Ovarian cancer. Old problems, new developments

With no available screening test and difficulties in diagnosing early-stage disease, ovarian cancer remains the sixth highest cause of cancer death in Australian women. Progress in treatment has been slow but incremental, and new treatments are leading the way.
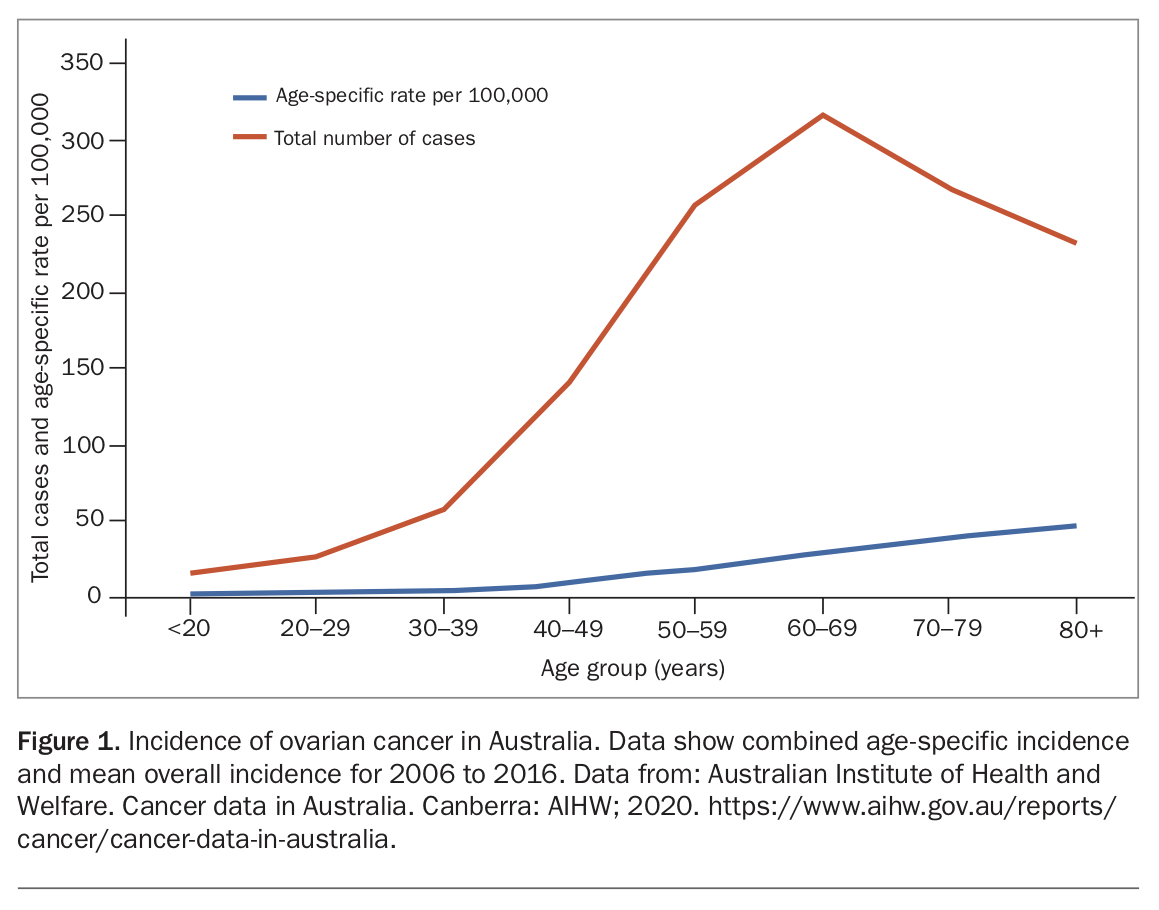
Ovarian cancer remains the 10th most common cancer diagnosed in women in Australia, but it is the sixth highest cause of death. One in 84 women will be diagnosed with ovarian cancer by the age of 85 years, and GPs may see only one or two cases in their entire careers.1 The incidence of ovarian cancer in Australia by age group is shown in Figure 1.
