Insulin in type 2 diabetes: initiating and titrating treatment

Diabetes type 2
Diabetes medicines
Despite insulin being the most effective medication for lowering HbA1c levels in people with type 2 diabetes there is significant inertia with regard to initiating treatment and titrating the dose. This article discusses when insulin should be initiated and how it can be titrated in the community.
Correction
A correction for this article was published in the June 2019 issue of Medicine Today. The online version and the full text PDF of this article (see link above) have been corrected.
The prevalence of type 2 diabetes around the world is increasing and is associated with significant morbidity and mortality from the microvascular and macrovascular complications of longstanding hyperglycaemia. Over the past 10 years many new classes of drugs have become available for treating type 2 diabetes. Despite these advances, insulin is still the most effective medication for reducing glycated haemoglobin (HbA1c) levels.1 Insulin is often initiated as a last resort when multiple oral hypoglycaemic agents have failed to achieve a target HbA1c level, despite evidence that optimal glycaemic control within the first 10 years after diagnosis has long-term benefits in terms of reduced risk of complications.2
The importance of optimal glycaemic control
It is well known that there is a significant correlation between hyperglycaemia and the complications of diabetes. Observational data from the UK prospective diabetes study (UKPDS) showed that for each 1% reduction in mean HbA1c level there was a relative risk reduction of 21% for any diabetes-related endpoint (i.e. myocardial infarction, stroke, microvascular endpoints, cataract extraction, lower extremity amputation, fatal peripheral vascular disease, heart failure) and similarly for diabetes-related mortality. Relative risk reduction varied for individual factors and was most profound for microvascular complications (37%).2
Glycaemic targets
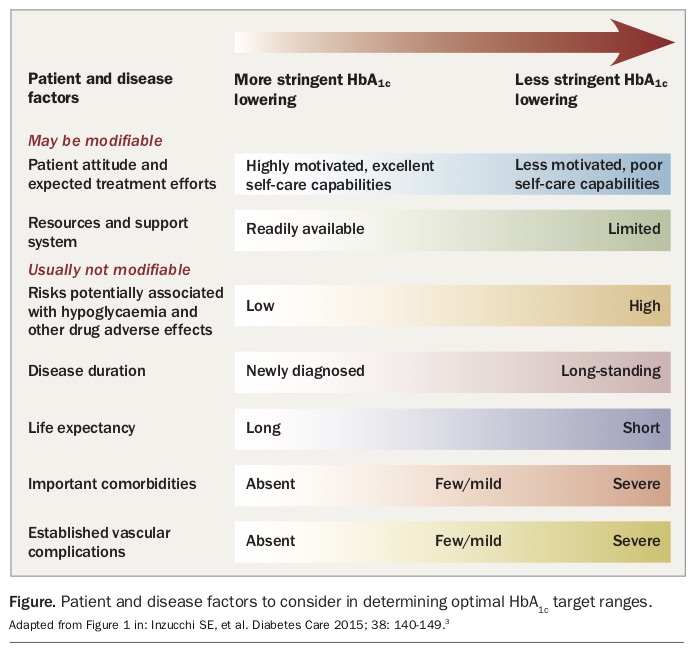
The American Diabetes Association and the European Association for the Study of Diabetes recommendation on target HbA1c level is that a personalised approach is necessary.3 For many patients with diabetes a target HbA1c level of less than 7.0% (53 mmol/mol) is optimal to reduce the risk of complications.4 Ideally, the fasting blood glucose level (BGL) should be maintained at 6 to 8 mmol/L and postprandial BGL at 8 to 10 mmol/L.5 Conversely, aggressive control in older patients with established complications may not have significant benefits and runs the risk of hypoglycaemia.3 Less strict HbA1c targets of 7.5 to 8% (58 to 64 mmol/mol), or even slightly higher, are therefore reasonable.4
Factors that should be considered when deciding a patient’s target HbA1c level are shown in the Figure.3
{kind=link}
Initiating insulin
Basal insulin
Metformin remains the initial drug of choice for patients with a new diagnosis of type 2 diabetes. Patients with a higher HbA1c level at diagnosis (≥9.0%) will usually require two noninsulin formulations or insulin to reach their target level, and therefore it is reasonable to start insulin as part of combination therapy in this situation.4 In the absence of marked hyperglycaemia and/or symptoms, a basal insulin alone is often sufficient. Basal insulin is typically commenced using insulin glargine 100 units/mL at a dose of 10 units daily.5 Insulin glargine 300 units/mL is a new basal insulin formulation that has a longer duration of action and is associated with fewer hypoglycaemic events than the less concentrated formulation.6 It is commenced at a dose of 0.2 units/kg daily.7 A unit-to-unit conversion is used when switching patients from once-daily insulin glargine 100 units/mL to once-daily insulin glargine 300 units/mL. Patients switching from twice-daily insulin glargine 100 units/mL to once-daily insulin glargine 300 units/mL should reduce their daily dose by 20%.7
