Is it IBD? Making an accurate and prompt diagnosis

Abdominal symptoms thought to be related to the lower gut (ileum and colon) are common, and most do not represent inflammatory bowel disease. Making an accurate and prompt diagnosis in general practice can be challenging at times. However, being aware of the range of differential diagnoses and the ways in which we can best estimate the pretest probability of each condition to enhance diagnostic accuracy is relatively straightforward.
- The cardinal symptoms of diarrhoea (with or without blood) and abdominal pain represent a common clinical scenario in general practice, and not all patients with these symptoms have inflammatory bowel disease (IBD) or require extensive work up or referral to a specialist.
- There is no single test that diagnoses IBD; diagnosis is based on a combined approach of clinical history, biomarkers, endoscopic, radiological and histological assessment.
- Many non-IBD-related colitides share basic clinical features with IBD; however, symptom pattern, time course, age group and other risk factors identifiable in the patient’s history can be used to guide accurate diagnosis.
- Reviewing potential differential diagnoses should guide the search for the underlying cause.
Evaluation of patients with suspected inflammatory bowel disease (IBD) requires a purposeful approach to considering differential diagnoses. The cardinal symptoms of diarrhoea (with or without blood) and abdominal pain represent a common clinical scenario in general practice, and not all patients with these symptoms have IBD or require extensive work up or referral to a specialist.
