Ovarian cysts: distinguishing the physiological from the concerning

Ovarian cysts occur frequently in women of all ages and can be physiological, benign or malignant. As cysts often first present in primary care, it is important that GPs assess the cyst and determine appropriate follow up. Patient history, age, menopausal status and physical examination will help determine the risk of a concerning cyst and whether referral to a specialist is warranted. First-line investigations include transvaginal ultrasound and, in some cases, testing for cancer antigen 125 levels.
Ovarian cysts can be physiological, benign or malignant. Although most ovarian cysts encountered in general practice are of no clinical concern, certain scenarios warrant further investigation, follow up and/or specialist referral. We present a structured approach to assessment based on common clinical scenarios (Flowchart), allowing GPs to distinguish physiological from more concerning ovarian cysts.
Ovarian cyst prevalence and classification
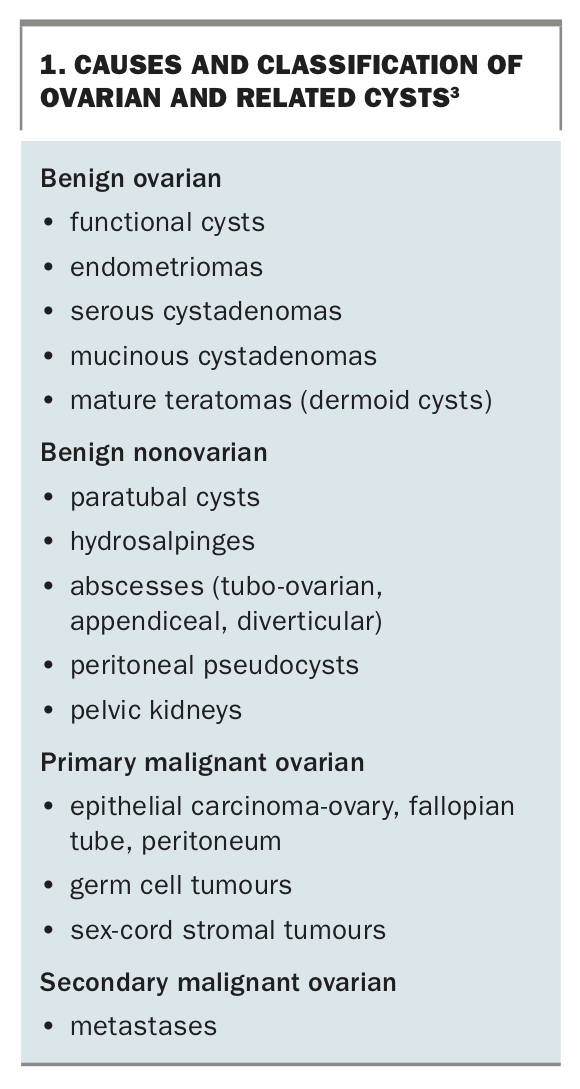
Ovarian cysts occur frequently in women of all ages. Their prevalence has been reported at 6.6% in asymptomatic premenopausal women and 14% among postmenopausal women.1,2 Common types of ovarian cysts include physiological or functional cysts (often ovulation related), haemorrhagic cysts, dermoid cysts, endometriomata, cystadenomas and malignant cysts (Box 1).3,4 Although most cysts are benign, ovarian carcinoma has an overall incidence of 9.8/100,000 in Australia, with a peak age at diagnosis of between 65 and 69 years.5 Late cancer diagnosis correlates with poor outcomes, underscoring the need for early diagnosis in the general practice setting.
{kind=link}
Many women with cysts will present to GPs after incidental discovery on imaging/radiology. Key challenges include distinguishing physiological from concerning cysts, determining follow-up requirements and knowing when to refer to a specialist. The key clinical features, investigations and management points for GPs to consider are discussed in this article.
