Liraglutide: for obesity, not just type 2 diabetes


Obesity
Weight control
Liraglutide is TGA approved as an adjunctive therapy for obesity, extending its indications for use beyond treatment of type 2 diabetes. What is its place in helping patients achieve and maintain weight loss?
The chronic nature of obesity has led to renewed interest in pharmacotherapy as an adjunct to lifestyle intervention for achieving and maintaining weight loss. Liraglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist that was previously TGA approved for the treatment of type 2 diabetes, at a dose of 1.8 mg daily. In December 2015, the TGA approved a liraglutide product with a higher daily dose (3 mg) for the treatment of obesity. The 3 mg product has potential as a long-term obesity therapy, although current long-term safety and efficacy data are limited.
The weight loss effects of the 3 mg liraglutide product appear superior to those of orlistat, the only other approved long-term obesity pharmacotherapy. The 3 mg liraglutide product can be prescribed by GPs, although the cost of a private prescription ($387 per month) may prove prohibitive for many patients.
What is liraglutide?
Liraglutide is an analogue of human GLP-1, a hormone that suppresses appetite and stimulates insulin secretion. Weight loss with liraglutide appears to be due to reduced appetite and energy intake.1 Peripherally, GLP-1 receptor agonists slow gastric emptying, causing early satiety. Gastrointestinal adverse effects associated with these agents, such as nausea and vomiting, likely also contribute to reduced appetite.2,3
Weight loss associated with GLP-1 receptor agonists can, however, occur in the absence of nausea and vomiting and independent of delayed gastric emptying.4 Recent studies suggest that the weight loss effects of liraglutide may therefore be predominantly mediated through its action within the central nervous system, as liraglutide is able to cross the blood–brain barrier.5,6 This central induction of satiety may explain the greater weight loss effects seen with liraglutide compared with other larger nonpeptide GLP-1 receptor agonists.
How does liraglutide compare with other agents?
Trials of the lower-dose liraglutide product in the treatment of patients for type 2 diabetes consistently found it to be associated with modest weight reduction.7,8 This finding led to three trials in adults with obesity or overweight without diabetes, which confirmed a dose-dependent weight reduction with liraglutide.9-11
In a 56-week randomised placebo-controlled trial involving more than 3700 adults, the 3 mg liraglutide product in conjunction with lifestyle intervention was associated with a mean 8.4 kg reduction in body weight, compared with 2.8 kg for placebo (lifestyle intervention alone) – i.e. a 5.6 kg mean-subtracted weight loss with liraglutide.12 Among participants receiving liraglutide, 63% lost at least 5% of their initial body weight, and 33% lost at least 10%, compared with 27% and 11%, respectively, of those receiving placebo. Liraglutide was also associated with a significant improvement in cardiometabolic risk factors, including reductions in waist circumference, blood glucose level, blood pressure and sleep apnoea.12 The cardiovascular benefits of liraglutide were confirmed by the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial which reported lower cardiovascular mortality and morbidity (nonfatal myocardial infarction or stroke) in patients with type 2 diabetes treated with liraglutide 1.8 mg compared with placebo over a median follow up of 3.8 years.13
Two other trials in obese and overweight adults without diabetes directly compared liraglutide (at varying doses) with orlistat in conjunction with lifestyle intervention as well as with placebo (i.e. lifestyle intervention alone).10,11 In the earlier of these trials, the mean weight loss with liraglutide was 4.8 kg (for the 1.2 mg dose), 5.5 kg (1.8 mg dose), 6.3 kg (2.4 mg dose) and 7.2 kg (3 mg dose), compared with 4.1 kg for orlistat and 2.8 kg for placebo.10 A follow-up one-year open-label extension study assessed the safety and efficacy of higher-dose liraglutide (initial maintenance dose of 2.4 mg subsequently increased to 3 mg) compared with orlistat. After two years, those taking liraglutide 2.4/3.0 mg sustained a mean weight loss of 7.8 kg from baseline, 3.0 kg greater than the orlistat arm and unchanged from the end of the first year.11
There are no head-to-head studies directly comparing currently available pharmacotherapy. By way of comparison, phentermine, which is an option for short-term (less than three months) weight management therapy in conjunction with lifestyle modification, is associated with weight loss that is about 3.6 kg greater than with placebo (95% confidence interval [CI], 0.6 to 6.0 kg).14 Orlistat, which is approved for long-term weight management and is available without a prescription, is associated with a mean weight loss of 2.89 kg (CI, 2.27 to 3.51 kg) at 12 months.14 Naltrexone hydrochloride/bupropion hydrochloride extended release 8/90 mg combination therapy is the most recent obesity pharmacotherapy approved in Australia. It has a four-week dose escalation schedule, and weight loss of 9 kg compared with 5.2 kg for lifestyle intervention alone has been reported in key studies.15
When is liraglutide used?
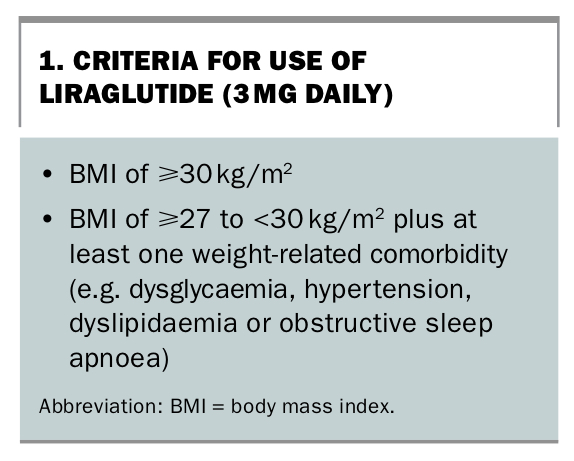
The 3 mg liraglutide product is TGA approved as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adults. Criteria for its use are shown in Box 1.