Irritable bowel syndrome (IBS), seen in up to 10% of people in the general population, is one of the conditions with these presenting symptoms.1 Accurate diagnosis avoids unnecessary investigations such as CT scans and colonoscopies, which are often overused in assessing patients with these symptoms. Inflammation of the ileal or colonic mucosa (referred to as ileocolitis) can be due to conditions other than IBD, including infections or drugs such as NSAIDs. Differentiation is necessary as treatments differ substantially. Many non-IBD-related colitides share basic clinical features with IBD; however, symptom pattern, time course, age group and other risk factors identifiable in the patient’s history can be used to guide accurate diagnosis. This review provides a brief overview of some of the relevant differential diagnoses and an approach to stepping through the initial clinical assessment.
Inflammatory bowel disease
IBD is a chronic immune-mediated condition with a relapsing-remitting course. Crohn’s disease and ulcerative colitis are the two most common IBD subtypes. However, in 5 to 15% of patients a clear distinction cannot be made despite endoscopic, radiological and histological assessment and a diagnosis of IBD-unclassified is made.2
Australia has one of the highest reported incidence rates of IBD internationally.3 IBD leads to significant morbidity and economic burden on society, with costs of more than $380 million from loss of productivity per annum.4,5
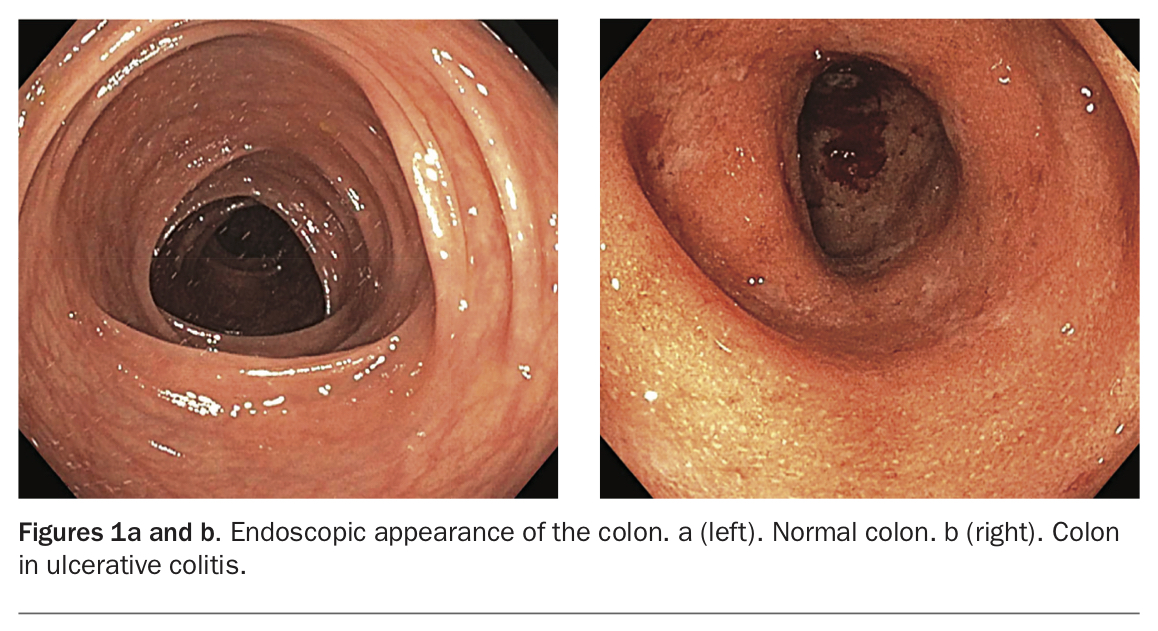
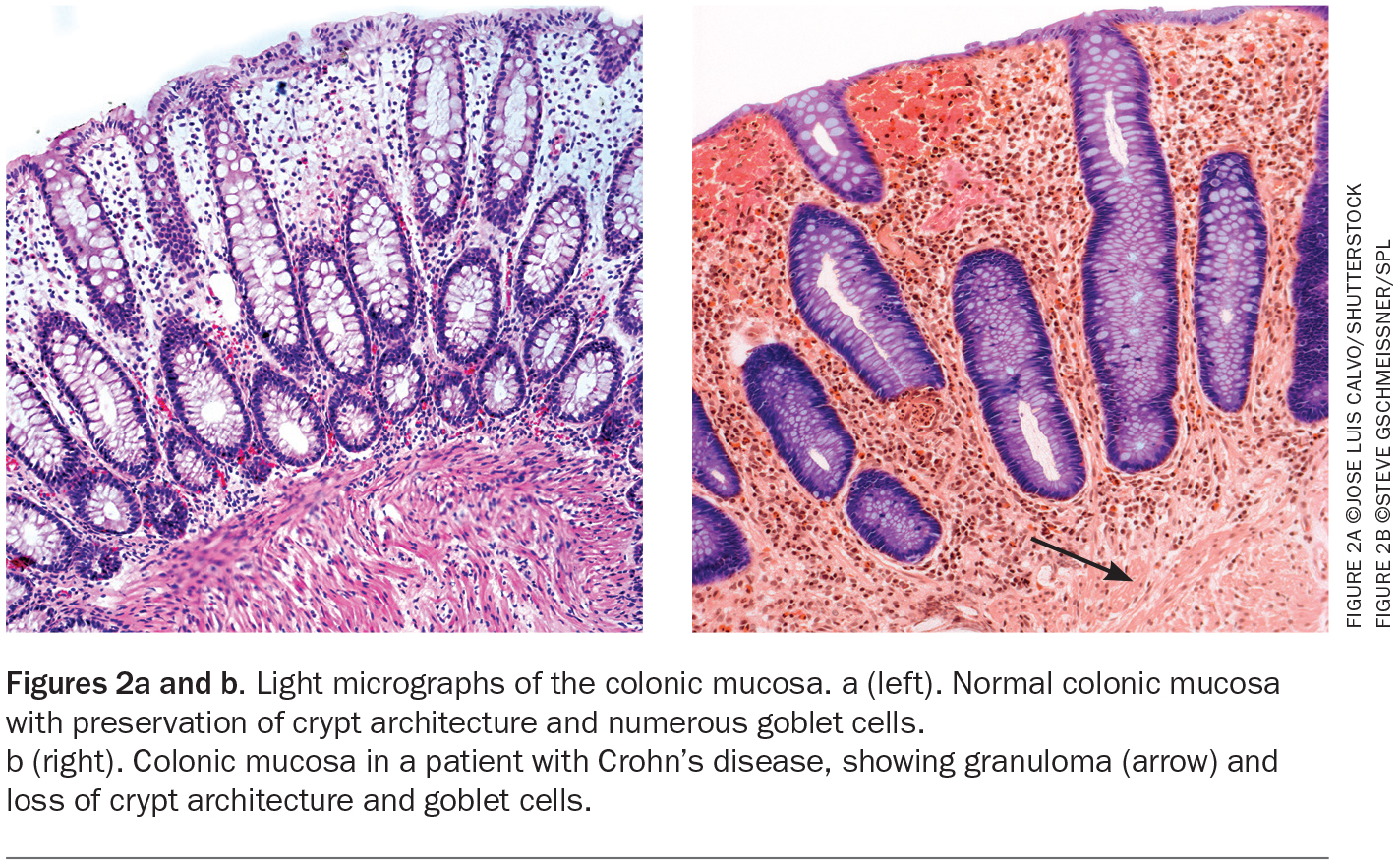
Given the chronic nature of IBD and its psychological and financial impacts, it is important to ensure the correct diagnosis is established.4,5 Regrettably, there is no single test that diagnoses IBD. Diagnosis is based on a combined approach of clinical history, biomarkers, endoscopic, radiological and histological assessment (Figures 1a and b; Figures 2a and b).
{kind=link}
{kind=link}