{kind=link}
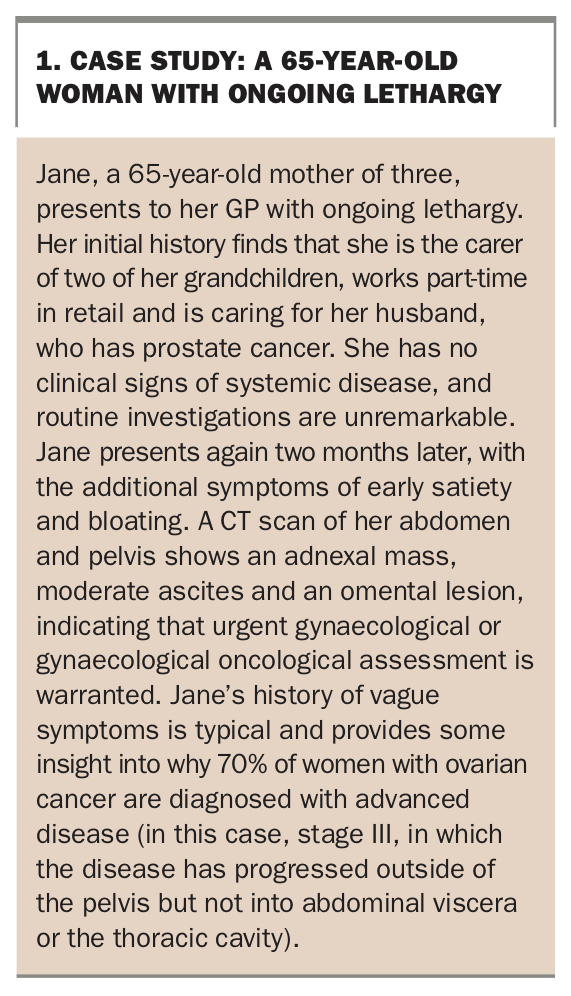
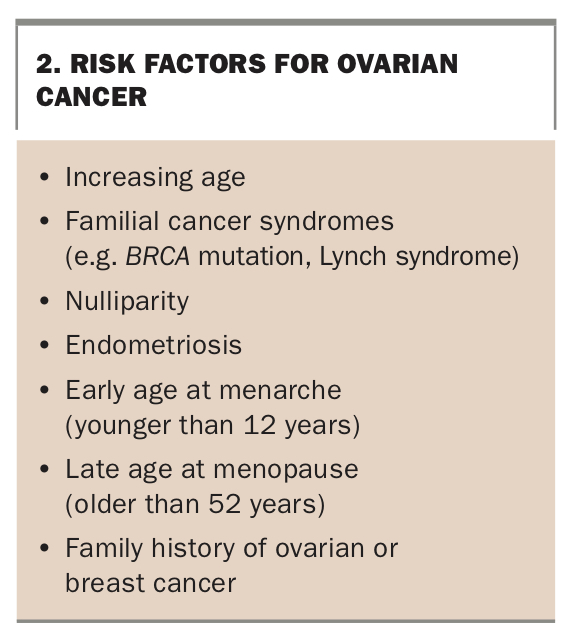
Although progress towards improving outcomes has been made, the pace has been slow. In 2016, the five-year overall survival for all ovarian cancer stages was 46%, but for stage III disease (at which 70% of patients with ovarian cancer are diagnosed; see case study in Box 1), it was only 25%.2 Risk factors for ovarian cancer, none of which are easily modifiable, are shown in Box 2.
{kind=link}
{kind=link}
The term ‘ovarian cancer’ encompasses ovarian, fallopian tube and primary peritoneal cancers. All share the same histopathological characteristics, immunohistochemical findings and genetic mutation profile. Most of what was previously called ovarian cancer has been shown to originate in the fimbria of the fallopian tube. This article refers to epithelial ovarian cancer (including tubal and peritoneal cancer) as ovarian cancer, as it is the most common subtype, responsible for about 85 to 90% of cases.
