An introduction to field therapies for photoageing

Photoageing caused by chronic sun exposure manifests with skin changes such as rhytids, lentigines, coarse texture and neoplasia. A wide range of field therapies are available to address visible signs of photoageing and, potentially, subclinical photodamage. These include sunscreens for primary prevention, topical retinoids and alpha-hydroxy acids, cancerised field therapies, chemical peels, and laser and other light and infrared therapies.
- Photoageing caused by chronic exposure to ultraviolet radiation is responsible for about 80% of facial ageing and manifests as rhytids, lentigines, coarseness and neoplasia.
- A broad range of field therapies that target photoageing are available, with options for all skin phototypes.
- Alpha-hydroxy acids promote skin desquamation and cell growth and stimulate collagen production; they can decrease fine wrinkling and lighten solar lentigines.
- Topical retinoids increase epidermal cell turnover and restore the dermal extracellular matrix; they can improve dyschromia and fine and coarse wrinkling.
- The ablative resurfacing laser, traditionally regarded as the gold standard for managing photoageing, has considerable side effects and downtime.
- Fractional and nonablative rejuvenation and radiofrequency techniques allow regimens with shorter healing times and fewer side effects, suitable for a wider range of skin phototypes.
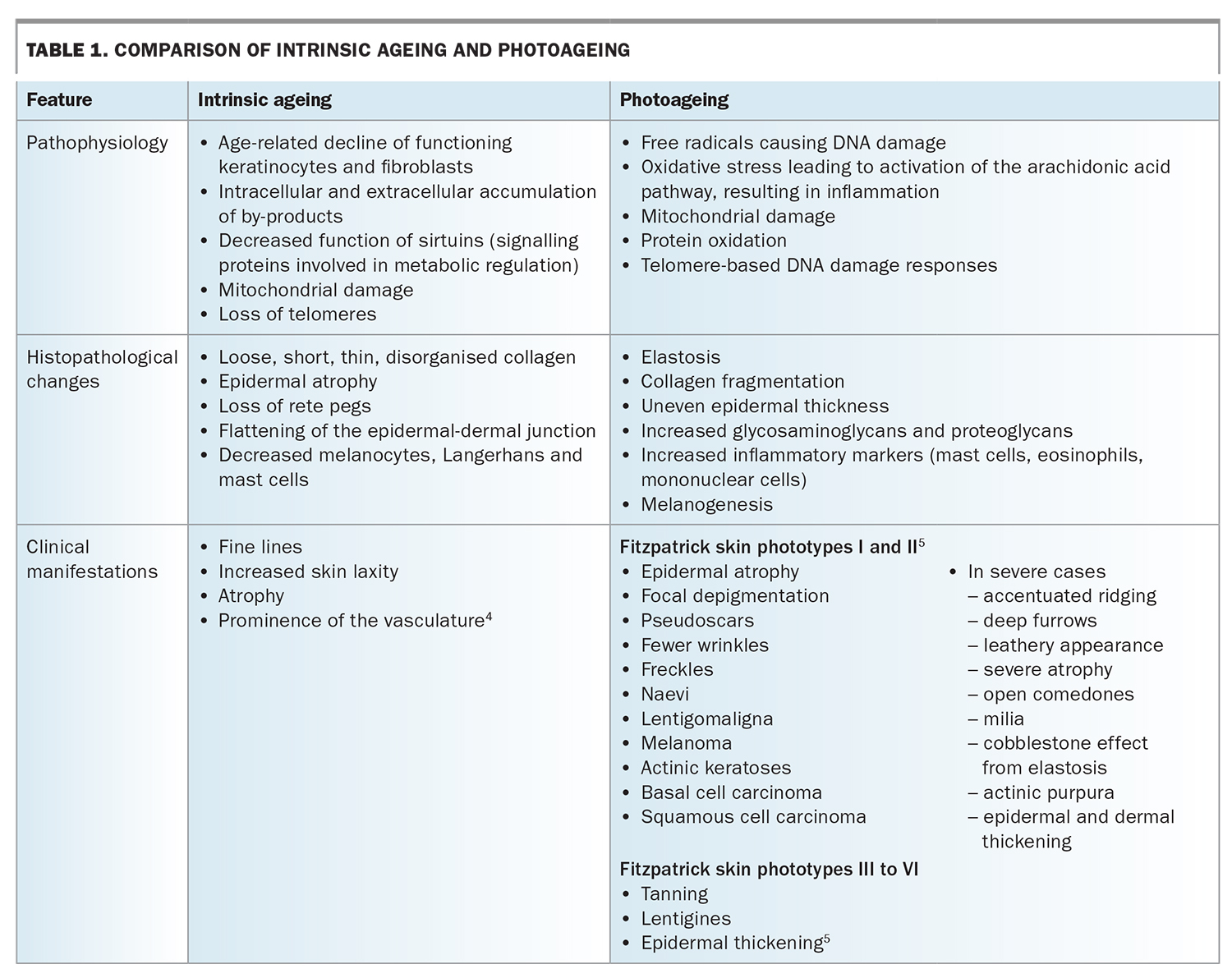
For over 1000 years, many techniques have been used to treat the effects of time on the skin.1 With an ageing population and a global market for antiageing products estimated at over $40 billion, public and scientific interest in therapies to maintain a youthful appearance has grown. Skin ageing is classified into two categories: intrinsic ageing and photoageing. Intrinsic skin ageing is influenced by genetics and results from the age-dependent deterioration of skin function and structure, such as epidermal atrophy and collagen reduction.2,3 Photoageing is characterised by chronic exposure of the skin to sunlight, particularly ultraviolet (UV) radiation. Its manifestations include rhytids, lentigines, coarse texture, laxity, sallowness, neoplasias and telangiectasias, depending on skin types and ethnicity.2 The features of intrinsic ageing and photoageing are compared in Table 1.4,5
