Zoonoses in Australia. Established and emerging risks

Zoonoses are an important group of infections transmissible between animals and humans and the source for potential new and re-emerging diseases, some with pandemic potential.
- Zoonoses are an important group of infectious diseases that are transmissible between vertebrates and humans.
- Zoonoses are the source for new and re-emerging infectious diseases, some with pandemic potential, and their control requires a ‘one health’ approach.
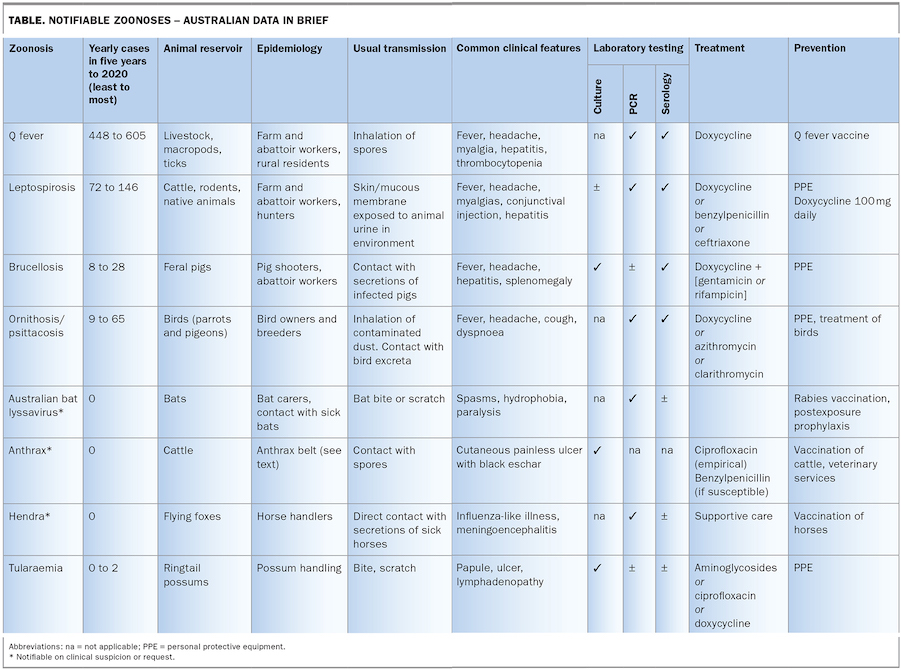
- Q fever is the most common classic zoonosis in Australia today (excluding foodborne zoonoses).
- Q fever, with its protean manifestations, should be considered in the differential diagnosis in patients from rural NSW and Queensland even where there is no direct animal contact.
- Improved diagnostics incorporating molecular techniques (polymerase chain reaction tests) have enhanced the detection of these pathogens, particularly for Q fever and leptospirosis.
- The foodborne pathogens Salmonella and Campylobacter, also have significant health and productivity impacts.
Zoonoses are common. This is unsurprising when you consider an estimated 60% of infectious diseases are attributable to pathogens shared between humans and other animals.1 A broad range of pathogens – viruses, bacteria, fungi and parasites ‒ are capable of zoonotic spread. Human population growth, global food chains, habitat destruction, climate change and travel all increase the contact points between humans and animals, leading to increased risk of disease transmission.
The recent emergence of severe acute respiratory distress syndrome coronavirus 2 (SARS-CoV-2) has brought these risks into sharper focus. SARS-CoV-2 is a member of the coronavirus family, of which four species were already common circulating human pathogens. Many other coronaviruses are found in mammals. This virus family has a particular ability to cross species boundaries, demonstrated by SARS-CoV-1 (SARS, 2003) and MERS-CoV (Middle East Respiratory Syndrome Coronavirus, 2013). Although the exact source of the current SARS-CoV-2 pandemic has not been established, genomic investigations have shown it to be closely related to viruses found in bats.2 Increasing human and animal interactions raise the risk of such viruses crossing into humans, with potential for subsequent outbreaks.
The effect of SARs-CoV-2 is not limited to humans. Infection has spread from humans to other mammals, with documented spread to a variety of species, including dogs, tigers, cats, lions, monkeys, hamsters, ferrets and mink. In some cases, this has resulted in animal deaths.3 This highlights the risks to both human and animal health and the importance of a ‘one health’ approach, by which professionals from human, animal and environmental health disciplines collaborate with the goal of optimal overall health outcomes.