There are multiple resources available to guide stepwise optimisation of glycaemic control in patients who are already on noninsulin medication but are not reaching their target HbA1c level.4,5 When choosing the best approach for your patient, keep in mind the expected decrease in HbA1c level that could be anticipated with each agent, in addition to the other potential risks and benefits of each class of medication. Given that insulin is the most effective medication for reducing HbA1c level it should be considered early in the management of patients with an HbA1c level of more than 9.0% in whom tighter glycaemic control is desirable.1
Prandial insulin
The addition of a prandial insulin should be considered in the following situations:4
- the fasting BGL is within target ranges but the HbA1c level remains above target three to six months after basal insulin titration
- postprandial BGLs are more than 10.0 mmol/L.
Initially, a ‘basal-plus’ schedule, with added prandial insulin at a starting dose of 4 units, may only be required with the meal containing the largest carbohydrate content.5 Basal insulin should be continued at the same dose, as should metformin. If the HbA1c level is still not at target after three months of titration a further dose of prandial insulin should be added to another meal at a starting dose of 4 units. If target HbA1c level is still not achieved after appropriate titration, prandial insulin should be added to the third meal (i.e. a ‘basal-bolus’ schedule).5 Sulfonylureas are usually ceased once patients are taking any prandial insulin.
Combination insulins
Premixed insulin (a fixed combination of an intermediate-acting insulin with a prandial insulin) is another option for people who eat regularly and would prefer a simpler schedule. Mixed insulins are traditionally administered twice daily with the two largest meals of the day, but can be used only once or even three times daily if required. They can be more difficult to titrate owing to the fixed combination of intermediate-acting and prandial insulin.4 A premixed insulin is usually commenced in an insulin-naive patient at a dose of 10 units administered just before the largest meal.5
A novel insulin coformulation that is a combination of an ultra-long-acting basal insulin (insulin degludec, 70%) and short- acting insulin (insulin aspart, 30%), which has distinct basal and prandial glucose-lowering effects, is now available on the PBS. In a 26-week, randomised, open-label, multinational phase IIIa trial it was found to be associated with less hypoglycaemia than biphasic insulin aspart in patients previously treated with premixed insulin with suboptimal glycaemic control, while being noninferior for reduction in HbA1c levels.9 If indicated, this coformulation can be commenced in insulin-naive patients once daily with the largest carbohydrate meal at a dose of 10 units, but it can be uptitrated to twice daily as needed.8
Titrating insulin
The target BGLs given in this section with regard to optimising the insulin dose apply to patients with a target HbA1c level of less than 7.0% (53 mmol/mol).
