Breast cancer: challenges in treating young women

Although breast cancer in women aged 40 years or younger is rare, these women face unique challenges. A strong family history of breast cancer can help identify young women at potentially high risk of breast cancer who would benefit from referral for risk assessment. A multidisciplinary approach to management includes guiding the patient through diagnosis and treatment. Addressing psychosocial impacts and counselling young patients about the impacts on fertility are essential.
- Breast cancer in women aged 40 years and younger is rare, comprising 5 to 7% of all breast cancers.
- Breast cancer in young women is associated with a higher rate of a positive family history and mutations in breast cancer genes 1 and 2 and tumour protein p53 (BRCA1, BRCA2 and TP53).
- Women identified as high-risk for breast cancer should be referred to a familial cancer service for assessment and screening.
- Most young women with breast cancer are symptomatic and present at a more advanced disease stage; therefore, any breast changes should be thoroughly investigated.
- Careful consideration should be given to imaging modality for young women, as dense breast tissue impedes accurate interpretation of standard breast imaging such as mammograms. Ultrasound is the initial imaging investigation of choice in young women with breast symptoms.
- Surgical options should be discussed; breast conservation should be offered when possible and adequate time and counselling given before proceeding with more extensive or bilateral surgery.
- A multidisciplinary team, of which the GP is a part, is the cornerstone of management.
Breast cancer in young women is arbitrarily defined as age at diagnosis of 40 years or younger. It is rare, comprising 5 to 7% of all breast cancers in developed countries, with higher incidence in developing countries.1-3 It is, however, the most commonly diagnosed cancer and cause of death in women under 40 years of age.4 In Australia in 2021, an estimated 5.5% of breast cancer diagnoses were in young women.5
Breast cancer is a distressing diagnosis for women of all ages and life stages, and young women with breast cancer face additional and unique challenges. This group particularly needs care in a specialist multidisciplinary setting, with input from specialists, including a breast surgeon, medical and radiation oncologist, reconstructive surgeon, gynaecologist and fertility specialist, pathologist, radiologist, breast care nurse, clinical trial expert, physiotherapist and psychotherapist. Issues such as fertility should be addressed before starting treatment. Lifelong and survivorship follow up is also important and the family or primary care physician plays a significant role in this aspect of management. Research and trials focused on best standards for managing breast cancer in women aged 40 years and younger, including diagnosis and communication, should be a priority.6
Family history and genetics
Breast cancer in young women is more likely to be associated with a positive family history and gene mutations than in older women.7 An assessment of family history and genetic counselling should therefore be considered in all young women diagnosed with breast cancer, as they are more likely to have a detectable mutation in the breast cancer genes 1 and 2 (BRCA1 and BRCA2) compared with the general population.8
A family history that suggests an inherited gene mutation (in the BRCA1, BRCA2 and tumour protein p53 [TP53] genes) includes:9
- the presence of breast cancer in two or more first-degree relatives on the same side of the family
- breast and ovarian cancer in one person
- bilateral breast cancer
- male breast cancer
- Ashkenazi Jewish ancestry.
