Autism spectrum disorder in general practice

Autism spectrum disorder (ASD) is a chronic condition typically diagnosed in early childhood. A multidisciplinary approach to management and an evolving treatment plan are essential for successful long-term patient outcomes. Early diagnosis, referral and intervention are key to management of children with ASD and GPs play an important role in co-ordinating care across their lifespan.
- Autism spectrum disorder (ASD) is characterised by deficits in social communication and the presence of restricted, repetitive or stereotyped behaviours.
- Presentations are diverse.
- Comorbidities are common and occur in over 70% of children with ASD.
- Early referral to a paediatric specialist for diagnosis is important, but diagnostic assessment need not delay commencement of intervention.
- GPs can facilitate referral of children with ASD to specialists and allied health professionals for early interventions including speech and occupational therapists, psychologists and audiologists.
- Medications may play a role in managing comorbid psychiatric and medical issues.
- GPs have an important role in early identification, ongoing management and care co-ordination of children with ASD, and are uniquely placed to monitor the wellbeing of carers.
- Referral to the local National Disability Insurance Scheme Early Childhood Early Intervention partner should be made for every child under 7 years of age who presents with developmental concerns, and can be made before specialist diagnostic assessment.
Autism spectrum disorder (ASD) is a common neurodevelopmental disorder characterised by social and communication impairment and restricted or repetitive behaviours, with a prevalence of approximately 1% internationally.1 In this article, we provide an overview of ASD management for clinicians in primary care, with a focus on early identification and early instigation of intervention.
Diagnostic criteria
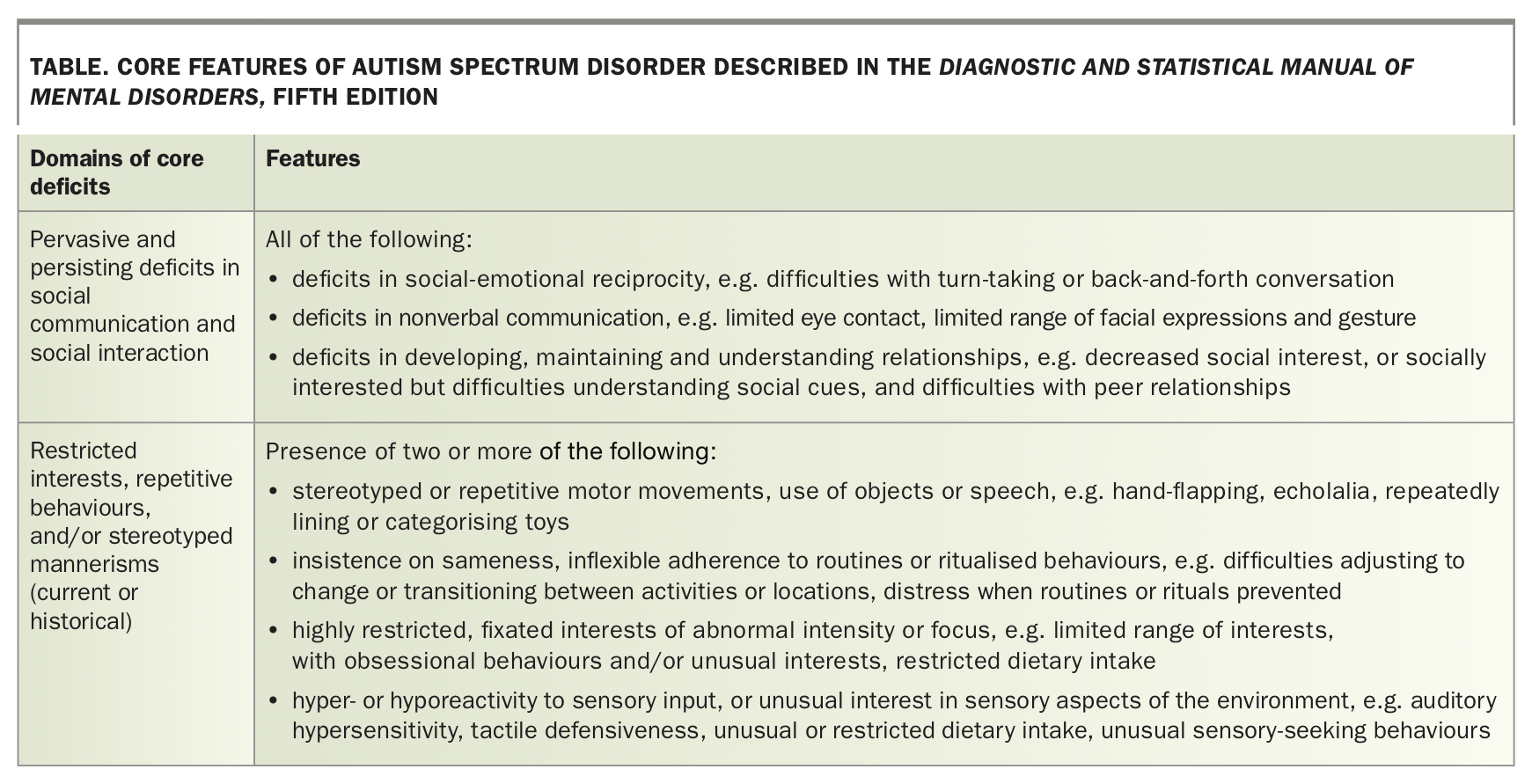
In Australia, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for ASD are used for diagnosis.2 Published in 2013, DSM-5 consolidated the previous nomenclature of pervasive developmental disorders (PDD) (autistic disorder, Asperger's disorder, PDD-NOS [not otherwise specified] and childhood disintegrative disorder) into a single diagnosis of ASD with modifiers (e.g. with or without intellectual disability or language impairment). It also permits diagnosis of co-occurring conditions such as attention deficit hyperactivity disorder (ADHD) and anxiety. DSM-5 also introduced three severity levels to describe support needs within the two domains of core deficits: social communication; and restricted, repetitive or stereotyped behaviours (Table 1).