In Australia, eight classic zoonoses of particular consequence are nationally notifiable and are the subject of more detailed discussion in this article (Table). However, many of the common infectious diseases encountered in clinical practice (e.g. foodborne diseases such as salmonellosis, campylobacteriosis or giardiasis) may be transmitted by contact with animals. In addition, animals are a known vehicle for transmission of multidrug-resistant organisms, commonly acquired through ingestion of contaminated foods. GPs, as the first point of contact for many patients, need to be alert to the risk of zoonotic disease. This is not just to aid in diagnosis of common zoonoses, but to assist in early recognition of novel diseases.
{kind=link}
Common notifiable zoonoses in Australia
Q fever
Australia has a proud history of Q fever research. Queenslander Edward Derrick provided the first clinical description of a febrile illness among meat workers at the Cannon Hill abattoir on the Brisbane River in 1937. ‘Query’ fever, as he named it, did not occur in the only other abattoir in town where pregnant animals were not slaughtered, thus highlighting an important epidemiological feature, the concentration of the organism in the placenta (Figure 1). Sir Frank McFarlane Burnett further characterised the organism as an intracellular rickettsia-like bacteria later named Coxiella burnetii. South Australian Professor Barrie Marmion went on to develop a Q fever vaccine – the only human Q fever vaccine available in the world today.
{kind=link}
Australia has one of the highest global notification rates for Q fever, with 500 to 600 cases notified annually – most in Queensland and New South Wales (NSW). Epidemiological studies have identified risk groups beyond those traditionally recognised.4 Activities such as mowing lawns contaminated by wildlife reservoirs (such as macropods) pose potential risks even in semiurban environments. Small outbreaks have been identified in catteries and vet clinics. Although not well studied in Australia, environmental contamination depending on topography and wind characteristics may play a role in dissemination of hardy, infectious Coxiella spores over considerable distances.
Infection, which only requires a low infectious dose and occurs predominantly by inhalation, becomes apparent two to three weeks after exposure. Sixty percent of cases are asymptomatic. When present, symptoms may be mild to severe, presenting most commonly as pyrexia of unknown origin and hepatitis, with community-acquired pneumonia considered less common in Australia compared with Europe.5 The importance of Q fever lies in the development of Q fever fatigue syndrome in 20% of infected individuals and chronic focal infection in another 1 to 4%. In adults this is most commonly endocarditis, but also infected vascular grafts and aneurysms. In children, chronic recurrent focal osteomyelitis is increasingly being recognised. The latter in particular poses significant challenges in terms of understanding the pathogenesis and best treatment regimens. The clinical utility of routine echocardiography to detect undiagnosed cardiac valvulopathy (e.g. congenital bicuspid aortic valve or mitral valve prolapse) and initiate pre-emptive treatment remains controversial.
Test selection, as with most infections, is very dependent on time of collection in relation to symptom onset. Polymerase chain reaction (PCR) is most reliable in the first seven to 10 days (sensitivity, 80%) before development of an antibody response. The organism is generally not cultured as it is a laboratory hazard (although sending blood cultures to rule out other pathogens is not a risk). Methods of antibody detection include enzyme immunoassays, immunofluorescence assays and complement fixation tests.
Two different antigenic forms of Coxiella can be distinguished. The difference resides in the surface lipopolysaccharide of the organism. Antigenic variation is important for serological diagnosis and vaccine production. Phase 2 antibodies are found in high levels in acute Q fever, whereas high levels of phase 1 antibodies are found during persistent or chronic infection.6
Doxycycline is the mainstay of treatment of acute infection, and chronic infection requires combination therapy with hydroxychloroquine. Q fever vaccine was licensed in 1994 and introduced firstly to abattoir workers and later, through the Commonwealth-funded national Q fever vaccination program from 2001 through 2005, to the at-risk rural population. After an initial decrease in notifications, case numbers have continued to rise since 2009. There are several barriers to more widespread vaccination including cost and reactinogenicity (particularly in those with previous exposure). Consequently, prevaccination screening requiring both serological testing and intradermal skin testing is necessary but poses logistic challenges. The vaccine is not licensed for children under 15 years of age.7
Brucellosis
There are four classic zoonotic Brucella species. Australian cattle were declared free of Brucella abortus in 1989 after a very successful national brucellosis and tuberculosis eradication campaign. B. suis, however, is endemic in the feral pig populations in Queensland and northern NSW. A recently published NSW survey of feral pigs indicated 2.9% seropositivity.8 Each year, 10 to 30 human cases are reported in recreational and occupational hunters of feral pigs or feral pig abattoir workers.9 A more recent twist in the epidemiology has been the increasing reports of B.suis infecting pig dogs in the field resulting in small numbers of infected veterinarians.10 Each year, occasional brucellosis cases, usually B. melitensis, are diagnosed in travellers to endemic countries, especially those visiting friends and relatives, migrants and refugees and after ingestion of unpasteurised cheese and dairy products. B. canis is not endemic to Australia.