{kind=link}
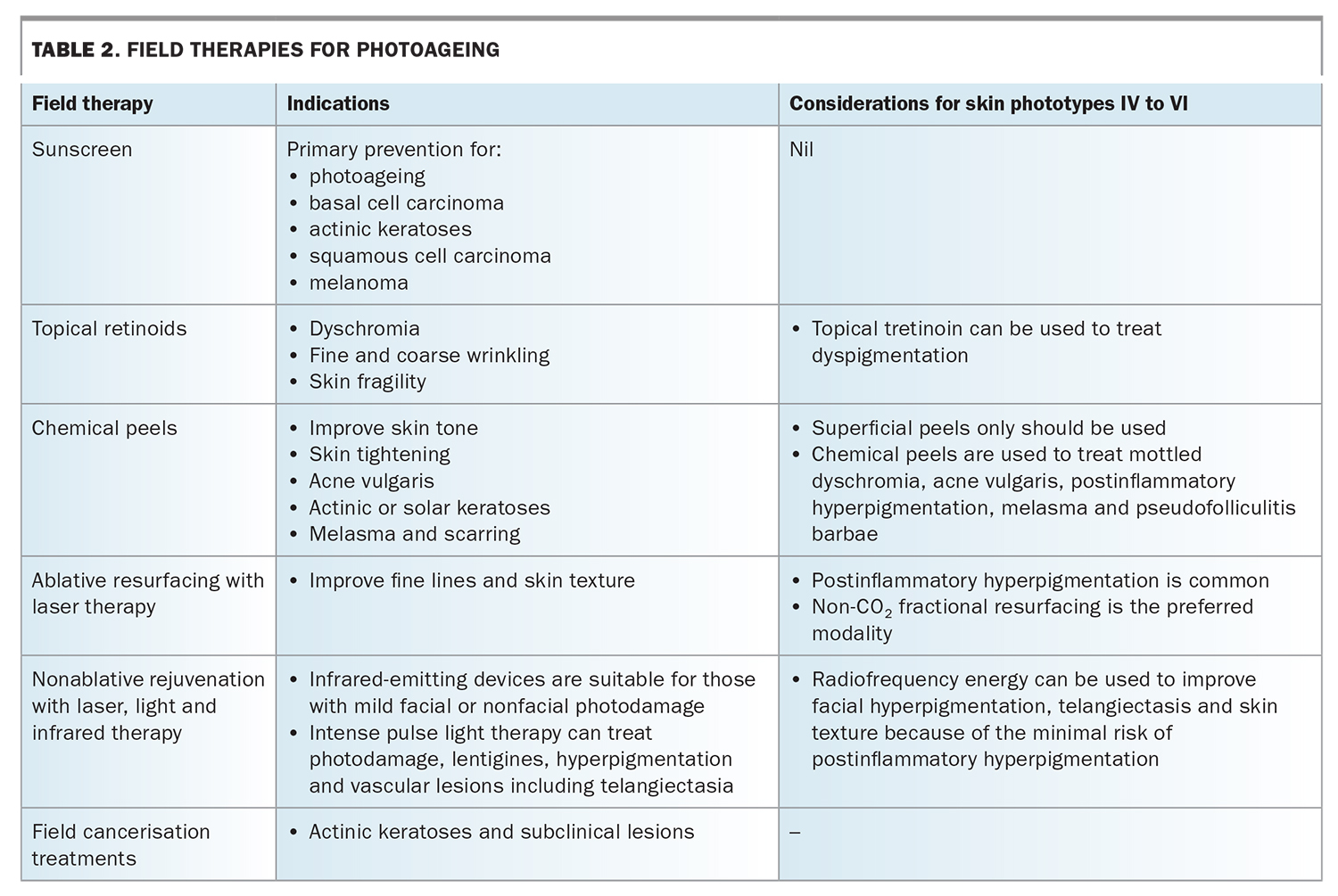
A broad range of field therapies to target photoageing are available. These are defined as treatments that address the visible signs of photoageing and potentially subclinical photodamage. Field therapies for photoageing include topical therapies, cosmeceuticals, chemical peels and laser, light and other nonlaser modalities, with options for people of all skin phototypes. This article introduces clinicians to the general concepts of photoageing and some of the main field therapies available (summarised in Table 2).
{kind=link}
Pathogenesis of photoageing
The term photoageing was first coined in 1986 and was used interchangeably with the term ‘dermatoheliosis’, erroneously implying a pathological condition of the sun.4 Both UVA and UVB radiation are involved in the photoageing process. However, UVA has a significant role, as it penetrates more deeply into the dermis and reaches the earth’s surface in 10 times greater quantity than UVB.4
Sun exposure is thought to be responsible for 80% of facial ageing.3 UV irradiation of the skin produces reactive oxygen species, which activate growth factors and receptor-initiated signalling to induce a transcription factor, activator protein 1 (AP-1). Increased AP-1 activity decreases synthesis of dermal collagen and keratinocyte proliferation.
UV irradiation also stimulates the expression of metalloproteinases, which degrade extracellular matrix proteins such as collagen, fibronectin, elastin and proteoglycans.6 UV-induced collagen degradation leads to the accumulation of partially degraded collagen fragments in the dermis, reducing the structural integrity of the skin.5 Further, continuous generation of reactive oxygen species injures the mitochondria, compromising their function and exacerbating collagen degradation and skin photoageing.4,5 UV irradiation can also cause cellular protein oxidation, inhibiting proteasomal function and interfering with the effective degradation of defective proteins.