{kind=link}
Epidemiology
Internationally, the prevalence of ASD is around 1%, but is on the rise, with the latest US estimate of prevalence in 2020 at one in 54.3,4 Recent studies suggest that Australia has one of the highest prevalences of ASD in the world.5 The rise in prevalence over decades is thought to reflect increased diagnosis of mild ASD presentations, increased awareness of ASD symptoms in the community and increased availability of early intervention and school-based support for children with ASD symptoms. Changes to diagnostic criteria and substitution of previous diagnoses for the term ‘ASD’ may also be contributing factors. However, some of the rise may be attributed to a true increase in prevalence over time.6 Males are diagnosed with ASD three to four times more often than females, although there is increasing evidence to suggest that ASD is under-recognised in females.1
Differential diagnoses
During diagnostic assessment for ASD, several alternative possible diagnoses should be considered, including isolated language delay, social (pragmatic) communication disorder and global developmental delay or intellectual disability. Social (pragmatic) communication disorder is a DSM-5 diagnosis used to describe children with social communication deficits, in the absence of restricted, repetitive or stereotyped behaviours. Preschool-aged children who meet DSM-5 diagnostic criteria for ASD in addition to delays in two or more domains of development (gross motor, fine motor, speech and language, social-emotional or cognitive domains) are described as having comorbid global developmental delay. This is a placeholder diagnosis used in young children before formal psychometric testing is performed. Psychometric testing is often first performed in the year before to school entry by a qualified psychologist, and is used to determine a child’s full-scale intelligence quotient (IQ) and their cognitive abilities across a number of domains. The diagnosis of intellectual disability infers an overall IQ of 70 or less, with associated impairments in adaptive functioning.
Aetiology
Autism was first described by Leo Kanner and Hans Asperger in the 1940s, and was later endorsed in the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III) in 1980.7 Diagnostic criteria based on behavioural presentations have evolved over time, but the diagnosis continues to be associated with a diverse range of phenotypic presentations. The broad diversity in ASD presentations are underpinned by heterogeneous pathways of causation that remain poorly understood.