Symptoms
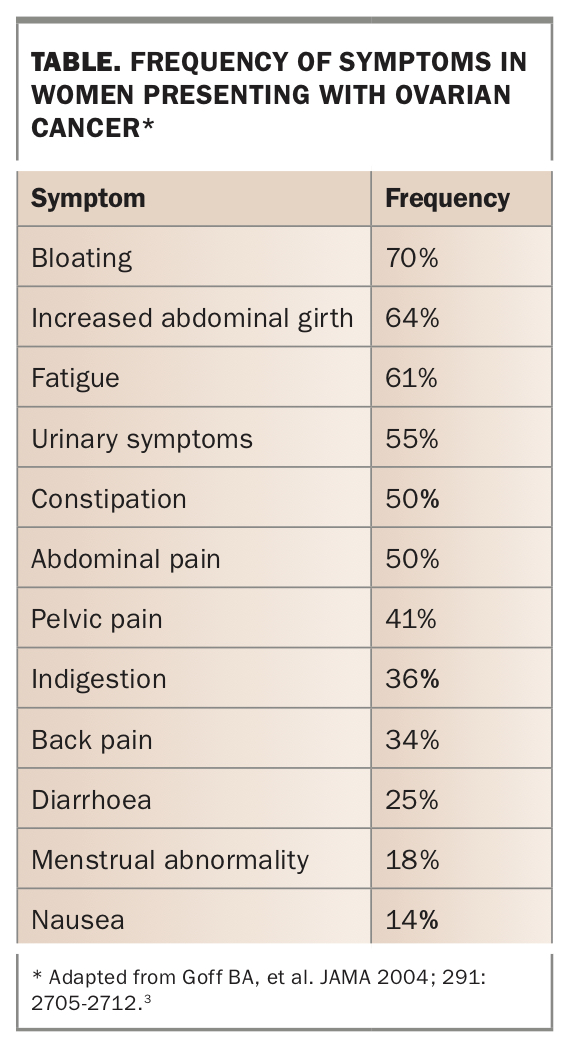
Historically, it has been said that ovarian cancer has no symptoms. This is not true; rather it whispers with a vague cluster of symptoms that, although well described, are often underappreciated by patient and doctor alike. These symptoms and the frequencies with which they occur are shown in the Table.3 Many symptoms are gastrointestinal in nature, leading to investigations of the gut rather than the reproductive system.
{kind=link}
The difficulty in achieving early diagnosis that is caused by the nonspecific nature of symptoms is compounded by the natural history of the disease (it often grows and spreads rapidly), the time of life at presentation (many symptoms are attributed to menopause) and the difficulty in distinguishing malignant ovarian lesions from their much more common benign counterparts on imaging. It is estimated that 5 to 10% of women will have an operation for an ovarian lesion in their lifetime, and the likelihood of a symptomatic ovarian lesion being malignant is one in 1000 for a premenopausal woman and three in 1000 for a woman aged 50 years.4,5
Diagnosis
Examination
If a patient’s history raises concern about an adnexal mass, a thorough abdominal and pelvic/rectal examination should be done. In a patient with advanced disease, the presence of ascites, a palpable omentum and intra-abdominal masses may be identified. On pelvic examination, a firm mass may be palpable in the pelvis. Rectovaginal examination may identify masses and/or nodularity in the pouch of Douglas. A rectovaginal examination is superior to the standard bimanual examination alone, but experience in this examination is necessary for clinically useful information to be gained.
Imaging and investigations
Initial imaging and other investigations will depend on the level of suspicion for local or advanced intra-abdominal disease. In a patient with primarily pelvic symptoms, and especially with abnormal bleeding, a transvaginal ultrasound is indicated. CT is the investigation of choice for patients with symptoms that suggest upper abdominal disease, including bloating, early satiety and ascites or a palpable omentum on examination. For patients with significant abdominal symptoms, use of oral contrast should be specifically requested as it is often not standard practice for CT undertaken privately.
As half of women with early-stage ovarian cancer will have normal levels of tumour markers, an intra-abdominal lesion should be suspected or identified before ordering tumour marker tests. In the absence of an intra-abdominal mass, testing for an elevated level of cancer antigen (CA)125 or carcinoembryonic antigen (CEA) is a fishing expedition that is likely to increase the woman’s anxiety and unlikely to provide any guidance for further investigations. Tumour marker levels are often elevated in women with endometriosis or fibroids and during ovulation and menses, so their specificity for identifying malignancy in premenopausal women is greatly reduced. Tumour marker testing is most useful in the context of a postmenopausal woman with a complex ovarian lesion.
Cancer Australia has developed a two-page guide for GPs on the assessment of symptoms that may be ovarian cancer (Box 3).6
{kind=link}
Assessing likelihood of malignancy after imaging
Scoring systems are available to help identify whether an ovarian mass is likely to be malignant. The most widely known of these is the Risk of Malignancy Index (RMI). The International Ovarian Tumor Analysis group has developed several other risk models, including the Simple Rules and the ADNEX (assessment of different neoplasias in the adnexa) model. The RMI and one of the ADNEX models use CA 125 level in their diagnostic algorithm. It has recently been suggested that the ADNEX and a version of the Simple Rules are the best at distinguishing between benign and malignant masses.7
Important elements that should be included in the imaging report are the maximal diameter of the lesion; size of the largest solid component; number of locules and papillary projections; the presence of acoustic shadows, ascites, bilateral masses and cystic spaces; and the degree of vascularity.