Telomeres are also susceptible to UV damage, triggering tumour suppressor protein p53 and other DNA damage response proteins to induce proliferative senescence or apoptosis. This may explain the features shared by photoageing and chronological ageing.3,5
Visible light and infrared radiation may also contribute to photoageing. Visible light is a substantial constituent of the solar spectrum but is suggested to contribute to less than 10% of total DNA damage caused by solar exposure, and infrared radiation generates reactive oxygen species in the skin. However, further research is needed on the role of visible light and infrared radiation in photoageing.7
Clinical manifestations of photoageing
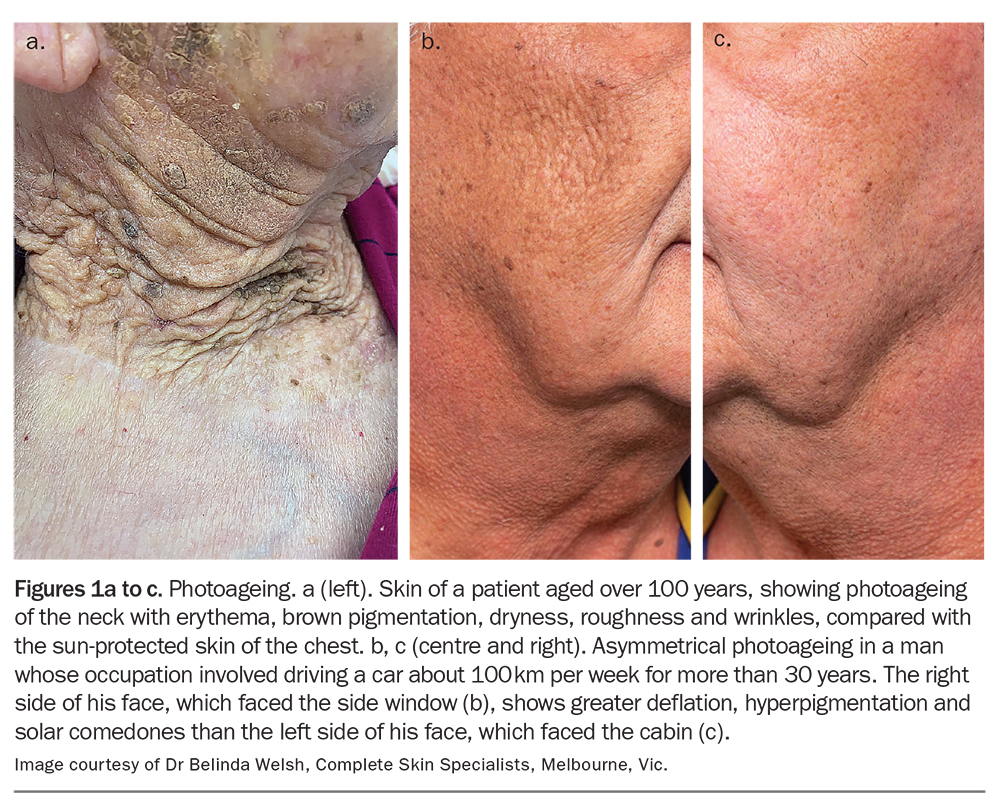
The clinical manifestations of photoageing vary with skin type and ethnicity. Photoageing is more prominent in fair-skinned individuals and less discernible in those with Fitzpatrick skin phototypes IV and higher (Table 1).6 Individuals with skin phototypes I and II show atrophic skin changes, with guttate hypomelanosis, lentigines and premalignant changes such as actinic keratoses and epidermal malignancies but fewer wrinkles (Figures 1a to c). Those with skin types III and IV tend to develop hypertrophic responses, such as deep wrinkling, coarseness, leathery appearance of the skin and lentigines.5,8 They also tend to experience photoageing effects 10 to 20 years later than their type I and II counterparts, and the effects are less severe because of the added photoprotection of darker skin.4
{kind=link}
Photobiologic scoring of photoageing
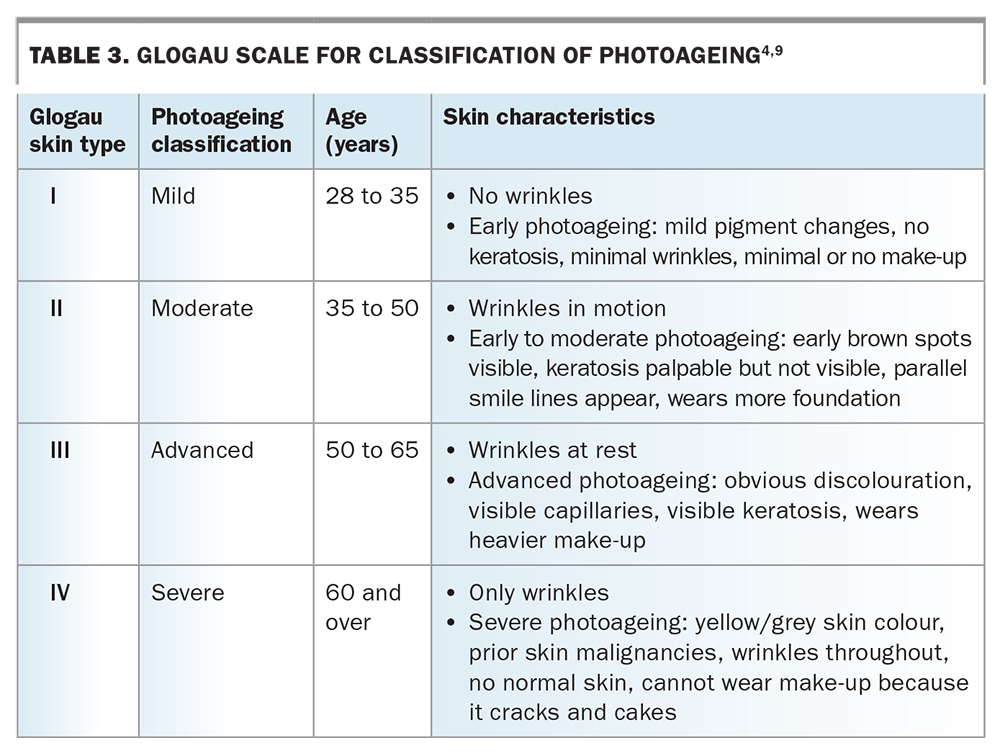
Evaluating the level of photodamage in a patient is crucial for determining a treatment plan and assessing treatment response. Several scales have been developed to quantify the severity of photoageing. The Glogau scale is an established tool that grades photoageing as mild, moderate, advanced or severe. This scale relies predominantly on the extent of rhytids in its classification (Table 3).4,9 Generally, patients with higher Glogau scores can receive more intensive treatments but have higher complication rates. The Glogau scale does not factor in skin type, which also influences complication rates.4,9
{kind=link}
Other tools to quantify photoageing include the photonumeric nine-point scale of Griffiths and colleagues and a validated grading scale by Carruthers and Carruthers that rates forehead lines, brow positioning elemental folds and crows’ feet.5 The Wrinkle Severity Rating Scale and Global Aesthetic Improvement Scale are used in clinical research studies to quantify facial folds.4
Treatments for photoageing
Sunscreens
Sunscreens have a long history; ancient Greek athletes applied a mixture of oil and sand to protect their bodies from the sun when training for the Olympic games.7 Regular use of broad-spectrum sunscreens, which block UVA and UVB, is the first line of defence in the prevention of photoageing. Sunscreens should be used in conjunction with other photoprotective measures, such as seeking shade when outdoors, wearing sun-protective clothing and avoiding exposure to both natural and artificial sources of UV light.4