At the neurobiological level, emerging evidence suggests that ASD is associated with atypical organisation of neuronal circuitry and connectivity. ASD is primarily regarded as a genetic disorder, although environmental exposures may play a role in unmasking genetic predisposition. Specific genetic syndromes, such as Fragile X or tuberous sclerosis complex, are identified in a minority of cases. However, in many cases, a range of common and rare copy number variants are believed to culminate in ASD in an additive fashion.8 Genomic copy number variants are typically inherited, but occur de novo in at least 5% of cases.7 To date, genes implicated in ASD risk appear to influence neuronal function and regulation of gene expression.1
A number of environmental risk factors are associated with ASD, including advanced maternal age (≥ 40 years), advanced paternal age (≥ 50 years), short interpregnancy interval (< 24 months), prematurity, low birth weight and various prenatal factors associated with a nonoptimal antenatal environment. For example, prenatal exposure to valproic acid is associated with risk of ASD in offspring. Maternal antenatal antidepressant use has not conferred ASD risk in well-controlled studies, and no consistent risk associated with caesarean section or assisted conception has been identified.1 Furthermore, we can confidently reassure families that historical misconceptions about a link between ASD and childhood vaccination have been disproven.6
Natural history and prognosis
A diverse range of developmental trajectories is associated with ASD and, although functional needs vary over time, overall diagnostic stability is high. At the population level, the greatest outcomes into adulthood are generally seen in children with ASD who have age-appropriate language skills by 3 years of age.6 Families are encouraged to celebrate developmental gains and progress irrespective of developmental stage, to alleviate stress in relation to long-term outcomes.
Early identification in primary health care
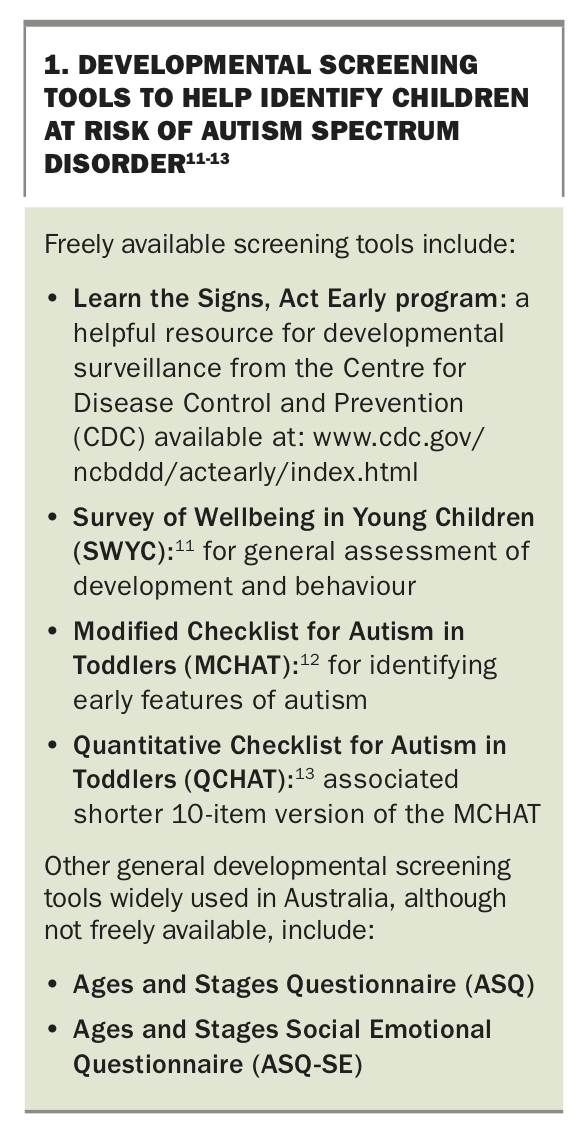
Increased efforts to improve the identification of ASD over the past decade have been due to the realisation that ASD is more common than previously thought and the emergence of good evidence that early identification and intervention can improve outcomes for children and families. Evidence from longitudinal studies indicate that participation in early intervention (between the ages of 2 and 3 years) predicts superior outcomes in relation to IQ, education, employment and adaptive functioning in adults with varying cognitive abilities. It also increases the probability of living independently in adulthood for individuals without comorbid intellectual disability.1,9 Nevertheless, early identification of ASD in the educational and medical sectors is still largely opportunistic rather than systematic. Although ASD can be diagnosed in children younger than 2 years old, the average age of diagnosis in Australia is 4 years.10 Clinicians should heed developmental concerns expressed by parents, and routine monitoring for development and ASD symptoms in toddlers and young children is encouraged. Developmental screening tools for ASD are summarised in Box 1.11-13 Almost all children identified as at risk on these screening tools have developmental difficulties and will benefit from further assessment and early intervention, although not all will have ASD specifically.