History and examination
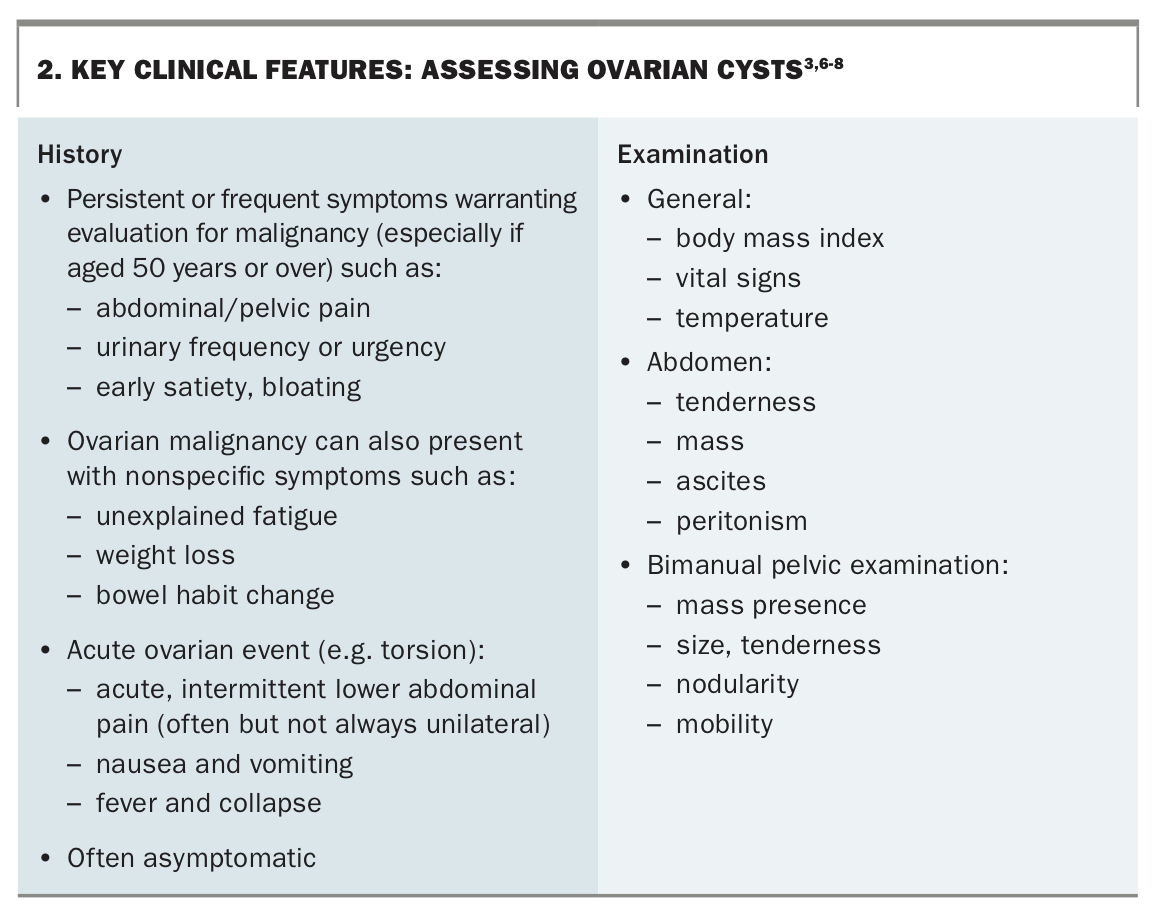
Key clinical features guiding the management of ovarian cysts are outlined in Box 2.3,6-8 A patient history should assess risk factors for ovarian malignancy, including older age, postmenopausal status, nulliparity, BRCA mutations, Lynch syndrome and a family history of ovarian or breast cancer. According to recent international guidelines, age and menopausal status are particularly crucial in assessing ovarian cysts as ovarian cancer is much more common with advancing age3,4,6,7 and cysts after the menopause are unlikely to be oestrogen-related. GPs should ask about contraception, as physiological cysts may be more unexpected among women using contraceptive methods that suppress ovulation.
{kind=link}
GPs should also enquire about bloating or increased abdominal girth, early satiety, or the new onset of unexplained urinary symptoms.7 Although such symptoms are nonspecific, their persistent or frequent presence without clinical explanation should prompt investigation.7 Other symptoms that warrant investigation include unexplained weight loss, fatigue or bowel habit changes, particularly in those aged 50 years and over.7
Physical examination includes recording body mass index, performing an abdominal examination for ascites and masses, and a pelvic bimanual examination to assess the mass and its tenderness, nodularity and mobility.3 Where a combination of these symptoms are present in an older patient, or ascites or a pelvic mass is noted, immediate specialist referral is appropriate.