Symptom patterns are helpful but nonspecific. IBD presents with gradual onset of abdominal pain, diarrhoea and rectal bleeding with only a small percentage of patients presenting with acute severe colitis.2 Family history is a significant risk factor to consider, as patients with a first degree relative with IBD have a fivefold increased risk of developing IBD.6 However, despite this, the absolute risk remains low within the general population, with less than 10% of patients with IBD having disease heritability explained by genetic influence.7
Laboratory markers are essential for diagnostic and differential diagnostic purposes, as well as global management of IBD, but lack specificity. C-reactive protein has been studied in IBD as an objective marker of inflammation and correlates with disease activity. Other markers such as erythrocyte sedimentation rate, leucocyte and platelet counts and serum albumin level are also useful but comparably less studied in IBD.8 Special serological tests for anti-Saccharomyces cerevisiae antibody (ASCA) and atypical perinuclear antineutrophil cytoplasmic antibodies (p-ANCA) have been used to differentiate subtypes of IBD, but their routine use in establishing a diagnosis is not recommended.9 Similarly, faecal calprotectin testing is highly sensitive in differentiating IBS from IBD, but its role in inflammatory colitides is limited as they all lead to neutrophil influx through the bowel wall and into the gut lumen that elevates faecal calprotectin level.10
Despite IBD being predominantly a disease of younger people, there is a 20 to 25% incidence rate of new-onset IBD in the elderly.11 Along with other age-related comorbidities, elderly people are also more susceptible to other forms of ileocolitis, such ischaemic colitis or the segmental colitis associated with diverticulosis.