{kind=link}
We recommend that parental concern and clinical judgment prompt referral to an allied health specialist and/or a paediatrician, particularly in vulnerable populations. To facilitate early access to intervention, GPs can initiate referrals to their local partnering National Disability Insurance Scheme (NDIS) Early Childhood Early Intervention provider (which vary across geographical locations). This referral can be made before a diagnostic assessment with a specialist on the basis of developmental concerns alone, to facilitate early access to intervention and funding.
Diagnosis
In Australia, the Autism Cooperative Research Centre (CRC) recently produced the National Guideline for the Assessment and Diagnosis of Autism Spectrum Disorders.14 This guideline was published in 2018 and has been endorsed by the National Health and Medical Research Council (NHMRC). It describes a standard approach to ASD diagnosis in keeping with evidence-based best practice, and emphasises the importance of equitable access for all (Flowchart). Trained professionals with neurodevelopmental experience should conduct diagnostic assessments for ASD. Practically speaking, the diagnosis of ASD is made on the basis of criteria described in the DSM-5 (or in the International Classification of Diseases 11th Revision, ICD-11).
Referrals for developmental assessment are initiated by primary healthcare physicians to a general paediatrician, developmental paediatrician, or team, who are tasked with collating documentation from previous treating physicians, school records and allied health therapists, to assist in the initial appointment. The focus of this visit is to identify the need for immediate referral to relevant support and intervention services (irrespective of presumptive diagnosis), and to determine the need for a diagnostic evaluation. A Single Clinician Diagnostic Evaluation will result in one of three possible outcomes. In the first two instances, the clinician will conclude with high confidence that a child either does or does not meet diagnostic criteria for ASD or another clinical diagnosis. In the third instance, where high diagnostic confidence is not possible, arrangement of a multidisciplinary Consensus Team Diagnostic Evaluation should follow.
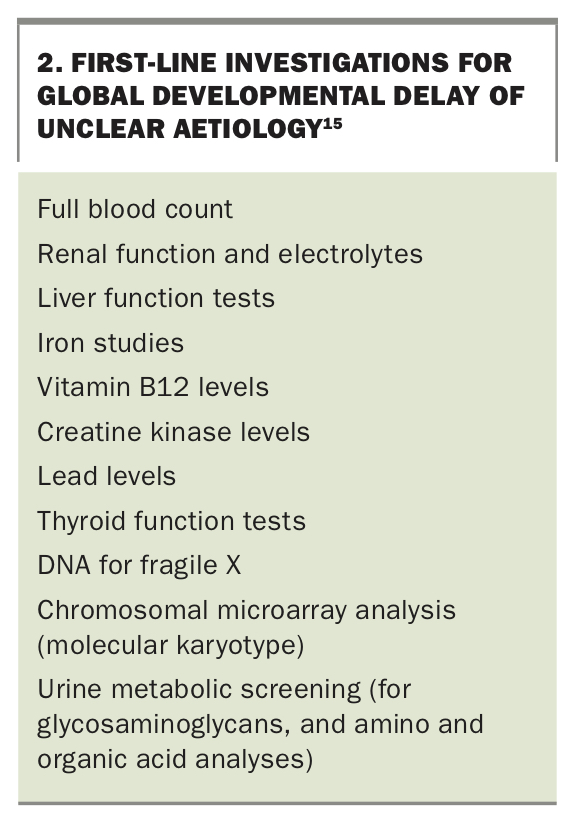
A number of blood and urine investigations are typically ordered when children present with ASD, global developmental delay or intellectual disability, as shown in Box 2.15 Additional medical investigations may also be indicated in some cases – for example, EEG in the context of language regression or suspected seizures.
{kind=link}
Local referral processes and resources – health pathways
Information regarding local referral processes, local services and other resources are available via primary healthcare network-specific HealthPathways. For example, the Autism HealthPathways Initiative developed nine new pathways related to autism, intellectual disability and developmental delay, in a collaborative project between the Autism CRC and Mackay Health.