The clinical spectrum of illness ranges from prolonged fever with indolent onset, relapsing illness and chronic focal suppurative complications. Diagnosis of acute brucellosis relies on serological testing and blood cultures. Culture of the organism is a laboratory hazard, so it is prudent to notify the laboratory if brucellosis is suspected. In relapsing disease, blood cultures are more useful as serological tests are already positive. Blood cultures allow speciation of Brucella, which is not possible serologically. In focal suppurative infection, serological testing is less helpful. Most focal suppurative complications are confirmed based on typical granulomatous histopathology of involved tissue, often with calcification, molecular confirmation on tissue using PCR, and culture of the organism. Both genus- and species- specific Brucella PCR assays are available from public health reference laboratories and have most value when used on culture-negative tissues and for organism speciation. Imaging techniques (radiographs, ultrasound, CT, MRI and FDG- positron emission tomography with CT [PET-CT]) are also of value in localising focal disease. A characteristic sonographic, CT and MRI pattern of calcification in brucellomas has been described. New Brucella species, including B. pinnipediae and B. ceti have been isolated from marine hosts within the past few years. The zoonotic potential of these emerging new Brucella species is unknown.
Leptospirosis
Leptospires are spiral-shaped, motile bacteria that have a wide spectrum of hosts, including humans. Bacteria of the genus Leptospira can be separated into distinct serovars, each adapted to certain animal species that act as environmental reservoirs for the disease. In Australia, the most common serovars include hardjo (in cattle), arborea (in rats and mice), zanoni (in bandicoots and rats) and australis (in rats and small marsupials). Infected host animals can remain asymptomatically infected for years, excreting viable leptospires in the urine. Transmission occurs when there is contact between contaminated moist soil or surface water and broken skin or mucosal surfaces.
Although leptospirosis is generally rare in Australia, outbreaks can occur, especially in the context of high rainfall or flooding. The largest outbreak in Australia was recently reported in raspberry pickers from northern NSW, who likely acquired the disease through scratches on their hands during picking.11 Leptospirosis can also cause fever in returned travellers, with notable outbreaks associated with watersports such as rafting or adventure expeditions.
Symptoms usually manifest between five to 14 days after exposure, with fever, malaise, headaches and meningism being prominent symptoms of the initial bacteraemic phase. Hepatitis and thrombo- cytopenia are frequent, and conjunctival injection, although not always present, may be a helpful distinguishing feature.12 In up to 50% of untreated patients, the disease may evolve into an immune phase, in which there are few symptoms but excretion of leptospires in the urine occurs. Fever may return after this phase, with substantial complications including renal failure, pulmonary haemorrhage and acute respiratory distress syndrome.
Serological testing forms the mainstay of diagnosis, although PCR (on blood) can be useful, particularly in the acute phase when serology results may be negative (i.e. days 1 to 7 after symptom onset). Leptospires can be detected in urine for a longer duration than in blood, although bacterial contamination of the specimen type limits its application. Culture of leptospires is possible but requires specialised media, is time consuming and is generally limited to reference laboratories.
Treatment consists of either doxycycline, benzylpenicillin or ceftriaxone for five to seven days. Doxycycline is occasionally used as prophylaxis in high-risk settings.