Young women who fit these criteria are considered to be at high-risk for breast cancer. Such women, including those already diagnosed with breast cancer, should be referred to a familial cancer service for assessment, screening planning, confirmation of MRI screening eligibility and to be considered for genetic testing.10 Failure to identify a known high-risk gene defect does not exclude the presence of a breast cancer-associated mutation, and ongoing surveillance is important. When a mutation is identified, the patient will need to be counselled regarding surveillance and surgery, such as prophylactic mastectomy and bilateral salpingo-oophorectomy, which have been shown to reduce the risk of second primary breast cancer and ovarian cancer.11,12
Screening
Regular screening of healthy, asymptomatic, average-risk young women using any form of imaging is not recommended because of the low incidence of breast cancer detection.6 These women are not eligible to attend the national BreastScreen Australia Program. Younger women tend to have dense breast tissue, which impedes accurate interpretation of mammograms, causing high recall rates, unnecessary biopsy, additional imaging and increased anxiety, with low cancer detection rates.13 An annual mammogram can be considered for high-risk women aged over 35 years. A screening mammogram should not be performed in high-risk women aged under 35 years.10
Annual MRI screening should only be started after formal assessment by a breast specialist or familial cancer service. Depending on national and regional guidelines, MRI screening is offered to women who carry BRCA1, BRCA2 (starting age 25 years) and TP53 (starting at age 20 years) mutations. Women who are firstdegree relatives of mutation carriers have a 50% risk of carrying the mutation themselves and are also eligible for MRI screening, as are other high-risk women from families not tested or whose test results are inconclusive for BRCA mutations. Other eligible groups include women who have undergone mantle radiotherapy before the age of 30 years (e.g. for Hodgkin’s lymphoma) and high-risk women already diagnosed with breast cancer.10
Diagnosis
The diagnosis of breast cancer in young women is more difficult and often delayed. Dense breast tissue, physiological changes due to menstruation, pregnancy and lactation, high-grade cancers mimicking benign lesions and imaging limitations in this group, coupled with a lower index of suspicion, contribute to the difficulty and delay. Imaging diagnosis needs to be made efficiently by an experienced breast radiologist who understands the challenges that young women with breast cancer face, including the choice and timing of appropriate investigations.
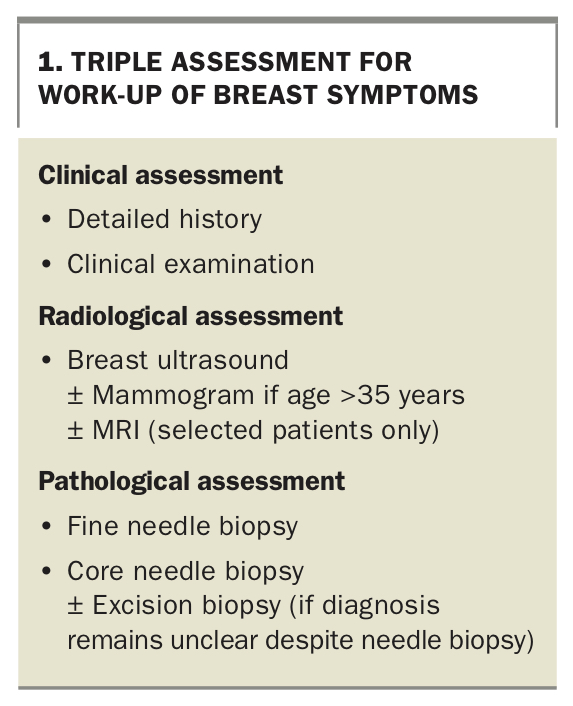
More than 90% of young women with breast cancer are symptomatic and present at a more advanced disease stage and with associated poorer prognosis. Young women should, therefore, be advised to promptly report and seek advice regarding any changes they perceive to their breasts. Any new breast changes should be approached in the time-honoured fashion of the triple assessment – history and physical examination, imaging and biopsy (Box 1). The triple test will detect over 99.6% of breast cancers.14 However, it should be remembered that, even in high-risk groups, most breast changes are not due to cancer.
{kind=link}
Mammograms have reduced sensitivity and specificity in young women due to increased breast density, which obscures malignant lesions.15 A mammogram is, however, useful for the detection of microcalcification, and would only be used in young women with an identified cancer to assess the cancer further and to look for associated ductal carcinoma in situ (DCIS). Tomosynthesis, or 3D mammography, appears to be a superior imaging modality for young women with dense breasts.16 Ultrasound is less affected by breast density and is more useful in the work-up of breast symptoms in young women, and is routinely used for guided biopsy and assessment of the axilla. Ultrasound is the initial imaging investigation of choice in most symptomatic young women.
MRI assessment is used with increased frequency in diagnosis, particularly in:
- complex cases of diagnosed breast cancer where discrepancy exists between clinical assessment and conventional imaging
- cases where a lesion is present but conventional imaging is inconclusive
- cases of biopsy-proven regional lymph node metastases with no identified breast primary.
Preoperatively, MRI is used to identify the extent of disease in cases of high-grade DCIS and invasive lobular carcinoma and to identify occult disease in the contralateral breast. It is also being increasingly used to assess patients undergoing neoadjuvant chemotherapy both before and after treatment.