Telehealth
Telehealth (involving high quality video- conferencing) has utility in providing access to care for individuals with ASD and their families who live in remote and rural locations. Although limited, there is evidence to suggest that web-based developmental surveillance programs are acceptable and efficient.16 Further, several studies have reported on the high level of agreement between ASD assessment protocols conducted via video compared with gold standard, in-person assessments.17,18 A novel telehealth Naturalistic Observation Diagnostic Assessment (NODA) consisting of a brief online developmental history followed by clinically-guided in-home video recordings capturing different scenarios of the child’s day-to-day interactions and problem behaviours has also been developed and reported to have high diagnostic agreement with in-person assessment.19
Although the suitability of telehealth alone for diagnostic assessment is limited, it provides a useful tool for triage, ongoing review, and education and training for caregivers and healthcare providers.20 Further, for those families in geographically distant communities and during times such as the COVID-19 pandemic, telehealth options can be the first step in the assessment process (such as the Watch Me Grow Developmental Check available online at: https://is.gd/wmgdevcheck), and can facilitate access to timely supports (e.g. through the NDIS) so that intervention can start without delay.21
Ongoing management after ASD diagnosis
ASD is a chronic condition and primary healthcare providers are key to providing care co-ordination across the patient's lifespan. Several resources for long-term management of patients are available to GPs through the HealthPathways. Therapeutic priorities evolve over time and GPs may identify when a child’s therapy regimen requires reconsideration. Children usually benefit from a combination of therapies and a multidisciplinary approach, and often need different therapies or therapy combinations at different stages of their development.
Interventions for ASD
The aims of intervention are to maximise functional independence by facilitating acquisition of adaptive skills, and minimise challenging behaviours that may interfere with quality of life. This includes facilitating general development and learning, promoting socialisation, reducing maladaptive behaviours and educating and supporting families to accomplish these goals. The most common interventions for children with ASD include the following.
- Enrolment in a high-quality daycare or preschool program with inclusion support – to provide a structured environment for children with ASD to learn and interact with other children their age
- Speech therapy – to assist with language skills, social communication skills, and in some cases with restricted dietary intake
- Occupational therapy – to assist with development of play, self-help, social and motor skills where indicated; may also assist in addressing challenging behaviours of a sensory nature
- Psychological therapy – to assist children with ASD with relationship building, strategies to recognise and cope with challenging emotions and optimisation of mental health
Some multidisciplinary early behavioural intervention specialists may deliver specific autism interventions, such as applied behavioural analysis (ABA), Early Start Denver Model (ESDM) behavioural therapy, the Treatment and Education of Autistic and Related Communications Handicapped Children (TEACCH) program and a parent-mediated video-aided intervention (iBASIS-VIPP), whereas others combine strategies from a range of these modalities, based on the individual needs of the child.
Funding for ASD
A number of funding sources are available to children with ASD including the NDIS, the Better Access to Mental Health Care (Medicare) Plan, the Chronic Disease Management (Medicare) Plan and the Carer’s Allowance. At the time of publication, item numbers 135 (paediatrician) or 289 (psychiatrist) in the Medicare Benefits Scheme can be billed following a diagnosis of ASD. Under the scheme, an initial referral to a paediatrician or psychiatrist can be given by the GP and following the assessment, the paediatrician or psychiatrist, for the purpose of diagnosis in collaboration, can provide referrals to up to another four professionals including audiologists, occupational therapists, optometrists, orthoptists, physiotherapists, psychologists and speech pathologists.
The previously accessible Helping Children With Autism (HCWA) program, which was a nonrenewable funding package providing subsidised access to 20 sessions of any allied health therapy, closed on 30 June 2020. For children with existing HCWA plans, the funding will remain available until 31 March 2021. However, no new HCWA plans will be available for newly diagnosed children. Rather, the pathway to support now involves initiating a referral to local partnering NDIS Early Childhood Early Intervention providers (which vary across geographical locations). This referral can be initiated by anyone (parents, allied health providers or clinicians) who has developmental concerns for a child under the age of 7 years, and can be made before an assessment with a specialist to facilitate early access to intervention and funding.
Educational considerations
Children with ASD may be eligible for additional assistance in the school setting. Many individuals with ASD are educated in mainstream classes, although some benefit from autism-specific learning environments. Those with co-occurring moderate-to-severe intellectual disability may benefit from attending schools for specific purpose (SSPs).