Ornithosis
Chlamydophila psittaci, an obligate intracellular bacterium found in birds, can cause psittacosis (or ornithosis), a severe illness in humans. C. psittaci has a worldwide distribution, with parrots and pigeons being the most commonly infected birds. Human infection arises seven to 21 days after the inhalation of excretions from infected birds. Clinical symptoms can range from inapparent, to severe pneumonia with high fevers and multiorgan failure. Headache is frequently a prominent feature. Pulmonary imaging is abnormal in more than 50% of cases, with ground-glass changes the most common. In Australia, contact with infected parrots is the primary method of transmission, although recent outbreaks demonstrate alternative risks, such as gardening, lawn mowing, and in several cases, contact with an infected horse.13
Given most treatment guideline recommendations for community acquired pneumonia in Australia cover psittacosis, it is likely underdiagnosed, as serological follow up may not be performed in a recovered patient and molecular testing performed on respiratory specimens (sputa or nasopharyngeal swabs) is not always readily available. Treatment options for confirmed cases include doxycycline, azithromycin or clarithromycin.
Uncommon notifiable zoonoses in Australia
Tularaemia
Tularaemia caused by the fastidious gram-negative bacterium Francisella tularensis has generally been considered a northern hemisphere disease. Its multiple modes of transmission (particularly inhalation) and associated mortality has seen it classified as a Category A bioterrorism agent, although handling infected animals, being bitten by infected arthropods and consuming or contacting contaminated food or water are other modes of transmission. A range of wildlife species serve as vectors for this disease. Interestingly, in 2011 two cases of the more common ulceroglandular presentation (regional lymphadenopathy associated with an inoculation site) of tularaemia occurred in close proximity on the west coast of Tasmania. Both these patients were bitten by a ringtail possum.14
Subsequent metagenomic searching and culture of archived possum material from two separate clusters of possum deaths that had occurred in NSW in 2002 and 2003 revealed evidence of F. tularensis in these populations.15 In 2020, two more cases were identified; one linked to a ringtail possum and the other believed to have been acquired in a laboratory setting during necropsy of Australian wildlife, which did not include possum species. As a result, other potential animal sources in Australia are suspected but have not been clearly identified. The organism can be cultured, although when F. tularensis infection is suspected this should be referred to a public health reference laboratory for further characterisation. Both PCR and serological testing are available. Antimicrobials with well-established clinical efficacy include the aminoglycosides, doxycycline and ciprofloxacin.
Anthrax
Anthrax is a very rare disease caused by Bacillus anthracis, a gram-positive bacillus capable of forming resistant spores that can remain infectious for long periods in the environment. Susceptible animals may become infected through grazing, and spores can be transmitted directly from deceased animals, scavengers or from animal products (e.g. hides) from endemic areas. Although the disease has a worldwide distribution, it is extremely uncommon in Australia due to excellent veterinary services and outbreak response. Acquisition within Australia is generally restricted to the ‘anthrax belt’, a zone which runs through central Queensland and NSW and into northern Victoria.
Anthrax can take on several clinical forms depending on the portal of entry. Cutaneous anthrax (most common) usually involves a small painless papule which may evolve to a blister with a blackened eschar, while inhalation (far less common) may result in cough, fever, tachypnoea and shock. The organism can be grown from involved tissues, and often in blood cultures in cases of pulmonary, intestinal or central nervous system infection. Ciprofloxacin is the preferred empirical treatment while antimicrobial susceptibility testing results are pending. Anthrax is a life-threatening infection that requires prompt diagnosis and treatment, and any suspicion of anthrax infection must be immediately notified to public health units.
Hendra virus infection
Hendra virus is an RNA virus named after the Brisbane suburb where the first outbreak in horses was identified in 1994. The reservoir for this virus is flying foxes (‘fruit bats’) of the genus Pteropus. Horses are thought to be infected indirectly via ingestion of pasture contaminated with bat urine (Figure 2).16
{kind=link}
Human infection is rare and results from direct contact with secretions or bodily fluids of infected horses. The disease manifests similarly to influenza initially and often progresses to severe meningoencephalitis. There is a high mortality rate; only three of seven cases thus far have survived. If Hendra virus infection is suspected, this should be discussed with your local public health unit. Diagnosis is best made by PCR and a variety of specimens may be useful including nasopharyngeal swabs, blood or cerebrospinal fluid. PCR and serological testing are available at reference laboratories. Any request for testing of Hendra virus is notifiable.