Sunscreens provide temporary protection against UV radiation through organic filters such as avobenzone that absorb UV light or inorganic filters such as zinc oxide and titanium oxide that absorb, reflect and scatter UV light. Studies have shown that daily sunscreen application can prevent the development of actinic keratoses, basal cell carcinoma, squamous cell carcinoma and melanoma, lessen the signs of premature ageing and prevent exacerbations of photodermatoses such as polymorphous light eruption.10
In Australia, it is recommended that sunscreen with a sun protection factor (SPF) of 30 should be applied 20 minutes before going outdoors. One teaspoon of sunscreen should be applied per limb, with a full-body application for an adult requiring at least 35 mL or around seven teaspoons.11
Topical retinoids
Retinoids are a family of substances containing vitamin A (retinol and its natural and synthetic derivatives). Topical retinoids were first used in dermatology around 80 years ago to treat acne vulgaris, and their use has since expanded to treat other skin conditions, including photoageing.12 Retinoids bind to nuclear retinoic acid receptors and exert their effects by modulating cellular differentiation to increase epidermal proliferation, compaction of the stratum corneum, and biosynthesis and deposition of glycosaminoglycans. Retinoids can also inhibit dermal matrix degradation after sun exposure and block induction of AP-1 and AP-1-regulated metalloproteinases.5
Topical retinoids have been shown to improve dyschromia, fine and coarse wrinkling, and skin fragility and to exert an anti-inflammatory effect.12 Additional short-term histological effects include improvement of atypia and dysplasia.13
Types of topical retinoids
Topical retinoids are classified by molecular structure as first-generation (retinol, tretinoin, retinaldehyde), second-generation (acitretin, etretinate), third-generation (adapalene, tazarotene) and fourth-generation (seletinoid G).
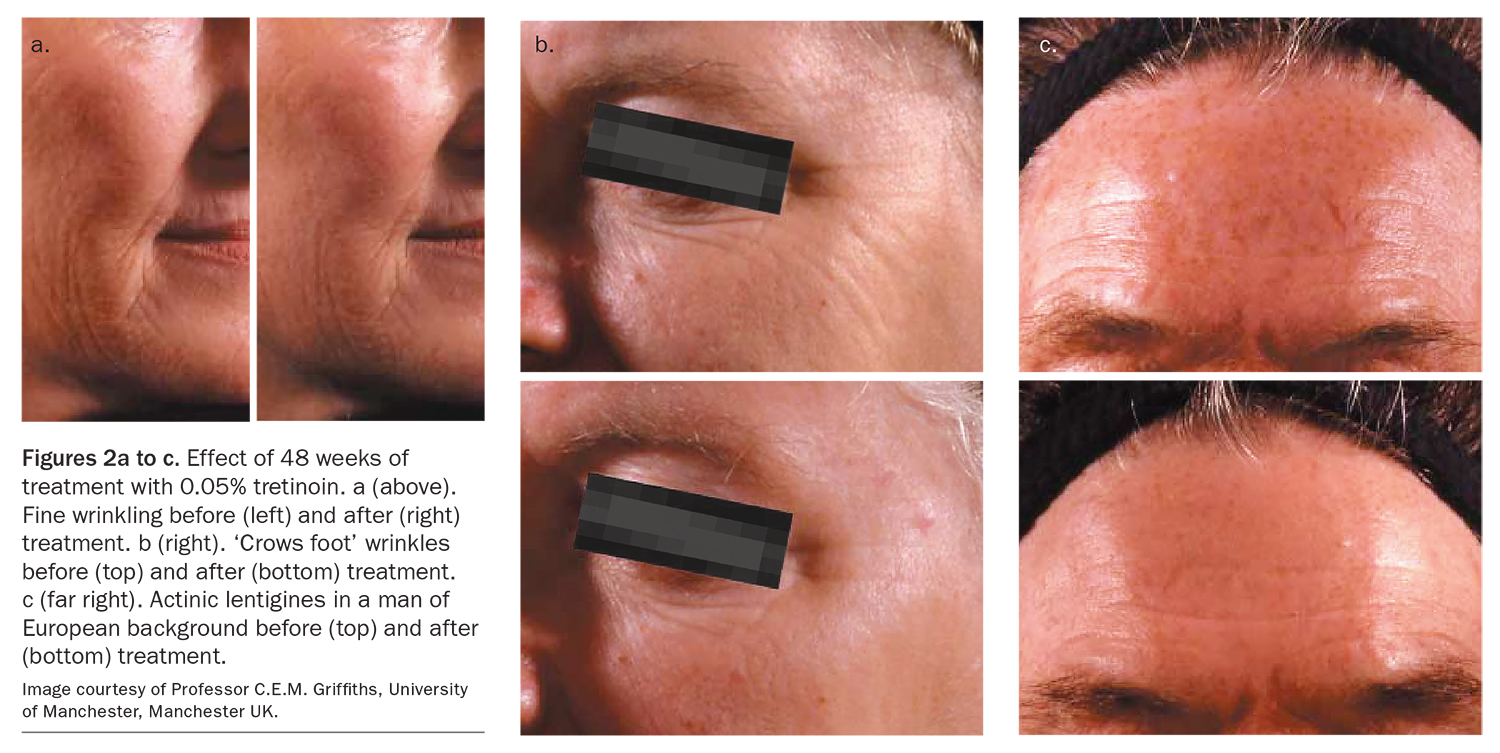
Tretinoin is the most researched compound for the treatment of intrinsic ageing or photoageing.14 It is available on prescription in 0.025% and 0.05% strengths. Tretinoin 0.05% cream has proven long-term efficacy and safety (Figures 2a to c). Low-strength tretinoin (0.025%) is also quite effective while being more tolerable. The benefits of tretinoin are dose-dependent and increase with the duration of therapy for at least 10 to 12 months. Cessation of treatment results in some clinical deterioration.15,16 Thus, most clinicians recommend initial treatment once daily at night for six to nine months, followed by a long-term maintenance, maybe at a lower concentration or reduced frequency (alternate days).17
{kind=link}
Tazarotene 0.1% gel, available in the USA, is also effective in improving skin hydration and reducing skin texture and fine wrinkling. It may have a faster effect than 0.05% tretinoin.18