Alternative therapies
Alternative interventions for ASD include a broad range of treatments that are not often used in the mainstream medical system because they are not currently supported by scientific evidence. There is no evidence to support the use of therapies such as secretin, elimination diets and yeast overgrowth management, and there are significant risks associated with some treatments, including chelation therapy, or from withholding the measles-mumps-rubella vaccine.
For treatments that are unlikely to cause health-related harm, a nonjudgmental approach to counselling families is suggested. Where treatments are expensive, time-consuming or impacting on engagement in evidence-based therapies, GPs can assist in counselling families on the effects of these. A good resource for GPs and families that summarises the evidence base for a broad range of mainstream and alternative therapies for ASD can be accessed on the Raising Children Network website (https://raisingchildren.net.au/autism/therapies-guide).
Management of co-occurring conditions in primary healthcare settings
Co-occurring medical conditions are common in children with ASD and can significantly affect child and family functioning.6 Primary healthcare physicians play a vital role in the identification and clinical management of these co-occurring conditions.
Psychiatric comorbidities and mental health issues
Psychiatric comorbidities and mental health issues are common in ASD and may include anxiety, obsessive-compulsive behaviours, depression, self-harm and aggression. GPs are encouraged to consider paediatric re-referral or psychiatric referral should these concerns emerge. Management of complex presentations may involve the use of psychotropic medications as adjuncts to behavioural intervention.
Learning difficulties and ADHD
Concerns regarding academic progress or attentional difficulties in a child with ASD warrant referral to the school counsellor, if available, and a paediatrician. Stimulants remain the first-line pharmacological treatment for ADHD in children with ASD, although response can be variable.
Gastrointestinal problems
Children and young people with ASD have higher rates of gastro-oesophageal reflux disease (GORD) and constipation than the general population, and optimisation of gastrointestinal (GI) health can have a profound impact on quality of life. Minimally verbal individuals may be unable to report specific GI symptoms, and can instead present with agitation, sleep disturbance and behavioural disturbance associated with GI discomfort. A high degree of suspicion for GI issues is advised, as is the early institution of a stool softener and paediatric referral.
Dietary issues
Many children with ASD have restricted dietary intake to varying degrees, associated in some cases with sensory aversions based on food colour, texture or temperature, and/or with rituals around food presentation or compulsive eating of arbitrary foods. Children with restricted dietary intake require monitoring for nutritional deficiencies. The management of restricted dietary intake can be complex, and multidisciplinary input from dieticians, speech pathologists, occupational therapists and behavioural therapists with experience in ASD is recommended.
Sleep and allergy
Sleep disturbances, especially difficulties with initiation and maintenance of sleep, are very common in children and young people with ASD. These difficulties may exacerbate problematic daytime behaviour and affect learning. Optimisation of sleep can therefore have a profound impact on quality of life for children with ASD. Early identification of difficulties with sleep onset, sleep maintenance and snoring are vital. Short-term use of melatonin can be considered, if used in conjunction with improvements to the sleep routine and paediatric referral. For children who snore regularly or have allergic sinusitis or hayfever, a short-term course of inhaled nasal corticosteroids and referral to and ENT and/or a sleep specialist are recommended.
Seizures
Children and young people with ASD have a higher prevalence of seizures than the general population, particularly those with associated intellectual disability. Screening EEGs are not recommended for patients who are asymptomatic. An EEG and referral to a paediatrician and/or paediatric neurologist should be considered for patients with suspected seizures or significant regression of language.
Dental health
Children and young people with ASD often have unmet dental health needs due to difficulties in maintaining regular dental hygiene and co-operating at dental visits. Families should be encouraged to see a child-friendly dentist from the age of teeth eruption for anticipatory guidance, and to desensitise the child to routine dental care. In complex cases, referral to a dental hospital for care by a specialist paediatric dentist may be required. Language delays in children with ASD may lead to delayed presentation if they have dental infections, and they may present instead with agitation, sleep disturbance or behavioural disturbance.
Carer wellbeing
Caring for a child with a chronic condition is challenging, and the health needs and wellbeing of carers may be overshadowed by these challenges at times. Primary care physicians are vital in providing whole-of-family care, and are encouraged to routinely screen for concerns regarding the physical and emotional wellbeing of carers of children with ASD.