On receipt of an ultrasound report indicating the presence of an adnexal mass, a decision about whether to order tumour marker tests, and which ones if so, should be made. In women younger than 40 years, the differential diagnosis of an adnexal mass includes germ cell malignancies. In both pre- and postmenopausal women with a suspicious mass, tests for CA 125 and CEA should be ordered, preferably between Day 8 and Day 12 of the menstrual cycle in premenopausal women. A CA 19-9 test does not provide any additional useful information. When a germ cell tumour is suspected on imaging in women younger than 40 years, testing of lactate dehydrogenase, alpha-fetoprotein and human chorionic gonadotropin levels is also needed.
The patient can then be referred to a gynaecologist or gynaecological oncologist. All general gynaecology units will have a referral pathway to a gynaecological oncology unit. In NSW and the ACT, gynaecological oncology units are listed on the Canrefer website (www.canrefer.org.au).
Management
Cancer Australia recommends that all women diagnosed with ovarian cancer be managed within a multidisciplinary team.8 Women with epithelial ovarian cancer are managed primarily with surgery, with or without chemotherapy.
The use of neoadjuvant chemotherapy before surgery has become more common as data continue to accumulate showing that its oncological outcomes are equivalent to those from chemotherapy only after surgery, with less perioperative morbidity. There are criteria specifying which patients are suitable for neoadjuvant chemotherapy, including stage IVA disease, peritoneal carcinomatosis and poor performance status. Primary debulking surgery remains the gold standard if optimal debulking can be achieved.
Standard chemotherapy includes six cycles of carboplatin and paclitaxel with or without bevacizumab, with surgery performed either at the beginning or after the third cycle. This treatment regimen takes at least 24 weeks. The removal of all macroscopically visible disease during surgery – a residual zero resection (R0) – is associated with an improvement in overall survival. This will nearly always include removal of pelvic organs and omentum, and removal of visceral organs encased by peritoneal tumours (e.g. bowel resection or splenectomy) as required. A higher residual disease burden is associated with worse overall outcomes.
Recent advances in treatment have highlighted the importance of the molecular characteristics of ovarian cancer. The Australian Ovarian Cancer Study found that 14% of all women with epithelial ovarian cancer (excluding those with mucinous tumours) and 17.1% of women with high-grade serous carcinoma had germline mutations in the BRCA1 or BRCA2 gene.9 For this reason, all women younger than 70 years with nonmucinous epithelial ovarian cancer are offered Medicare-funded genetic testing. The detection of a BRCA mutation has implications for both the patient and her family. A woman who is found to have a pathogenic BRCA variant will have an increased risk of breast cancer and will be referred to a familial cancer centre to discuss her risks and to facilitate predictive testing for unaffected family members.
Women with either a germline or somatic BRCA mutation have access via the PBS to the targeted therapy olaparib, a poly (ADP-ribose) polymerase (PARP) inhibitor, as ongoing maintenance treatment after chemotherapy. This treatment significantly extends progression-free survival at both initial treatment and in recurrent disease.10 Women with advanced (suboptimally debulked stage IIIB or IIIC, or stage IV) disease can be treated with the vascular endothelial growth factor monoclonal antibody bevacizumab as part of initial and continuing treatment through the PBS. It is recommended that women with a pathogenic BRCA variant have bilateral salpingo-oophorectomy after they have finished having children and are over the age of 35 years if they have a BRCA1 mutation, or over the age of 40 years for BRCA2.11
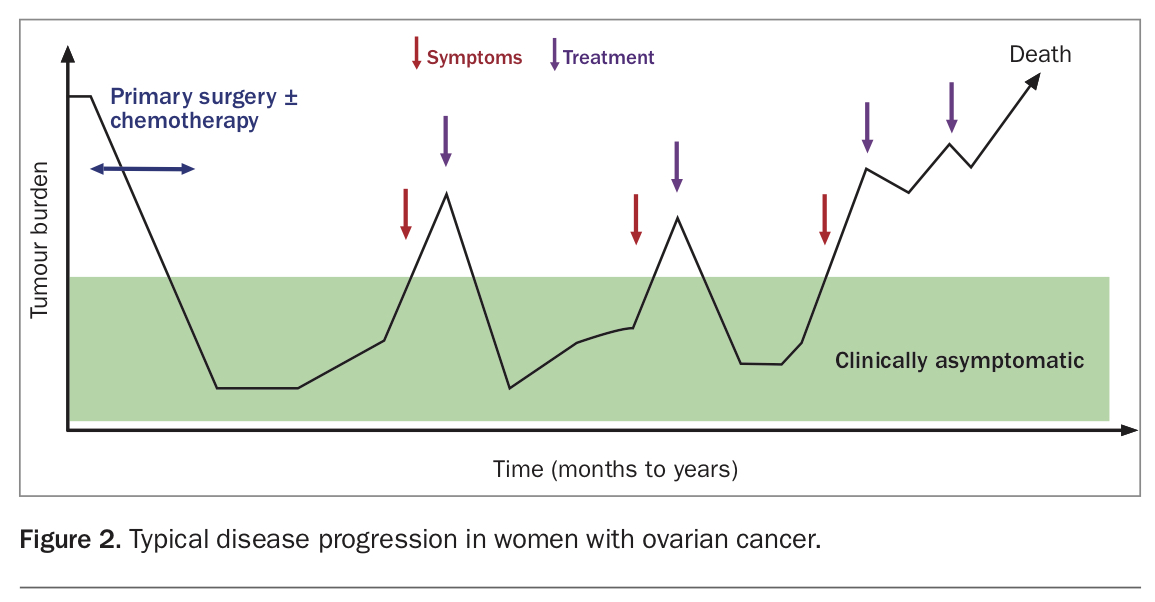