{kind=link}
The 3 mg liraglutide product appears more effective than orlistat, which is also TGA approved for chronic weight management. However, longer-term safety and efficacy data are available only for orlistat because it has been available for many years.
How is liraglutide used?
Liraglutide is injected once daily subcutaneously into the abdomen, thigh or upper arm. To minimise the gastrointestinal adverse effects, liraglutide should be started at 0.6 mg daily for one week and increased by 0.6 mg daily at weekly intervals until the maximum 3 mg daily dose is achieved.
GPs should keep in mind the ‘stopping rule’ for the 3 mg liraglutide product for obesity: treatment should be discontinued after 12 weeks on the maximum 3 mg daily dose if the patient has not lost at least 5% of their body weight. Given the lack of long-term safety and efficacy data, therapy continuation should be re-evaluated at this time (i.e. week 16 after treatment initiation) and in an ongoing manner thereafter.
As the 3 mg liraglutide product is approved for chronic weight management, it seems reasonable for patients to continue therapy until they have lost 5 to 10% of their baseline body weight and potentially longer if there is evidence of further and/or durable weight loss associated with treatment. In practice, treatment duration with the 3 mg liraglutide product will ultimately be determined by its cost. Postmarketing studies assessing its longer-term safety will also provide further guidance on treatment duration.
There is no evidence at present for the efficacy of recommencing the 3 mg liraglutide product for patients who regain weight after treatment cessation. However, it seems reasonable to speculate that reintroducing liraglutide treatment might be of benefit, although there may be a role for alternative interventions, including bariatric surgery.
Adverse effects of liraglutide
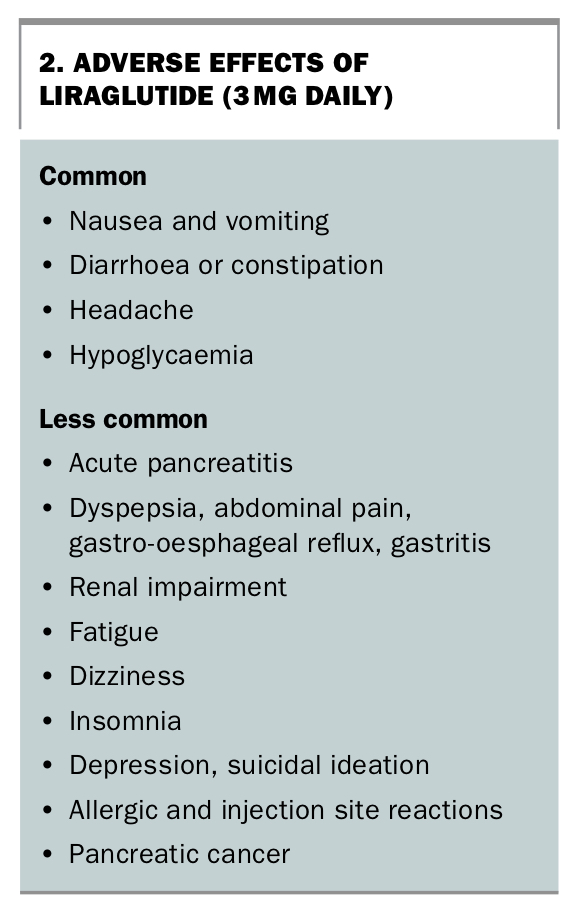
Liraglutide is commonly associated with gastrointestinal adverse effects that are generally self-limiting, including nausea, vomiting, diarrhoea or constipation (Box 2). Other frequent adverse effects are hypoglycaemia, particularly in patients with type 2 diabetes, and headache.12
{kind=link}
Uncommon adverse effects of liraglutide include acute pancreatitis and other gastrointestinal effects, such as dyspepsia, abdominal pain, gastro-oesophageal reflux and gastritis. Although an increased incidence of pancreatic cancer was noted in ongoing studies of the GLP-1 receptor agonist class, this does not appear to be an issue in usual clinical management at this stage. Renal impairment due to severe dehydration from nausea and vomiting has also been reported. Liraglutide is also associated with central nervous system effects, including fatigue, dizziness, insomnia, suicidal ideation and depression.16 Allergic and injection site reactions can also occur.
Precautions
It is important to note that there are no long-term safety data for the 3 mg liraglutide product. For example, it is associated with an increase in heart rate, but the effects on cardiovascular morbidity and mortality for the 3 mg liraglutide product have not been definitely established, although as discussed above, the results of the LEADER trial appear reassuring.13
Liraglutide is contraindicated in patients with a personal or family history of medullary thyroid cancer or multiple endocrine neoplasia syndrome type 2, because of an increased incidence of thyroid C-cell tumours observed in rodents.17 It is also contraindicated in those with hypersensitivity or a history of angioedema with other GLP-1 receptor agonists and in pregnancy.
The 3 mg liraglutide product is not indicated for the treatment of type 2 diabetes and should not be used in combination with other GLP-1 receptor agonists or with insulin. It has not been studied in patients with a history of pancreatitis.
Conclusion
It is well recognised that weight reduction of 5 to 10% from baseline reduces cardiometabolic morbidity and mortality and improves quality of life in patients who are overweight or obese. Although weight loss can be achieved through lifestyle interventions, maintenance of weight loss remains difficult. Liraglutide is the first GLP-1 receptor agonist to be approved as obesity pharmacotherapy and it achieves superior weight loss compared with the only other long-term obesity pharmacotherapy, orlistat. The acceptability, durability of effect and long-term safety of liraglutide for weight loss remain to be seen. Moreover, as liraglutide is not PBS approved, GPs may find the cost prohibitive for their patients. MT