First-line investigations
Transvaginal ultrasound
Transvaginal ultrasound is recommended to assess ovarian cyst size and classification.
Benign cysts
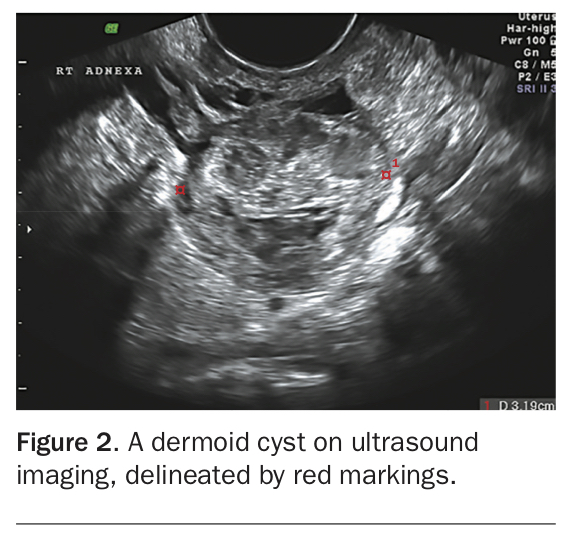
In premenopausal patients, simple cysts of less than 50 mm in size (Figure 1) without ultrasound risk features do not require follow up (Flowchart).3 These ‘functional’ physiological cysts usually resolve after several menstrual cycles. Referral to a provider who specialises in gynaecological ultrasound is recommended. If there are sonographic features of a dermoid cyst (Figure 2) or an endometrioma and the sonologist is clear that this is the diagnosis, no further investigation of the cyst is needed.
{kind=link}
{kind=link}
Cysts warranting further surveillance and/or specialist referral
Cysts that are 50 to 70 mm in size should be monitored with repeat transvaginal ultrasound after three to four months (Flowchart). Cysts persisting or increasing in size are less likely to be functional, and warrant specialist referral.3 Because larger cysts (more than 70 mm in size) are often more difficult to assess sonographically, specialist referral is recommended to determine the appropriate next steps.3,9-11 Any cysts with sonographic risk features such as bilateral lesions, multilocular, solid or papillary components, or evidence of ascites or metastases (Flowchart) require immediate specialist referral. Although ultrasound can predict risk of malignancy with an overall sensitivity of 86 to 91% and specificity of 68 to 83%,10 no single ultrasound feature alone can definitively establish malignancy without a histological diagnosis arranged by the specialist.3 Additionally, although Doppler flow assessment at ultrasound may be informative for cyst characterisation, it cannot be used in isolation to determine malignancy risk.12,13
Cancer antigen 125 blood test
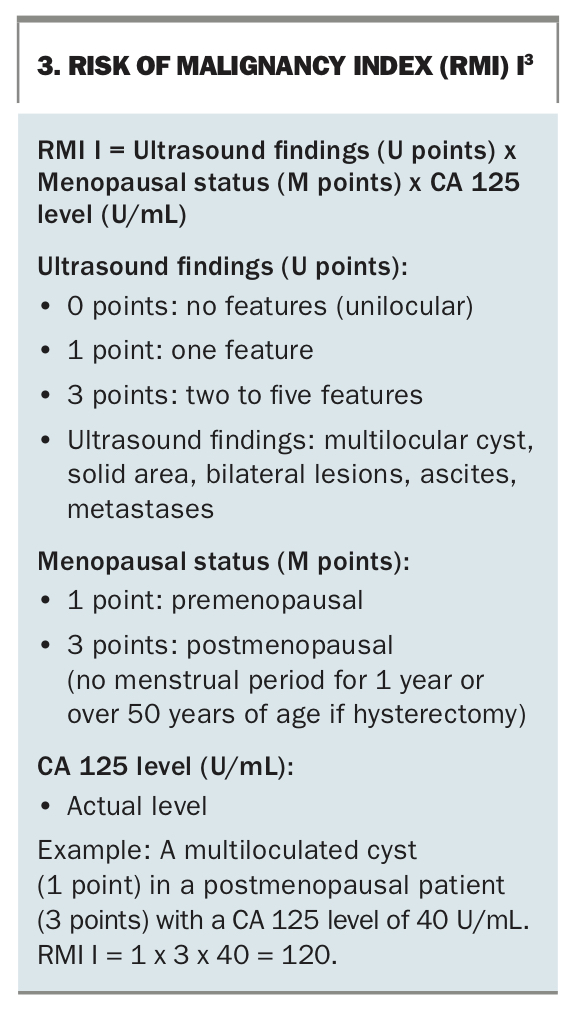
The cancer antigen (CA) 125 blood test is the most useful adjunctive investigation for large or enlarging cysts, symptoms (above), cysts with sonographic risk features and any cyst in a postmenopausal patient. CA 125 measurement is used for the risk of malignancy index (RMI) calculation and to guide specialist investigation and management. The RMI has evolved through four iterations – RMI I to IV – with RMI I the most widely used and validated.4 Therefore, RMI I will be used throughout this article. The RMI I incorporates menopausal status, cyst features on transvaginal ultrasound and CA 125 level (Box 3), and is the most effective model for predicting suspected malignancy.3,9 However, GPs need to be aware that a normal CA 125 level (below 35 IU/mL) can be falsely reassuring in early malignancy and does not definitively exclude ovarian cancer. CA 125 may also be less sensitive in borderline ovarian tumours.3,14