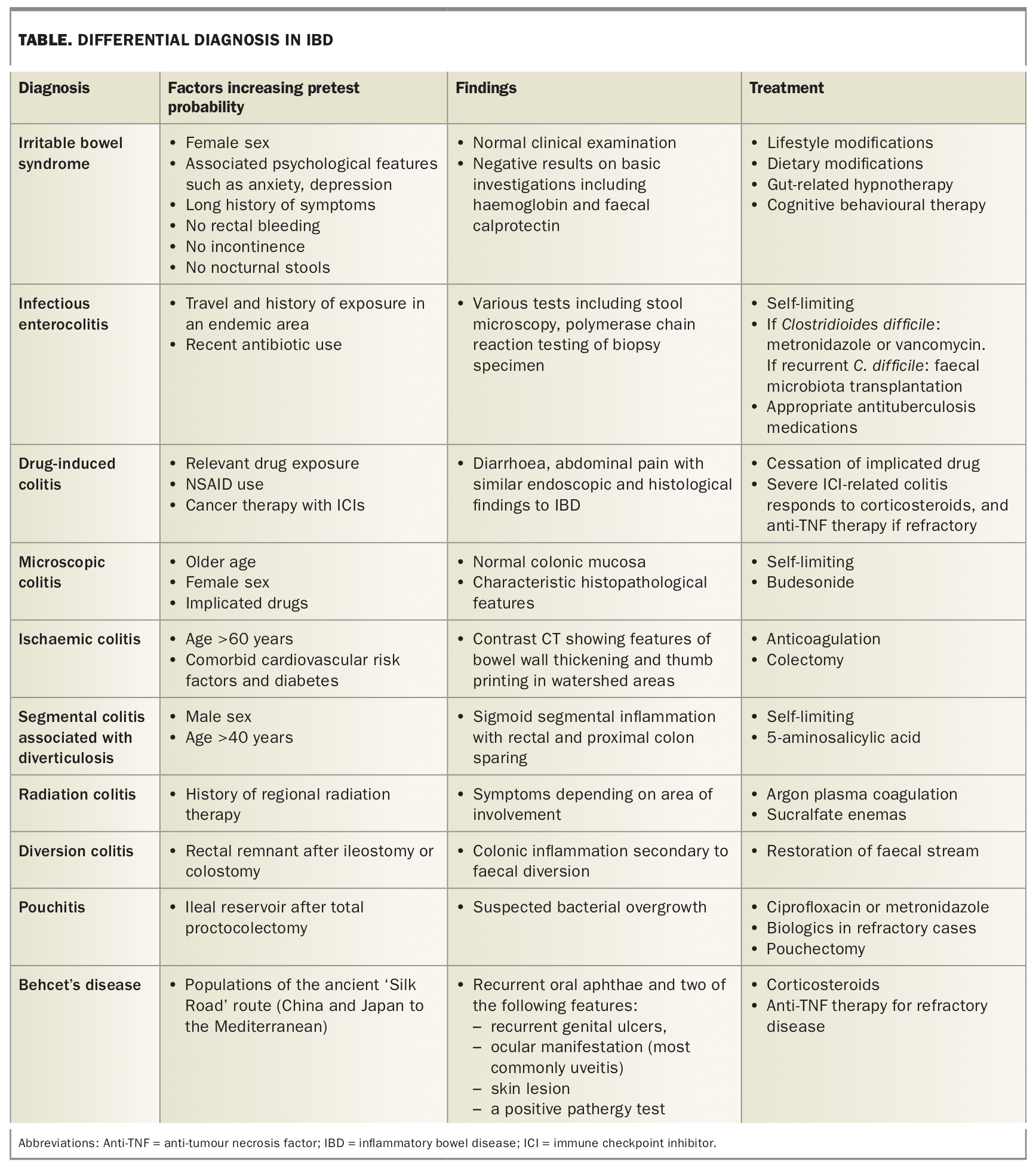
With increasing use of immunotherapy in cancer patients, there is an increasing burden of immune-related adverse events, particularly colitis, which needs to be considered in the differential diagnosis for IBD. Some common conditions that mimic IBD and need to be considered in appropriate settings as potential differential diagnoses are described below and summarised in the Table.
{kind=link}
Differential diagnoses for inflammatory bowel disease
Irritable bowel syndrome
IBS is a chronic relapsing disorder of the gut that causes cardinal symptoms of abdominal pain or discomfort associated with a change in bowel habit. It is an important differential diagnosis in the community setting and its prevalence exceeds that of other relevant differential diagnoses for IBD. Reassuringly, IBS no longer needs to be approached as a diagnosis of exclusion, and in most instances a structured clinical history (notably, symptoms continuing for more than six months) and physical examination can lead to a safe and reliable IBS diagnosis without further testing.1,12
Helpful resources for GPs that are designed to empower accurate diagnosis are available online. These include Choosing Wisely Australia, an initiative of NPS MedicineWise (www.choosingwisely.org.au), and the Gastroenterological Society of Australia’s guides to IBS for GPs (www.IBS4GPs.com), which is a web tool that demystifies some of the common misconceptions around the diagnostic work up of patients with IBS and provides various management principles that can be effectively employed for symptom management.