The timing of breast imaging in young women is important. To optimise results, mammogram should be performed in the first two weeks of the menstrual cycle and MRI in the second week of the menstrual cycle (day 7 to 14), when breast tissue is most likely to be less dense due to cyclical hormonal changes. Ultrasound can be performed at any time in the menstrual cycle and is usually the first diagnostic modality used to investigate a clinical abnormality in all young women, including pregnant and lactating women.17
Breast implants
Breast augmentation is a common aesthetic procedure performed on young women worldwide. Breast implants are not a risk factor for developing breast cancer and young women with breast implants will present with breast changes similar to those as women without breast implants.18 Diagnosis and work-up may be more difficult; however, breast changes must be assessed in the usual manner, and expert breast radiology is needed. A high-risk family history for breast cancer should not stop young from women undergoing augmentation. They should undergo a preoperative diagnostic check, including clinical examination and ultrasound.
Tumour characteristics and biology
Breast cancers in young women show aggressive biological characteristics compared with older women, regardless of whether the young patient is a recognised mutation carrier. Tumours are more often high grade (Grade 3 – increased cellular abnormality and higher degree of proliferation) and more likely to be oestrogen (ER) and progesterone (PR) receptor negative. Compared with the older cohort, young patients with breast cancer show a higher prevalence of human epidermal growth factor receptor 2 (HER-2) positivity and triple negative (ER, PR and HER-2 negative) breast cancer. The tumours are associated with lymphovascular and lymphocytic invasion. Tumour gene expression profiling shows a higher proportion of more aggressive basal-like and HER-2 enriched tumours.19 Regardless of diagnostic stage, these features suggest different tumour biology and predict poorer prognosis.20
Stage
Stage of disease is assessed by taking into account the tumour size, extent of involvement of regional lymph nodes and the presence or absence of distant metastases. Young women are usually symptomatic at the time of presentation, with palpable and larger tumours, and frequently present at a higher disease stage.7 This may result from a combination of tumour biology characteristics and delays in diagnosis.
Treatment
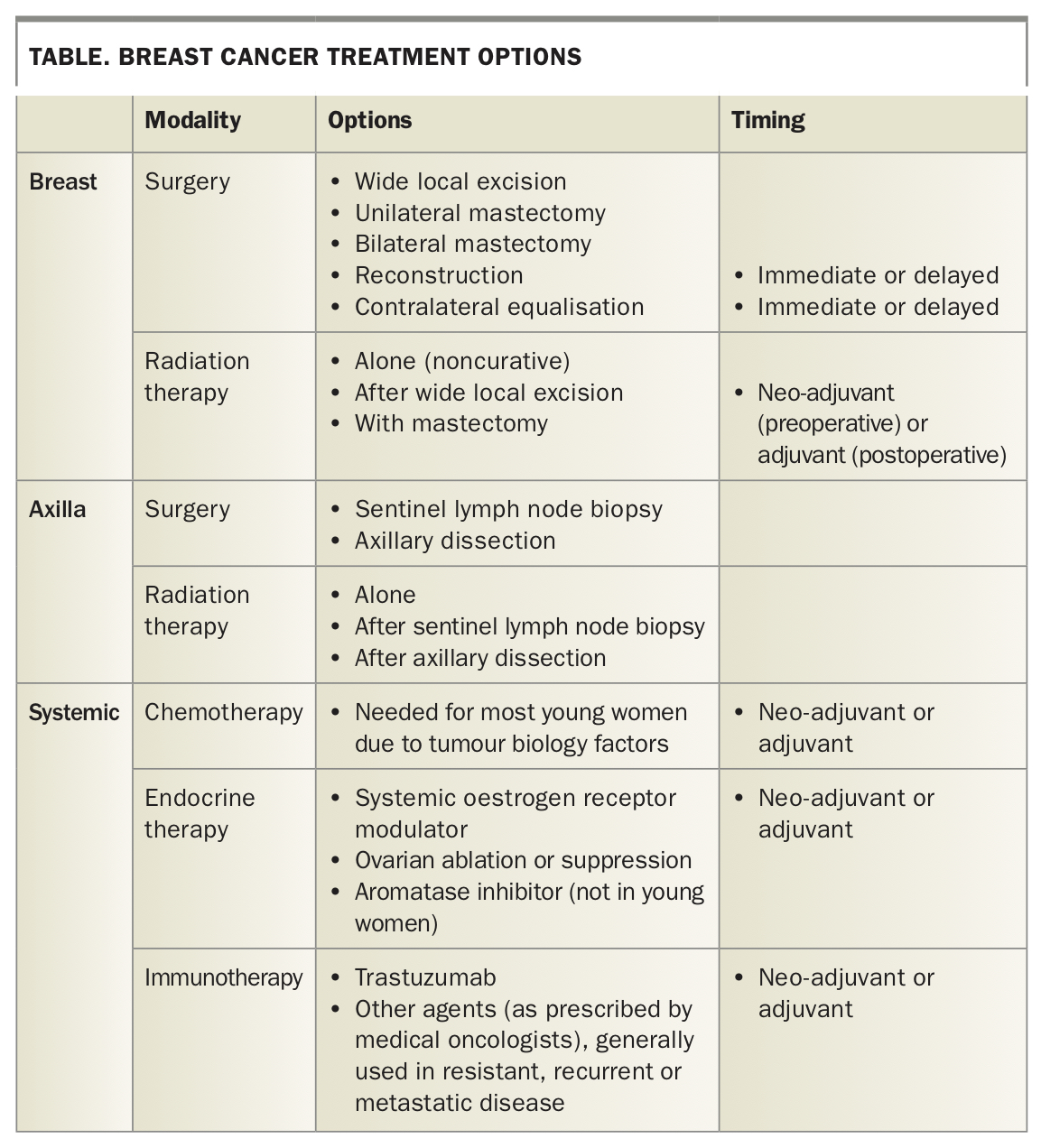