Retinols and retinaldehyde are available in several over-the-counter preparations. Retinol has been estimated to be 10 times less potent than tretinoin, and factoring this, studies comparing retinol and tretinoin have shown similar clinical benefits in photoaged skin.12 Retinaldehyde has been shown to improve fine and deep wrinkles when compared with 0.05% tretinoin, with less irritation.12
Clinical use of topical retinoids
Importantly, the benefits of topical retinoids may be seen only after a couple of months of use, and diligent, concurrent use of sunscreen and moisturiser to prevent irritation is recommended.19 Topical retinoids have photosensitising and irritating effects and hence should only be applied at night and washed off in the morning. Daily use of sunscreen with SPF 15 or higher before going outdoors and avoidance of strong sunlight if unprotected are recommended. Irritation can be minimised by the application of a moisturiser after topical retinoid therapy and by introducing slowly and increasing to a nightly application as tolerated. Clinicians should be aware that topical retinoids are teratogenic and should not be used by women who are planning to become pregnant or who are pregnant or breastfeeding.20
There are few data on the use of topical retinoids for photoageing in darker-skinned individuals. A small 40-week trial in people of Japanese or Chinese background found that once-daily application of 0.1% tretinoin cream significantly lightened hyperpigmentation in 90% of those in the treatment group, compared with 33% of those receiving a vehicle cream.21 Hence, topical tretinoin may be indicated to treat dyspigmentation, a common manifestation of photoageing in individuals with darker skin pigmentation. However, in people with sensitive skin types, the exfoliative properties of retinoids can cause dryness and irritation, leading to postinflammatory responses that can worsen hyperpigmented lesions or patches.
Assessment of a patient’s skin type, use of skincare and haircare products, cleansing techniques and history of irritation with dermal treatment can aid in deciding the best retinoid treatment regimen. Generally, the newer third- and fourth-generation retinoid formulations may be less irritating than older gel or cream formations, while offering the same level of efficacy.22
Topical alpha-hydroxy acids
Alpha-hydroxy acids (AHAs) are a class of organic acids commonly used in cosmetics and dermatology.23 AHAs are found naturally in foods such as dairy products (lactic acid), fruit (malic acid and citric acid) and sugar cane (glycolic acid).24 The ancient Egyptian queen Cleopatra was reported to have bathed in sour milk, which contains lactic acid, to smooth her skin and make her appear more youthful.25,26
The precise mechanism of action of AHAs is not fully defined. However, AHAs are hypothesised to affect the epidermis and dermis by reducing the pH, thereby inhibiting transferases and kinases, reducing calcium ion concentration and promoting desquamation and cell growth.24 Studies have also shown that glycolic acid accelerates collagen synthesis and epidermal turnover while modulating matrix degradation and inhibiting melanin formation through antityrosinase activity.27 The extent of the exfoliative effect of AHAs is determined by the concentration and pH of the product.