Basal insulin only
After starting insulin, the basal insulin dose can be increased by one to two units at a time (or 5 to 10% of the daily insulin dose in those on higher doses) to achieve fasting glycaemic targets of 6 to 8 mmol/L.4,5 These adjustments can be made every three to seven days and can often be done at home by the patient with sufficient support from their diabetes educator, practice nurse or GP. A randomised study involving 4961 patients with type 2 diabetes from 59 countries who were starting insulin found that subject-driven titration every three days was not associated with more hypoglycaemia than physician-driven titration and achieved a lower HbA1c level after 24 weeks.10
Basal insulin plus prandial insulin
For patients who are taking basal and prandial insulin, the most accurate way to adjust prandial insulin involves asking the patient to check their BGL before a meal and two hours after a meal. Dose adjustments are made according to the two-hour postprandial BGL, aiming for a postprandial level of 6.0 to 7.9 mmol/L. If the two-hour postprandial BGL is 8 mmol/L or more for three consecutive days the prandial insulin can be increased by 2 units. Conversely, if the two-hour postprandial BGL is less than 5.9 mmol/L the prandial insulin should be reduced by 2 to 4 units, especially if there are any BGL readings below 4.0 mmol/L.5
Premixed insulin
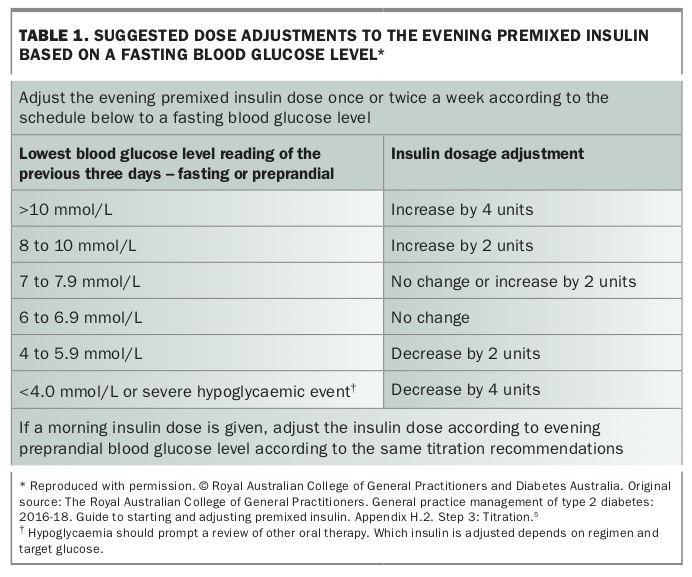