Breast cancer treatment is similar in younger and older women. Treatment options include surgery with or without reconstruction, radiotherapy, adjuvant or neo-adjuvant chemotherapy, endocrine therapy and immunotherapy; these are summarised in the Table.
{kind=link}
Surgery
Breast conservation vs mastectomy with or without reconstruction
Young age is an independent risk factor for increased local breast cancer recurrence. However, as with older patients, mastectomy in young women has not been shown to improve overall survival when compared with breast conservative surgery and radiotherapy.21 There has been a trend for routine bilateral mastectomies in recent years among young women diagnosed with breast cancer.6 There is no evidence that this benefits patients who are noncarriers of a gene mutation, although it could be considered in other high-risk women. Adequate time and counselling are needed before proceeding with this surgery to avoid hasty emotional decisions and other drivers, such as fear of cancer and anxiety.22 As with older patients, surgery should be tailored to the individual and guided by tumour factors, including size and location, the size of the breast, the ability to achieve clear margins and create an acceptable cosmetic outcome, the outcome of genetic testing where applicable and patient preferences.
When breast conservation is possible, it should be offered. A discussion regarding oncoplastic surgical techniques, such as therapeutic breast reduction (to remove the cancer) and immediate or delayed contralateral reduction, particularly if significant asymmetry is anticipated, can help maximise cosmesis and maintain patient body image, while still providing sound oncological resection.
Breast reconstruction is an important aspect of psychosocial wellbeing and impacts quality of life, and should be discussed with patients in whom mastectomy is deemed necessary. Oncological control and cosmetic needs can be optimised with skin-sparing or nipple-sparing mastectomy and immediate reconstruction. Prosthetic (implant) or autologous tissue (free transfer of tissue from abdomen, buttock or thigh, with microsurgical anastomoses or pedicle flap transfer from back) are routine reconstructive techniques. Delayed reconstruction is an acceptable option for women with inflammatory breast cancer, or locally advanced cancer, in patients needing radiotherapy after mastectomy and in women who need more time to consider their reconstructive options. Although highly valuable, patients need to understand the limitations of reconstruction (insensate, different to touch) and that a reconstruction will not replicate their original breast.