AHAs are often present at lower concentrations (4 to 20%) in nonprescription creams and gels for long-term application on aged skin and also in cleansers, moisturisers, toners, masks and age-spot removers. AHAs at higher concentrations (over 20%) are often used in chemical peels applied by dermatologists, as described below (Chemical peels).28
Research on the effectiveness of low-concentration AHAs is limited. However, a study of 8% glycolic acid or lactic acid applied daily over 22 weeks found that more than 70% of patients reported a noticeable improvement in the appearance and texture of photoaged skin.25 Daily application of 12% lactic acid for three months was also shown to increase epidermal and dermal firmness and thickness.25 The effect of AHAs on photoageing is not as well established as that of retinoids, and there is no evidence that high-cost creams with or without AHAs are more efficacious than low-cost creams.24,29 Long-term effects of AHAs on the rate of exfoliation are unknown, although the skin may develop tolerance to the stimulatory effect of AHAs in cell shedding.28
Adverse reactions to AHAs depend on their pH and concentration, but daily application of a concentration of up to 20% is generally well tolerated in patients with normal skin. Patients should still be informed of the potential side effects of skin irritation, stinging, photosensitivity from exfoliation of the stratum corneum, pain and erythema.23,24
Research into AHAs led to the discovery of polyhydroxy acids. These include lactobionic acid, which has similar effects to AHAs with a better side-effect profile.27
Field cancerisation treatments
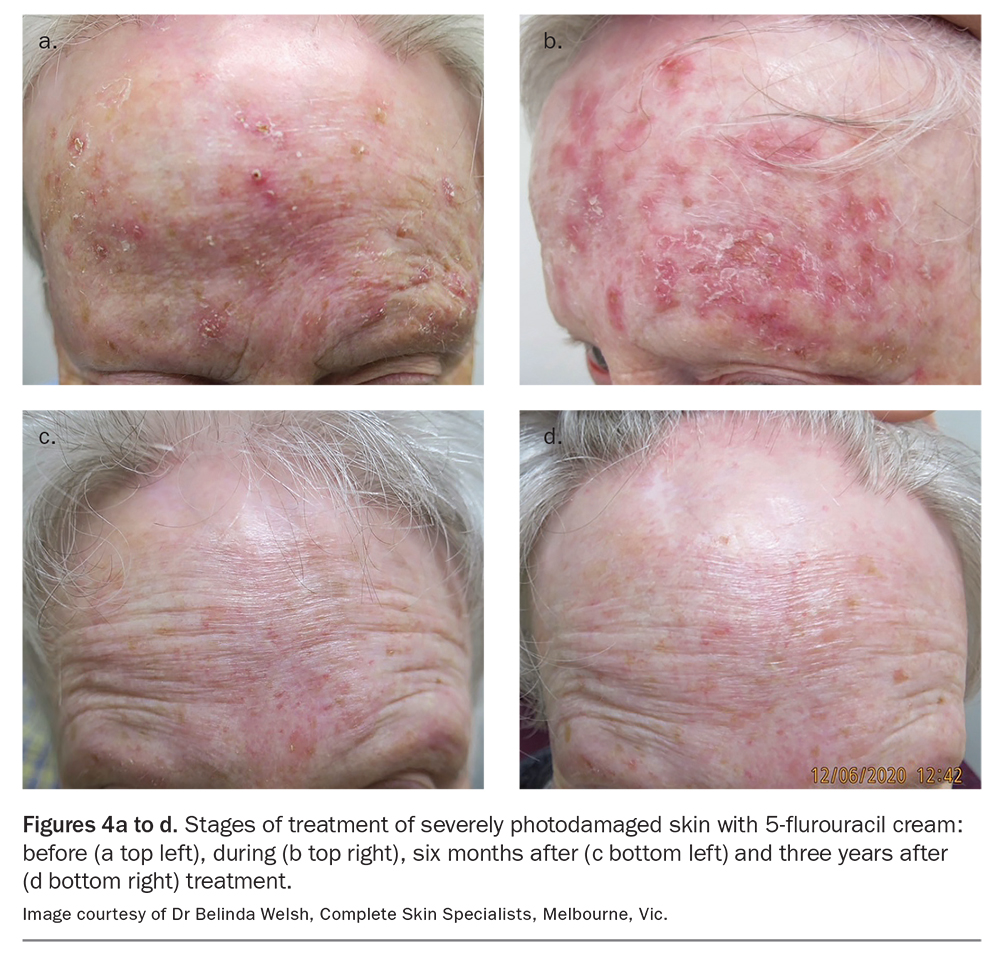
Precancerous changes and actinic keratosis are components of photoageing. Field treatments are available that aim to treat both visible and subclinical lesions, termed the ‘cancerised field’.30 These treatments include, but are not limited to, 5% fluorouracil cream, 5% fluorouracil chemowraps, 4%
5-fluorouracil cream, 5% topical imiquimod, 3% diclofenac in 2.5% hyaluronic acid gel, photodynamic therapy, dermabrasion and oral chemoprophylaxis agents (Figure 3 and Figures 4a to d).31
{kind=link}
{kind=link}
Chemical peels
First documented in ancient Egypt, superficial and medium-depth chemical‘peels’ are safe, effective clinic-based procedures used to treat photoageing by wounding the skin with a caustic substance. Chemical peels cause partial or complete destruction of the epidermis or dermis, resulting in subsequent exfoliation, regeneration and remodelling of the layers, leading to improved skin tone and skin tightening.1,4 Chemical peels can also be used to treat acne vulgaris, actinic or solar keratoses, melasma and scarring.1 Patients should not be offered a chemical peel if they have an active infection, open wound, history of allergy to a peeling ingredient, recent isotretinoin therapy (unless being treated with a superficial chemical peel) or if they are pregnant.1
Types of chemical peel
Chemical peels are classified according to the depth of skin affected as superficial, medium or deep. Superficial peels target the epidermis and the epidermal-dermal interface and cause basal keratinocyte renewal and reactive inflammation that stimulates neocollagenesis.32 Clinicians can use a superficial peel to treat mild photoageing. Examples of superficial peel agents include 10 to 30% salicylic acid, 20 to 70% glycolic acid, Jessner’s solution and trichloroacetic acid at a concentration less than 20% .