The evening premixed insulin dose is adjusted according to the fasting BGL to a target of 6 to 6.9 mmol/L. Suggested dose adjustments based on the fasting BGL are provided in Table 1.5 As mixed insulin is usually used twice a day most people are also taking mixed insulin in the morning. The dose of the morning insulin is adjusted using the same scale, based on the evening preprandial BGL.
{kind=link}
Changing from a basal insulin to a twice daily premixed insulin
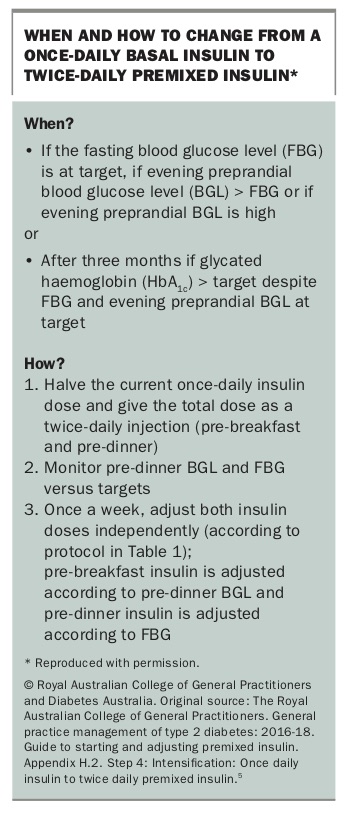
Changing from a basal insulin to a twice-daily premixed insulin may be considered when the evening preprandial BGL is high and the fasting BGL is within target, or if after three months the patient has not reached their target HbA1c level. In this situation it is recommended to halve the current once-daily basal insulin dose and give the total premixed insulin dose over two daily injections given just before breakfast and dinner (Box).5
{kind=link}
When switching from a once-daily basal insulin to a once-daily premixed insulin schedule the premixed insulin should be given at the same unit dose and administered with the meal with the largest carbohydrate content. After starting premixed insulin, patients – especially the elderly – need to closely monitor their BGLs with appropriate input from a dietitian and a diabetes educator to avoid the risk of hypoglycaemia from the short-acting component.8
Insulin formulations in Australia
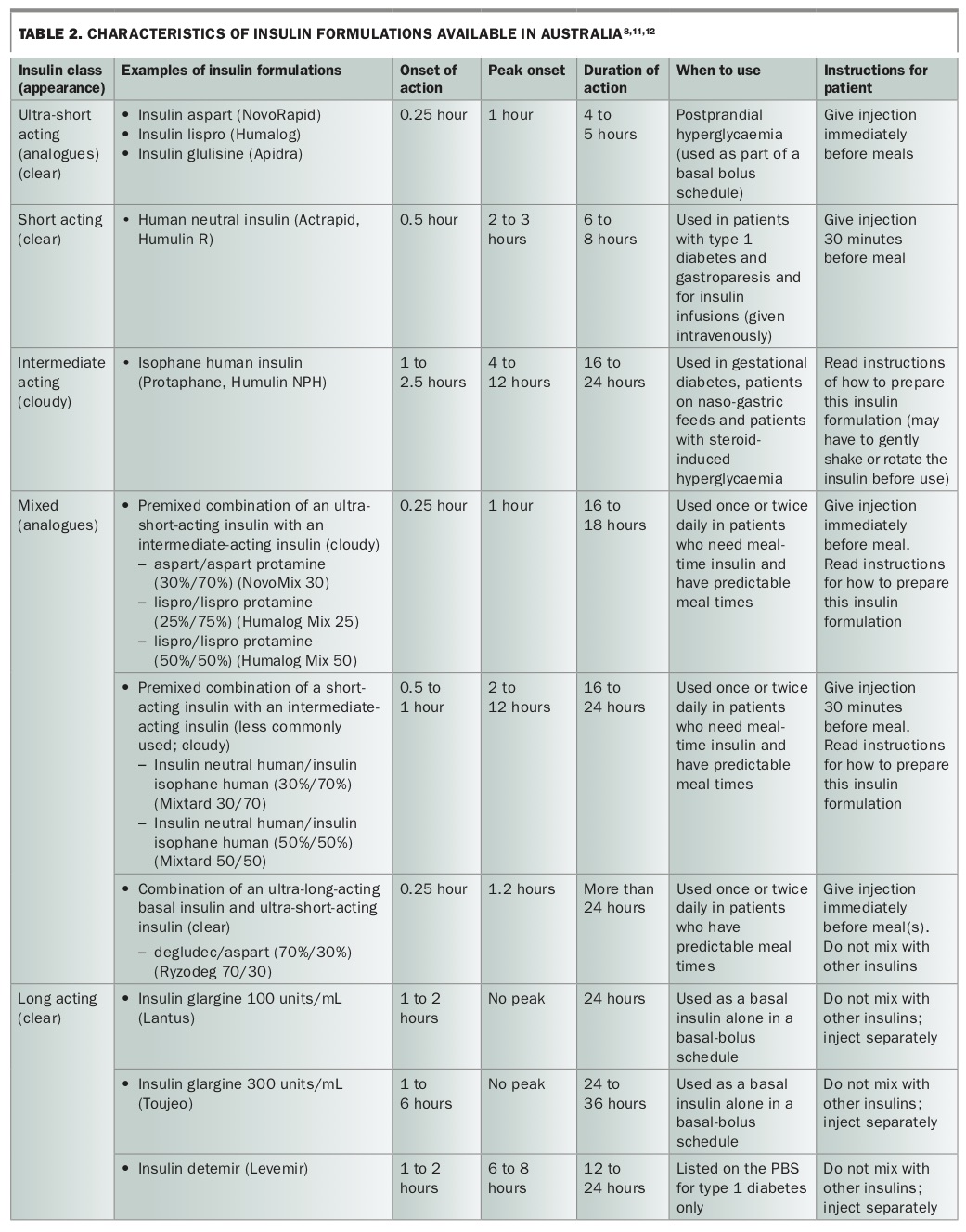
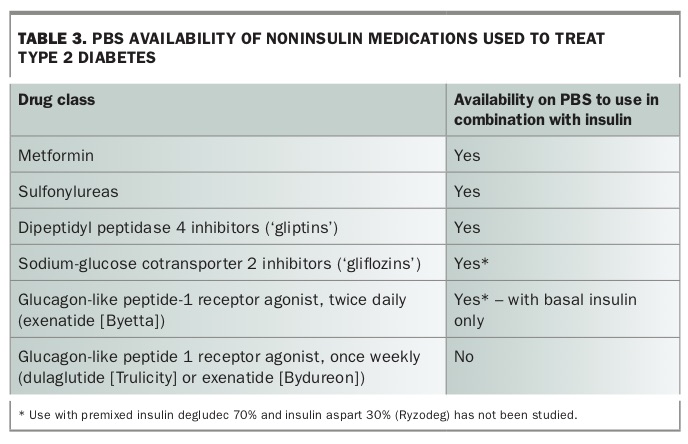
Five classes of insulin are available in Australia and are classified according to their duration of action (Table 2).8,11,12 Table 3 provides a list of other medications used to treat type 2 diabetes and their current availability on the PBS for use with insulin.