Breast reconstruction after mastectomy is more common in young women than in older women. The reasons for this are varied and include patient education, personal choice and beliefs, opportunity, financial considerations and out of pocket costs, availability in both public and private systems and excessive waiting times. The rates of reconstruction in Australia are low, however, disparities among all age groups need to be addressed.23,24
Axilla surgery
Surgical management of the axilla in young women with breast cancer is the same as for older women. There is a trend towards minimising axillary surgery in all patients to avoid morbidity such as lymphedema, chronic pain and functional arm disability. Sentinel node biopsy is the procedure of choice for the axilla. Extensive axillary surgery is being increasingly replaced by radiotherapy and systemic therapy.25
Radiation therapy
Radiotherapy is indicated postoperatively in all women undergoing breast conserving surgery. A boost may be given to the resection bed. The impact of radiotherapy on a conserved breast can be distressing for patients, as fibrosis may cause deformity, displacement of the nipple and size decrease in the treated breast, which may need to be remedied. The indications for postmastectomy radiotherapy, nodal irradiation and hypofractionation, although complex, are the same for all age groups. Young age is a recognised risk factor for higher local recurrence rates after mastectomy.26 When radiotherapy is anticipated after mastectomy, reconstructive options may need to be readdressed due to the impact of radiotherapy, particularly on implant reconstruction.
Adjuvant systemic therapy
Young age alone is not a reason to prescribe aggressive systemic therapy. The type of systemic therapy is determined, as with other age groups, by tumour characteristics such as size, receptor status (ER, PR and HER-2), grade, proliferation, nodal status, stage and patient comorbidity and preferences.
Chemotherapy
Gene expression signatures, which can be assessed using commercially available tests (such as the Oncotype Dx test), may, in some cases, be useful in selecting a treatment option by providing additional information regarding an individual’s risk of recurrence and predicting the benefit of adjuvant chemotherapy.27
Due to the tumour biology factors, most young women will need chemotherapy, and this can be given pre- or postoperatively. Neo-adjuvant chemotherapy (given before definitive surgery) aims to downstage the disease by reducing tumour size and eliminating unidentified low volume metastatic disease. It can provide an in vivo way to monitor disease response to chemotherapy agents and, in many cases, allows conservative surgery to be undertaken.
Immunotherapy
This is indicated for all women with HER-2-positive disease and either node-positive or high-risk node-negative disease. Trastuzumab is combined with chemotherapy in either the adjuvant or, increasingly, in the neo-adjuvant setting in young women.
Endocrine therapy
Endocrine therapy is offered to young women with endocrine sensitive tumours.28 Tamoxifen, a systemic oestrogen receptor modulator (SERM), is the usual treatment. Ovarian suppression or ablation (gonadotropin analogues, oophorectomy or ovarian radiation) can be added to tamoxifen. Endocrine therapy is usually prescribed for five years, but in some cases of high-risk disease, is extended to 10 years.
Aromatase inhibitors (AIs) are avoided in premenopausal women, even if the patient develops chemotherapy-induced amenorrhoea because of concerns that reduced oestrogen feedback to the hypothalamus and pituitary will stimulate gonadotropin release and ovarian stimulation, i.e. it may promote recovery of ovarian function. AIs cannot be used if functioning ovaries are present and producing oestrogen. AIs block the aromatase pathway, which is present in peripheral fat and not the ovaries.
Younger age is associated with lower treatment compliance with tamoxifen due to side effects, including hot flushes, sexual dysfunction, psychological problems, increased risk of thrombotic events and endometrial cancer.