Medium-depth peels target the entire epidermis and papillary dermis, and even the upper reticular dermis, causing skin regeneration from the follicular epithelium. Medium-depth peels are used for moderate photoageing (Figures 5a to c).
{kind=link}
Deep peels penetrate the midreticular dermis, causing intense collagen synthesis and protein coagulation, which is clinically observed as frosting.32 They are suitable for severe photoageing and are best for skin phototypes I and II.26 Deep peels are rarely used and should be performed only by experienced clinicians because of the high risk of side effects such as hypopigmentation, demarcation, scarring and (in the case of phenol) cardiac effects. Examples of deep chemical peeling agents include trichloroacetic acid at a concentration over 50% and the Baker-Gordon formula, containing phenol and croton oil.1,4,32
Chemical peels and darker skin
Special considerations apply to the use of chemical peels in people with Fitzpatrick skin phototypes IV to VI. In this group, chemical peels are not generally used to treat photoageing but rather for mottled dyschromia, acne vulgaris, postinflammatory hyperpigmentation, melasma and pseudofolliculitis barbae.
Superficial peels are well tolerated by those with darker skin. However, clinicians should avoid medium-depth and deep peels because of the high risk of disfiguring, long-term postinflammatory pigment changes or hypopigmentation from an unpredictable response of melanocytes to injury.26 The risk of postinflammatory pigment changes can be reduced by meticulous procedure planning (such as starting with a low-potency peel and titrating up) and close monitoring after treatment. Treating prolonged erythema with emollients and topical corticosteroids can help to avoid dyschromia.26
Ablative skin resurfacing with laser
Ablative laser skin resurfacing is the process by which the epidermal and superficial dermal layers of the skin are removed to minimise the signs of photoageing. Ablative skin resurfacing is also used to treat scarring, actinic keratoses, seborrhoeic keratoses and facial wrinkles.33
Laser ablation for facial rejuvenation started with the continuous carbon dioxide (CO2) laser in the 1980s. For a time, this was regarded as the gold standard for the treatment of photoageing. The CO2 laser produces an invisible beam that emits energy at a wavelength of 10,600 nm, which is primarily absorbed by water, the most abundant chromophore in the skin. The delivered light energy contracts the skin immediately by denaturing collagen, which subsequently stimulates the production of new collagen. The CO2 laser can markedly improve rhytids, dyspigmentation and skin laxity but best targets fine wrinkles around the eyes and mouth.4,34 Nonetheless, because of the difficulties in controlling tissue-dwell time, CO2 lasers were prone to excessive thermal diffusion and unintended tissue damage, leading to a high risk of char formation, pigment changes, fibrosis, scarring and prolonged recovery.4,35
The subsequent development of the erbium:yttrium aluminium garnet (Er:YAG) laser allowed greater precision and depth of cutaneous ablation, with a reduced side-effect profile.35 Like CO2 lasers, Er:YAG lasers act on water but energy absorption is 12 to 18 times greater, leading to complete ablation of tissue with little thermal damage.36 Er:YAG lasers have less of a skin tightening effect than CO2 lasers but may be preferred by dermatologists to treat dyschromia and fine wrinkles or areas with a high risk of scarring, such as periorbital skin. Er:YAG laser therapy has a shorter recovery period, less postoperative oedema and fewer side effects.34,37
Because of the high risk of side effects with ablative lasers, they should be used only by experienced clinicians and in people with Fitzpatrick skin type I (the latter because of the risk of relative hypopigmentation). Anaesthetic techniques such as eutectic mixture local anaesthetics (EMLA) cream, regional nerve blockade for cosmetic units and intravenous sedation or general anaesthesia for the full-face ablative laser are needed to ensure patient comfort during epidermal ablation and dermal heating.38
Fractionated laser and radiofrequency therapy
The prolonged postoperative recovery time and significant risk of side effects with traditional ablative laser therapy prompted the development of fractionated therapies in the 2000s. Fractional laser therapy uses narrow columns of laser light to create microscopic thermal zones surrounded by islands of healthy tissue, allowing rapid re-epithelisation and healing.39
Ablative and nonablative fractionated lasers
Fractional laser therapy can be ablative or nonablative. Ablative fractionated lasers are effective in treating dyspigmentation, skin laxity, skin rhytids and atrophic acne scarring, and their use is significantly safer than conventional ablative resurfacing (Figure 6). However, there is still a high risk of complications in the form of scarring, discolouration and skin infection. Ablative fractionated lasers include the 10,600 nm fractional CO2 laser, 2940 nm fractional Er:YAG laser and the 2790 nm fractional erbium:yttrium scandium gallium garnet (Er:YSGG) laser.
{kind=link}
Nonablative fractionated lasers combine the safety and gentleness of fractionated and nonablative technologies, delivering narrow beams of high-energy light at differing wavelengths to target tissue water, leaving the stratum corneum intact. Nonablative fractional laser therapy can improve skin texture, wrinkling, dyspigmentation and telangiectasia and can safely treat the neck, chest and extremities. Examples include the 1410 nm laser, 1440 Nd:YAG laser and 1540 nm pulsed laser.
Although ablative fractionated lasers can be more effective than nonablative fractionated devices at improving fine lines and skin texture, they typically produce more discomfort and have a longer recovery time. For these reasons, nonablative fractionated lasers have increased in popularity for the treatment of photoageing. These lasers are also effective in darker-skinned individiuals with reduced risk of pigment changes.
