescents shows that it may be substantially or fully reversible in this age group.64,65 Evidence on fracture risk is inconclusive.66,67 Because of the theoretical concerns relating to its impact on bone density, use of DMPA in adolescents aged under 18 years and women over 45 years is classified as MEC 2. This means that, although not always a first choice, DMPA can be used for women in whom other methods are unsuitable. New users should have a detailed assessment and receive advice regarding osteoporosis risk factors; this should occur every two years for continuing users.15
Although progestogen-only contraceptives do not appear to increase the risk of cardiovascular disease, even in smokers,50,51 there is a theoretical concern about DMPA’s hypo-oestrogenic effect on reducing HDL-cholesterol levels.68 It is advised to switch to another contraceptive method at the age of 50 years, as the risks of DMPA to both bone health and cardiovascular health (due to its effect on lipids) generally outweigh the benefits.69
Conclusion
LARC methods, including the contraceptive implant and copper and hormonal IUDs, have low failure rates and few contraindications. Uptake of these fit-and-forget methods is increasing in Australia.4 They offer several benefits over other contraceptive methods and can be considered as first-line methods of contraception in most situations. GPs are ideally placed to provide access to and information on all LARC methods and to either initiate their use or, in the case of IUDs, ensure there is a rapid referral pathway in place for insertion if they are not providing this service. The benefits of LARC methods should be discussed with women who present for renewal of oral contraceptive pill or vaginal ring prescriptions. MT
of Family Planning NSW from Bayer Healthcare
and MSD. Family Planning NSW and Family Planning Victoria receives funding for educational courses, research and training from Bayer Healthcare and MSD.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.