Special considerations
Breast cancer during pregnancy
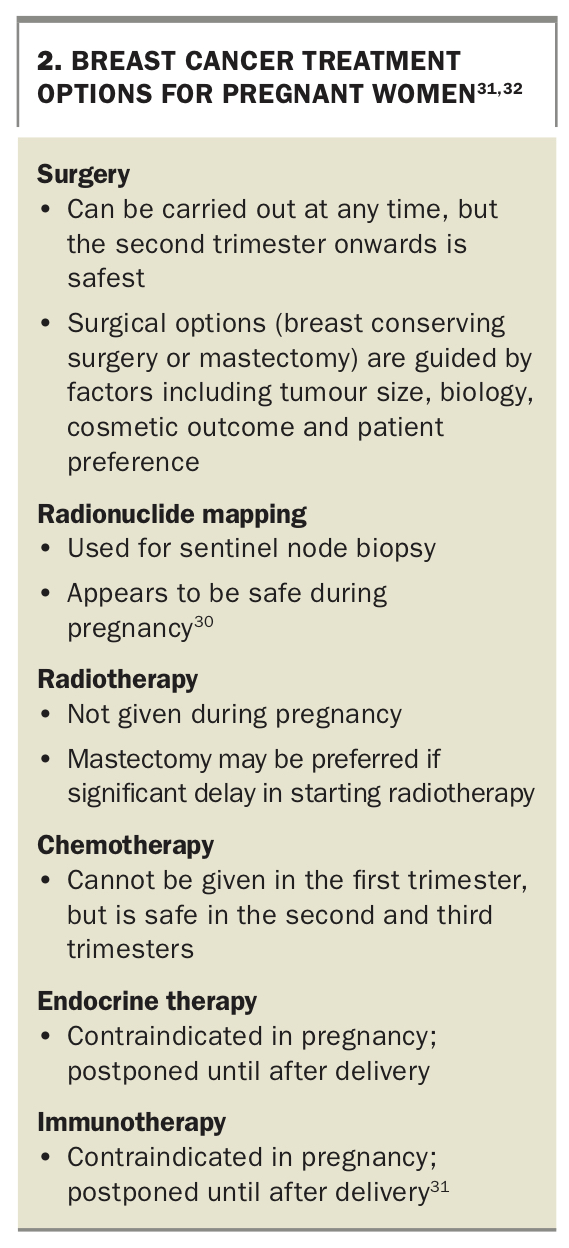
Breast cancer encountered during pregnancy is difficult to diagnose because of the hormonal effects of pregnancy on breast tissue causing increased density and lumpiness. These physiological changes can obscure pathological changes, leading to delayed presentation and diagnosis. Malignant pathology is confused for benign pathology, such as mastitis, and young patients often present with larger and more locally advanced cancer. Prognosis is similar to nonpregnant patients and breast cancer can be successfully treated during pregnancy.29 Termination is generally not advised, except in exceptional circumstances to allow cancer treatment to proceed rapidly. Diagnosis proceeds in the usual manner with ultrasound and biopsy. Mammogram is also possible with shielding of the uterus. Treatment options vary compared with nonpregnant patients and are listed in Box 2.30,31
{kind=link}
Fertility and fertility preservation
Fertility and family planning are major concerns for young women diagnosed with breast cancer.32 Young patients need to be counselled about the impacts of treatment on their fertility and the techniques available for fertility preservation, such as embryo, oocyte or ovarian tissue cryopreservation, as well as the role of ovarian function suppression with gonadotropin-releasing hormone agonists (GnRHa) during chemotherapy.6,33 Early referral, before the start of treatment, is needed to implement fertility preservation strategies.
Premature menopause
Chemotherapy may cause permanent or transient menopause and is related to the agents used, dose and patient age, with likelihood of menopause increasing with increasing age (40% at age 40 years). Symptoms of menopause may be particularly distressing for young women and a reason to stop endocrine therapy. Symptoms such as hot flushes, sleep disturbance, fatigue, weight gain and sexual dysfunction may be compounded by anxiety and depression, further affecting quality of life. Symptoms should be managed in a multidisciplinary setting that includes the use of pharmacological agents, such as antidepressants and vasomotor agents, and nonpharmacotherapies, such as acupuncture, mindfulness, meditation.
Bone health
Young women with breast cancer who experience chemotherapy-induced amenorrhoea also experience a decline in bone density.34 Tamoxifen may also cause bone loss in premenopausal women, despite being osteoprotective in postmenopausal women.10 General measures, such as doing regular weight bearing exercise and taking dietary supplements (calcium and vitamin D), should be emphasised. The use of bisphosphonates may be beneficial in reducing the rate of bone loss, and treatment is guided by degree of bone loss, as for older women.6
Future pregnancy and contraception
Pregnancy during active treatment is discouraged because of the risk of teratogenesis. Effective nonhormonal contraception, such as barrier methods, including condoms, copper intrauterine devices and partner vasectomy, should be considered.