{kind=link}
CA 125 in premenopausal patients
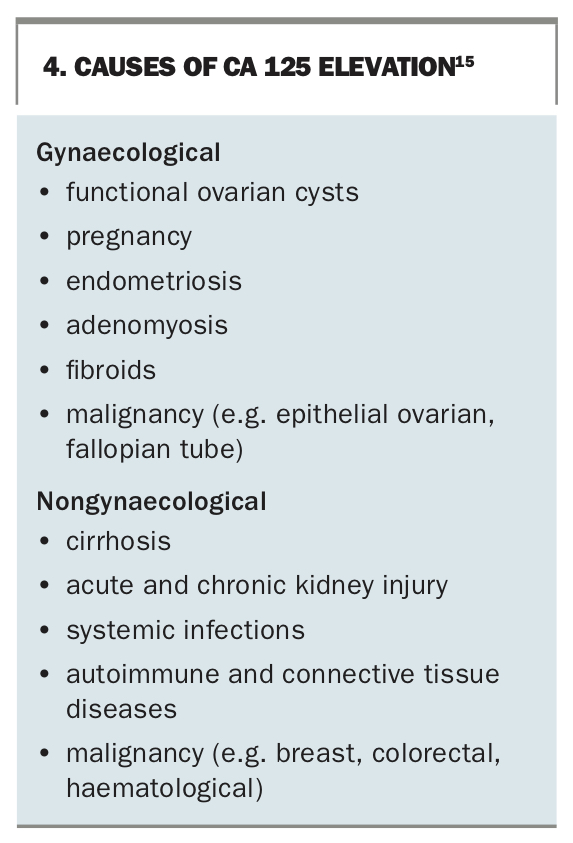
For asymptomatic ovarian cysts occurring before menopause, GPs should not routinely use the CA 125 level to determine the need for specialist referral. Rather, they should only measure CA 125 when the decision for specialist referral has already been made (based on factors discussed above), as levels may inform specialist management.3 Premenopause, CA 125 elevations can occur due to a variety of conditions (Box 4)15 and levels cannot reliably differentiate benign from malignant lesions.3 When referring patients aged 40 years and younger to the specialist, GPs should also perform blood tests including alpha fetoprotein, human chorionic gonadotrophin and lactate dehydrogenase levels because germ cell tumours are more common in this group.3
{kind=link}
CA 125 in postmenopausal patients
GPs should measure CA 125 levels in postmenopausal patients with ovarian cysts to allow RMI I calculation and subsequently decide on the need for specialist referral (Flowchart). CA 125 is a better indicator of the malignancy risk of ovarian cysts in postmenopausal patients than in premenopausal patients.4 A meta-analysis has shown that a CA 125 level of 35 IU/mL or higher in postmenopausal patients has a sensitivity of 69 to 87% and specificity of 81 to 91% for the detection of ovarian cancer.10
Other blood tests
Other serum biomarkers are generally not recommended when investigating ovarian cysts in primary care settings. CA 19-9 is a biomarker used in the investigation of gastrointestinal and pancreatic cancers. Recent studies have found no clear diagnostic benefits associated with CA 19-9 measurement for ovarian cysts, and its use is not recommended.16 Human epididymis protein 4 (HE4) has been used alongside CA 125 (without ultrasound features) to calculate the predictive ‘risk of malignancy algorithm’ (ROMA).8,17 Conversely, the International Ovarian Tumour Analysis (IOTA) Group has produced a risk classification system based on sonographic features alone, without serum markers.18 In practice, however, the RMI I (combining ultrasound features with CA 125 level) remains the most widely used and endorsed model for predicting suspected malignancy.