Infectious enterocolitis
Various gastrointestinal infections can mimic IBD. Infectious enteritis caused by fungal (Coccidiodes and Histoplasma spp.), bacterial (Clostridioides [previously ‘Clostridium’] difficile, Escherichia coli, and Yersinia, Salmonella, Shigella, Campylobacter and Aeromonas spp.), protozoal (Entamoeba histolytica) and parasitic (Strongyloides) infections can cause diarrhoea, abdominal pain and fever that may mimic IBD, although the time course is shorter, with an abrupt onset (within days, compared with weeks and months for IBD). Iron deficiency, common in IBD, is rare in patients with infectious colitis; nonetheless, infectious aetiology needs to be considered in the relevant clinical setting and excluded on stool microscopy and culture before diagnosis of IBD.13
C. difficile infection is important to consider as it is becoming increasingly common among patients with IBD.14 Furthermore, patients with IBD are more susceptible to recurrent episodes compared with the general population.15 Prompt diagnosis and treatment is important, with vancomycin being the preferred agent compared with metronidazole in patients with IBD.13 Faecal microbiota transplantation is reserved for patients with refractory disease and has excellent response rates.16
Infectious enteritis and, notably, tuberculous enteritis can be difficult to differentiate from IBD. The interferon-gamma release assay is clinically useful for differentiation, although it lacks sensitivity (67%).17 Diagnostic accuracy can be increased from 67 to 95% by combining CT features and endoscopic findings. Segmental small bowel involvement and mesenteric vascular stranding (the ‘comb sign’) are highly predictive of Crohn’s disease, as opposed to necrotic mesenteric lymph adenopathy and focal ileocaecal lesions, which are more common in intestinal tuberculosis (TB).18 A validated web-based Bayesian model that incorporates all significant findings has 92% accuracy in estimating the probability of intestinal TB compared with Crohn’s disease.19 Treatment of tuberculous enteritis usually involves quadruple therapy, as for pulmonary TB, for a minimum period of six to nine months.20
Drug-induced colitis
NSAIDs are notorious for causing ulceration within the gastrointestinal tract. Long-term use can lead to complications of stricture formation (the pathognomonic ‘diaphragmatic’ strictures), with features similar to those of Crohn’s disease.21,22
Advancements in cancer immunotherapy have also come at the cost of some well-recognised complications, in particular, immune checkpoint inhibitor-induced colitis. This condition occurs in 20 to 50% of patients being treated with immune-based chemotherapeutic agents such as ipilimumab and has similar endoscopic and histological features to IBD.23 Resolution usually occurs with cessation of the drug, but in severe cases that are refractory to corticosteroids, anti-tumour necrosis factor therapy or antileucocyte trafficking agents have also been used.24,25
Microscopic colitis
Microscopic colitis is characterised by nonbloody watery diarrhoea and has two distinct histological subtypes, lymphocytic colitis and collagenous colitis. Diagnosis, as suggested by the name, is made on histological assessment of the colon, which appears normal on endoscopic examination. The condition has a preponderance in women with a mean age of 65 years. Risk factors include smoking and taking multiple drugs. Proton pump inhibitors and anti-inflammatory agents confer the greatest risk.26 Treatment with budesonide has been shown to be effective in multiple randomised trials, although there is a substantial risk of relapse.27 Microscopic colitis runs a benign course with no complications in the longer term.