{kind=link}
{kind=link}
Barriers to initiating insulin
The mean HbA1c level in people with type 2 diabetes is typically 1.5 to 2.0% above target before insulin is commenced: 9.3% (78 mmol/mol) in the UK, 8.6% (70 mmol/mol) in the US and 9.4% (79 mmol/mol) in Australia (after a median duration of 8.1 years).13 The delay in both initiation and titration of insulin can be due to multiple factors.14
Healthcare professional factors
A questionnaire distributed to 600 physicians from Germany, Japan, Spain, Turkey, the UK and the US found that 30% of primary care physicians never or rarely intensified insulin treatment, compared with 4% of specialists.15 The main barriers as self-reported by physicians were lack of experience with the available insulins (49%) and the considerable amount of time it takes to educate patients about insulin intensification (49%); and 32% of physicians disagreed with the statement that administration of intensified insulin therapy was technically easy.15 Concern about hypoglycaemia remains a major obstacle to initiating more intensive treatment among both primary care physicians and diabetes specialists.16
Patient factors
In a survey in the US involving 1653 people with type 2 diabetes, treatment with oral medications was rated the management approach that was least burdensome, even less so than a moderate diet. The burden ratings increased with an increasing number of insulin injections per day and with checking the BGL more often.17
A global study found that 33.2% of patients had self-reported insulin omission or nonadherence on at least one day in the past month, with an average of 3.3 days. The most commonly reported reason was being too busy (18.9%), and simply forgetting to take insulin was reported by 7.4% of patients.16 Only 3.8% of patients reported the schedule was too complicated, and 2.6% reported painful injections as a reason for insulin being missed or not taken as prescribed.16
Health system factors
Starting and titrating insulin in the primary care setting might be avoided by some physicians because of the misconception that it is too time consuming. A cluster randomised controlled trial conducted in Victoria looked at insulin intensification in the primary care setting. In this ‘stepping up’ model of care the practice nurse played a lead role in insulin initiation and intensification, mentored by a diabetes educator and in liaison with the GP.13 GPs and practice nurses assigned to an intervention had a 60 to 90 minute on-site briefing and training session followed by ongoing support as they worked with patients over the 12 months of the study. After 12 months there was a statistically significant difference in HbA1c level (mean difference, -0.6%; 95% CI, -0.9% to 0.3%; p<0.001), favouring the intervention.13 Most of this change was seen by six months. Insulin was commenced sooner (32 days) in the intervention group than the control group (85 days) and short-acting insulin was commenced more commonly (17 patients vs one patient).13 A target HbA1c level of less than 7.0% (53 mmol/mol) was achieved by 54 patients (36%) in the intervention group compared with 22 patients (19%) in the control group.13 This study showed how pre-existing resources can be utilised in a multidisciplinary approach to get the best outcomes for patients.
Conclusion
Type 2 diabetes is associated with significant morbidity and mortality and the incidence of the disease is increasing. Treatment schedules have become more complicated over the past 10 years with the addition of new agents, but insulin remains the most effective agent for lowering HbA1c level. There are significant delays in both initiating and uptitrating insulin, and many patients are commenced on insulin as a last resort after years of suboptimal control. It is important for both specialists and primary healthcare providers to recognise the factors that contribute to this delay. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.