Many young women will not have started or completed their family at the time of breast cancer diagnosis. Subsequent pregnancy shows no detrimental effect on breast cancer outcome in young women treated for breast cancer, including those treated for ER-positive disease.35 The timing of pregnancy after diagnosis should be discussed with the multidisciplinary team, particularly for patients with ER-positive disease, where treatment cessation of endocrine therapy is considered or required. Although pregnancy is possible after breast cancer, other difficult issues need to be confronted by the patient and their family, with particular thought given to impact on the family if the mother were to relapse and succumb to her disease.
Breastfeeding
Breastfeeding is usually not possible from the treated breast due to radiotherapy. The contralateral untreated breast may successfully produce breastmilk.
Psychosocial impact
The psychosocial impact of a breast cancer diagnosis on any woman cannot be overemphasised; however, young women are affected in a number of additional ways. They often have young families and are caring for young children. Premature menopausal symptoms, psychological issues such as anxiety and depression, anger, sadness and guilt, although understandable, may have a detrimental impact on relationships and family life. Roles within the family are often changed during treatment, as partners, who are also usually, young take on more responsibility as caregivers to children and a sick partner.
Depending on treatment regime and side-effects, time off work is often needed during treatment and may result in financial strain (from loss of income) and frustrations due to lost career and work opportunities, which may affect relationships and intimacy. Communication with children, who will often perceive that something is wrong, may be difficult for parents and needs special attention. Counselling and psychological support should therefore be available to all members of the family and provided by qualified and experienced clinicians.
Chemobrain and cognitive impairment
Neurocognitive symptoms are frequently reported by patients after chemotherapy, with symptoms lasting up to two years and affecting younger patients more severely.36 Forgetfulness, difficulty concentrating, fatigue, distractibility, poor attention and difficulty with word finding are reported. These symptoms may be so severe that they negatively impact daily functioning, which may affect the ability to work and career progression. Hormonal changes, chemotherapy-induced amenorrhoea and premature menopausal symptoms may also contribute cognitive decline after treatment, and further research is needed in this area.
Body image
The breast is extremely important in the expression of femininity and beauty for many women and is a vital part of body image. Body image and sexual identity are adversely affected in women undergoing treatment for breast cancer, particularly young women, with patients experiencing feelings of loss and sadness. Appropriate surgical techniques that optimise cosmesis while ensuring an oncologically safe procedure are emphasised, along with psychological support to help young women manage their emotional wellbeing as their body changes.
Sexuality
Sexual dysfunction is a major issue impacting the quality of life of young women diagnosed with breast cancer, including the quality of a couple’s relationship. Sexual dysfunction is multifactorial and impacted by chemotherapy-induced amenorrhoea, ovarian function suppression and endocrine therapy. Body image concerns, menopausal symptoms, fatigue, vaginal dryness, dyspareunia, decreased libido, anxiety, depression and the side effects of medications, including antidepressants, all contribute to sexual dysfunction and may result in treatment cessation.
As the cause is multifactorial, the management must be multifaceted. Psychological support and couples’ counselling may be necessary. Vaginal dryness can be managed with vaginal lubricants. Low-dose vaginal hormones have been shown to be safe and effective, but individual risk should be discussed with each patient's medical oncologist. Novel treatments such as vaginal CO2 laser have been reported to improve symptoms, but further trials are needed.37
Lifestyle changes
General lifestyle measures apply to all women with breast cancer and include regular exercise, weight loss, eating a low-calorie diet, smoking cessation and avoiding high alcohol intake.
Conclusion
Breast cancer in young women is rare. These women face a number of additional challenges. Multidisciplinary care, which includes the patient’s family physician, aims at optimising communication between all members of the treating team and allows issues in all aspects of management to be identified, and addressed early and efficiently. The ultimate aim of this approach is to ensure best practice, increase treatment success and decrease distress for the young woman during her breast cancer journey. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.