Australian bat lyssavirus (ABLV) infection
ABLV is closely related to rabies virus and is found in several different bat species in Australia. The illness is transmitted via the saliva of an infected bat to a human, usually through a bite or scratch. The disease manifests as an acute viral encephalomyelitis after an incubation period of weeks to years. Initial symptoms may include fever or sensory changes at the site of a preceding animal bite. There have been three cases of ABLV, with no survivors.
The disease may be prevented by diligent vaccination (rabies vaccine) in those who are at increased risk (such as bat handlers, wildlife officers, veterinarians and laboratory workers manipulating lyssaviruses). Identification of at-risk exposures by GPs is crucial, as the disease can be prevented by careful postexposure prophylaxis. Postexposure management consists of wound care, rabies vaccine and human rabies immunoglobulin, dependent on the exposure category and vaccination status. Any possible ABLV exposure should be urgently discussed with your local public health unit so that prophylaxis can be arranged if indicated. Requests for laboratory testing for lyssavirus are generally limited to public health units or infectious diseases specialists, apart from monitoring immune status after vaccination.
Other notable zoonoses for primary care
Lymphocytic choriomeningitis virus (LCMV) has recently emerged as a rare cause of aseptic meningitis in Australia. LCMV is an arenavirus present in rodents worldwide; however, human infection has not been diagnosed previously in Australia. Current cases have arisen during the recent devastating mouse plague in Queensland and NSW (Figure 3). Serology and detection of the virus by PCR in cerebrospinal fluid specimens is the mainstay of diagnosis.
{kind=link}
Several different Rickettsia species are endemic to Australia and can cause disease in humans. These are transmitted by ticks, fleas or mites and include Rickettsia australis (Queensland tick typhus [QTT]); ticks), Rickettsia honei (Flinders Island spotted fever [FISF]; ticks), Rickettsia typhi (murine typhus; fleas) and Orientia tsutsugamushi (scrub typhus; mites). It is notable that most of these are geographically restricted in some way. For example, scrub typhus is restricted to the tropics (particularly coastal tropical Queensland, Litchfield National Park in the Northern Territory, and the Kimberley in Western Australia), QTT to the coast east of the Great Dividing Range, and FISF to Flinders Island and Tasmania.
Although their distribution and transmission are varied, the clinical syndromes associated with the different rickettsioses are remarkably similar. These include fever, rash, eschar at the site of a bite, myalgias and headache. Thrombocytopenia and hepatitis are common laboratory features, particularly in severe infection. Diagnosis may be made by serology and also PCR of the eschar or blood (in the acute phase). Scrub typhus produces the most frequently severe disease and complications, including pneumonitis and myocarditis, and rare fatalities have been reported. Early therapy reduces the risk of complications. Doxycycline is the preferred agent for treating all the rickettsial infections. Response to therapy is generally rapid.
Significance of zoonoses in Australia
The classic zoonoses are of substantial public health importance in Australia. There is also, however, a large and growing threat to human health from diseases not traditionally regarded as zoonoses, but which nevertheless have animal origins. Notifiable gastrointestinal infectious diseases are rising in Australia, with campylobacteriosis and salmonellosis contributing over 31,000 and 12,000 cases, respectively, in 2020.17 Animals (including livestock, backyard chickens and other pets) are common vectors for these diseases. Furthermore, transmission of multidrug-resistant organisms poses an additional challenge, with high rates of antimicrobial resistance seen in Campylobacter and Salmonella isolates from overseas travellers and imported meat products. Australian GPs have rightly recognised these issues, with a recent GP survey listing foodborne disease as the second most important zoonosis, behind only Q fever.18 Similarly, a 2019 US report prioritising zoonotic disease threats rated foodborne disease highly. Interestingly, this report ranked zoonotic coronaviruses a distant fifth.19 The subsequent SARS-CoV-2 pandemic has demonstrated how rapidly zoonoses can emerge and how difficult such events can be to envisage.
Conclusion
Established zoonoses remain a significant risk to the community, and the SARS-CoV-2 pandemic has highlighted the risks that emerging zoonoses pose to global health. A ‘one health’ approach is essential to the prevention and control of both existing and emerging zoonoses, and GPs are key stakeholders in this. Remaining well-informed regarding zoonoses and aware of the threat they pose is crucial to protecting the community. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.