Management of ovarian cysts
GP management
For simple cysts smaller than 50 mm in asymptomatic patients or when a confident sonographic diagnosis of a benign cyst has been made by an experienced radiologist, reassurance is appropriate. Larger simple cysts (50 to 70 mm in size) in premenopausal patients should be followed up with repeat imaging after three to four months to assess for resolution or persistence (Flowchart). Given the potential increased risk of torsion, GPs should advise patients with ovarian cysts to seek urgent medical attention in the unlikely event of acute lower abdominal pain.19,20
Specialist referral
Specialist referral is indicated for ovarian cysts with one or more ultrasound risk features, larger cysts (more than 70 mm in size), cysts of size 50 to 70 mm that persist on repeat imaging or cysts in postmenopausal patients in the context of a nonreassuring RMI I (Flowchart and Box 3).
Clinicians should have a very low threshold for specialist referral for ovarian cysts among patients with known genetic risk factors for ovarian cancer (such as BRCA mutations). Although referral will usually be to a gynaecologist, direct referral to a gynaecological oncologist is recommended in certain circumstances, such as a high RMI I in a postmenopausal patient or the presence of ultrasound risk features.4,7 Specialist management can include further imaging and monitoring of serum markers, diagnostic laparoscopy, cystectomy for tissue diagnosis or, for those with a higher malignancy risk, a full staging laparotomy and frozen section with or without tissue debulking under gynaecological oncology.
Cyst aspiration is generally not recommended because if the cyst is malignant, this can result in a higher risk of recurrence.3,8 For asymptomatic simple ovarian cysts in women of reproductive age, no specific medical therapy has been shown to hasten cyst resolution, with a Cochrane review demonstrating no benefit to the use of hormonal contraceptives.3
If the specialist opts for observation, patients may be discharged back to their GP for a period of ongoing surveillance. Many patients can cease surveillance where there has been resolution of the cyst or no significant change for 12 months, but specific management recommendations will depend on the clinical scenario.4
Other considerations for GPs
Other specific cyst-related diagnoses may be suggested depending on the clinical context and can include:
- acute adnexal torsion, requiring urgent emergency care19,20
- endometriomas, indicating significant endometriosis, even in the absence of symptoms
- cysts in pregnancy, which can pose a higher risk of adnexal torsion19,20
- theca lutein cysts in the context of assisted reproductive technology or, rarely, due to gestational trophoblastic disease.
A detailed discussion of the work-up and management of these conditions is beyond the scope of this article.
Finally, ovarian cysts can be associated with significant anxiety and it is important to sensitively reassure patients when appropriate. Avoiding unnecessary surveillance, investigations and referral for those at very low risk is another important consideration.
Conclusion
GPs commonly encounter ovarian cysts and although many cysts will be functional and benign, the opportunity for follow up or referral in concerning scenarios should not be missed. In distinguishing physiological from concerning cysts, relevant clinical information, risk factors for malignancy and ultrasound risk features are key considerations. Transvaginal ultrasound is the initial investigation of choice but other testing, including measurement of CA 125 levels in some circumstances, can stratify risk. GPs have a crucial role in providing reassurance where appropriate and in deciding which cases to follow up and/or refer. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.