Ischaemic colitis
Ischaemic colitis predominantly affects older people (around 90% of cases are in adults over the age of 60 years) but can also be seen in younger patients.28 It usually presents with an abrupt onset of symptoms including abdominal pain and rectal bleeding; however, some patients may present with chronic symptoms.29 Recommended investigations for confirming a diagnosis are a contrast CT scan, looking for features of bowel wall thickening and thumb printing in watershed areas such as the splenic flexure and rectosigmoid region, followed by early colonoscopy within 48 hours of presentation.30 In most instances the episode is transient, but the condition overall carries a high mortality rate;31 therefore, in the appropriate setting a quick search for potential risk factors (i.e. comorbid cardiovascular disease and diabetes) should be considered and the diagnosis of colonic ischaemia suspected.30
Segmental colitis associated with diverticulosis
Chronic mucosal inflammation associated with diverticular disease can often become difficult to differentiate from IBD as histopathological and endoscopic features are fairly similar and occasionally nonspecific.32 Characteristically, segmental colitis associated with diverticulosis is a self-limiting condition, predominantly affecting men over the age of 40 years and, unlike IBD, infrequently requires medical treatment with oral 5-aminosalicylates.33 Rectal sparing with segmental colitis predominantly affecting the sigmoid colon are typical features.33
Radiation colitis
A history of regional radiation therapy usually predates the onset of rectal bleeding as a symptom of radiation colitis by six months to five years.34 Symptoms depend on the site and extent of gastrointestinal involvement and vary from abdominal pain or diarrhoea to rectal bleeding. Radiation proctitis from prostate cancer treatment is the only commonly occurring form of this condition, and even this appears to be less common now than previously. Endoscopic treatment with argon plasma coagulation has shown promise in the short term, with good evidence to support use of sucralfate enemas; however, refractory disease can be difficult to manage because surgical options may be limited due to extensive fibrosis as a consequence of previous therapy.35
Diversion colitis
This atypical colitis occurs in the rectal remnant of patients after ileostomy or colostomy, when a mucous fistula or Hartmann’s pouch has been left.36 The colonic inflammation results from diversion of the faecal stream from the colorectal mucosa.37 This relates to the colonic mucosa being devoid of short chain fatty acids, which are the preferred energy source for colonocytes.38 In normal circumstances, short chain fatty acids are derived from the breakdown of complex carbohydrates by resident bacteria.37 Lymphoid follicular hyperplasia is considered the hallmark histopathological feature of diversion colitis.39 Patients may be asymptomatic or may present with rectal bleeding. Restoration of faecal continuity leads to resolution and is often the treatment of choice.40 Such patients should ideally be cared for in IBD expert centres when possible.
Pouchitis
In patients with pouchitis, inflammation occurs in the ileal reservoir after total proctocolectomy for ulcerative colitis or other reasons.38 The aetiology is unclear, but bacterial overgrowth is suspected and hence treatment usually involves a course of oral antibiotics (ciprofloxacin shows better response rates than metronidazole).41 Cumulative incidence rates after ileal pouch-anal anastomosis formation vary from 20 to 40% by five years. Refractory disease not responding to antibiotics may respond to further immunosuppression with biologics, or ultimately may require pouchectomy.
Behcet’s disease
Populations of countries along the ancient ‘Silk Road’ route (Japan and China to the Mediterranean) have a predisposition to this primary vasculitis that is diagnosed based on clinical findings of recurrent oral aphthae and two of the following features: recurrent genital ulcers, ocular manifestation (most commonly uveitis), skin lesion or a positive pathergy test.42 Gastrointestinal manifestations are similar to Crohn’s disease; however, the ‘punched-out’ ulcers seen in the ileocaecal region usually suggest Behcet’s disease. Typically, the bordering tissue is not inflamed, which helps support the diagnosis.43 Therapeutic off-label options in steroid-refractory disease include anti-tumour necrosis factor therapy for induction and maintenance of remission.44
Conclusion
Multiple conditions lead to clinical, endoscopic and histological features that are similar to those seen in patients with IBD. Risk factor assessment, age at presentation and the time course of symptomatology are all important aspects for consideration in making a diagnosis. Reviewing potential differential diagnoses as presented here should guide the search for the underlying cause. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.