At least 80% of women with high-grade epithelial ovarian cancer will respond to treatment and enter a period of remission after debulking surgery and chemotherapy. Although some women will be cured by this treatment, most will have a recurrence of their disease. Ovarian cancer can be viewed in such cases as a chronic disease, as these women will have periods of good health followed by recurrence and further treatment. Figure 2 illustrates how disease treatment, recurrence and disease-free intervals may progress. The duration of remission tends to decrease after each treatment cycle. Palliative care is an essential part of this treatment journey. The timing of this will depend on the patient’s wishes, but it is well established that early referral and linking with palliative care improves overall quality of life and decreases the number of futile treatments.12
{kind=link}
Post-treatment surveillance
The aim of surveillance is to detect recurrence, identify and manage side effects of treatment and provide reassurance to the well woman. Follow up with treating specialists usually occurs every three months for two years after completion of chemotherapy, then six-monthly in years three to five.
The frequency and form of surveillance are subject to several variables, including the patient’s anxiety, geographical location, medical comorbidities, social situation and disease trajectory. Follow up must be in a form that best serves the goals of the woman. A Cancer Australia guideline on follow up of women with epithelial ovarian cancer specifically discusses the stress and anxiety associated with follow-up investigations and appointments.13 GPs are well placed to identify the degree of concern women have about their follow up and to work with the patient’s oncology team to adjust it as needed.
The use of CA 125 testing as part of follow up is controversial, and clinicians will often discuss the benefit (or lack thereof) of using it as a surveillance tool. In a trial of 1400 women with ovarian cancer, patients were randomly assigned to either receive treatment when their CA 125 level was elevated or to delay treatment until symptoms occurred. The study found no difference in survival between those treated early and those whose treatment was delayed (mean delay to treatment was 4.8 months).14 Importantly, the early-treatment group had an earlier reduction in their global health score compared with the delayed-treatment group. Given the results of this trial, it is advisable to consult with the oncology team if a woman requests this test during follow up. CA 125 testing is of no use as a surveillance tool if the level was never elevated at diagnosis.
Screening
The evidence on screening for ovarian cancer is clear. Multiple extremely large trials have found that there is no role for routine ultrasound or CA 125 testing in screening for ovarian cancer in women with population-level risk or high risk.15-20 In May 2021, after a median of 16.3 years of follow up, the UK Collaborative Trial of Ovarian Cancer Screening found no survival benefit from screening for ovarian cancer in more than 200,000 women.15 Cancer Australia has issued a position statement in support of this finding and provided a ‘frequently asked questions’ document to help doctors educate patients (see case study in Box 4).21,22 If screening is started, it is difficult to stop. Women thought to be at high risk can be identified through guidance from Cancer Australia (Box 3) and should be referred to genetic counselling services before undertaking any testing.23 Before initiating screening, GPs can discuss the issue with their local gynaecological oncology team.
{kind=link}
Conclusion
Ovarian cancer is a devastating diagnosis for a woman and her family. Early diagnosis leads to better outcomes, but the rapid disease trajectory, vague symptoms and lack of a good screening test mean that most women will be diagnosed with advanced disease. Prompt referral to a specialist gynaecological oncology unit and a multidisciplinary approach to management will give women the best chance of a better outcome. MT
COMPETING INTERESTS: None.
Acknowledgements: The authors thank Letitia Lancaster RN and Dr Cameron R. Evans for their input into this article.
References
epithelial_ovarian_cancer.pdf?file=1&type=node&id=3958 (accessed May 2021).
for_ovarian_cancer_in_asymptomatic_women.pdf (accessed May 2021).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.