Transition to adult services
Although the management of ASD in adulthood is beyond the scope of this article, we acknowledge that primary healthcare physicians are the main medical providers of care for adults with ASD. Referrals to rehabilitation specialists and psychiatrists may be helpful for complex cases.
The future of ASD
Researchers and clinicians are aware that a ‘one size fits all’ approach to ASD management is suboptimal, particularly in light of the vast heterogeneity in presentations in this condition. Current research efforts are seeking to inform personalised treatment recommendations by identifying subgroups of individuals based on behavioural, psychometric and biological data and treatment response. In the future, more specific subclassification of individuals with ASD may be possible, with more nuanced treatment recommendations and prognostic prediction as a result.22
As genetic research evolves, it is likely that the genetic basis of ASD will be further delineated over time. There is increasing interest in next generation sequencing including whole exome sequencing (which examines all nucleotides that code for proteins in an individual’s DNA) and whole genome sequencing (which assesses for variation in any part of the genome, both in coding and noncoding regions). Some clinicians in North America and Europe already request next generation sequencing for children with ASD without an abnormality on chromosomal microarray, and such testing may become routine in time.
Whole exome sequencing is now available in Australia through the PBS for some children with moderate to severe intellectual disability. The identification of specific genetic abnormalities is of some clinical utility, in that it can inform family planning decisions, guide prognostication and connect family with specific support groups in some cases. In time, identification of specific genetic diagnoses and/or underlying neurobiology in ASD may guide treatment recommendations and permit the development of pharmacological adjuncts to behavioural intervention. Advances of this nature are anticipated in the coming decade.1
Conclusion
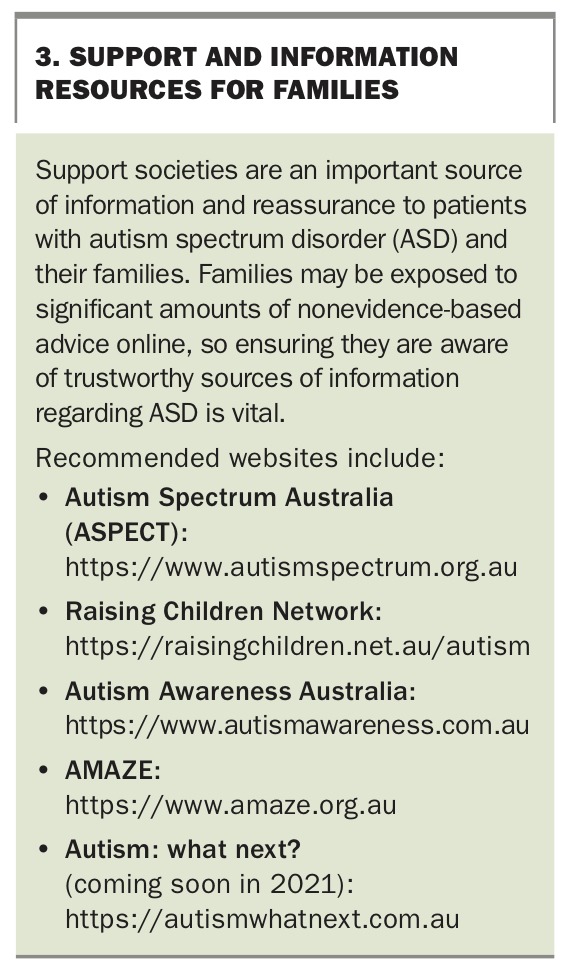
GPs have a vital role in developmental surveillance and identification of developmental concerns in children. Swift referral to early intervention therapies is key. Vision and hearing screening are first-line investigations. Early diagnostic referral is recommended, but need not precede referral for intervention from speech and language therapists, occupational therapists, and psychologists. Monitoring and management of co-occurring conditions after diagnosis is crucial for achieving optimal outcomes in ASD. GPs have an ongoing relationship with families, and are invaluable in monitoring carer wellbeing over time. The process of exploring and addressing developmental concerns in childhood is an emotional experience for parents and families. GPs play an important role in guiding families on this journey and in providing holistic care for optimal outcomes across the life course. Useful ASD support societies and resources for families are listed in Box 3. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.