Skin tissue contraction after fractional resurfacing has been shown to persist for a minimum of one year after the procedure.39 Operators may use topical anaesthetics alongside nerve blocks or intralesional anaesthesia for procedures involving broad regions, such as the central forehead.33
Fractionated radiofrequency devices
Fractionated radiofrequency devices deliver another type of fractionated therapy that uses deep dermal heating in an inverted-cone distribution. These devices are used for photoageing treatment, skin tightening and reduction of rhytids and scars. As radiofrequency energy does not target epidermal melanin, it can be used to treat all skin types (see below). Radiofrequency devices are safe and effective with no patient downtime.40
Facial resurfacing and darker skin
A common complication of facial resurfacing in patients with darker skin is postinflammatory hyperpigmentation. In some cases, hyperpigmentation can occur three to four weeks after treatment and persist up to six to nine months.15 The rate of postinflammatory hyperpigmentation increases with the energy and density of the treatment but is often unpredictable. Hence, it is crucial to start with conservative settings in patients with skin of colour.
Non-CO2 fractional resurfacing is the preferred modality for people with skin phototypes IV to VI, as CO2 laser use carries a higher risk of laser-induced dyspigmentation.33,34 Counselling and implementation of a pretreatment topical regimen consisting of sunscreen and prophylactic topical hydroquinone or topical retinoids are essential for all patients undergoing facial resurfacing. Strict sun avoidance before the procedure and for several weeks or months afterwards is crucial.
Treatment of delayed onset hyperpigmentation involves broad-spectrum sunscreen, topical bleaching agents such as hydroquinone or light glycolic acid peels. Other bleaching agents such as kojic acid and azelaic acid may also be helpful for long-term management of postinflammatory hyperpigmentation.9
Nonablative rejuvenation with laser, light and infrared therapy
The undesirable adverse effects and long recovery time after ablative therapies led to the development of nonablative laser, light and other energy-emitting devices. These devices were initially designed for managing vascular and pigmented abnormalities but have been adapted for skin rejuvenation.5,41 Nonablative treatments selectively damage the dermal tissues, leaving the epidermis intact, and are associated with less morbidity and downtime.33,42
Most nonablative systems emit light in the infrared range of the electromagnetic spectrum and target water molecules. Examples include the infrared nonablative 1320 nm Nd:Yag laser, 1450 nm diode laser and 1540 nm Er:glass laser. These are suitable for people with mild facial or nonfacial photodamage.43,44 Most studies report clinical improvement in facial and nonfacial rhytids of 30 to 50% after a series of these nonablative laser treatments.44
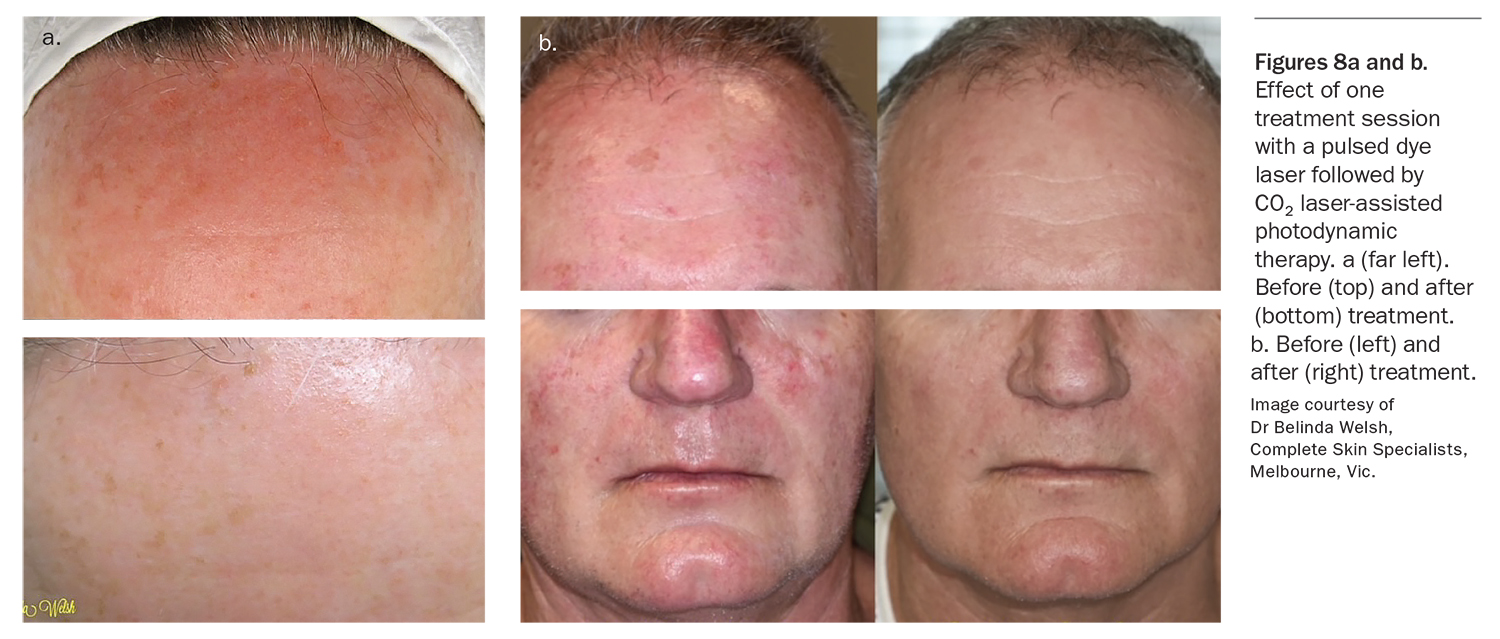
Pulsed dye lasers are considered the treatment of choice for cutaneous vascular disorders. These lasers emit visible (yellow) light, which is selectively absorbed by oxyhaemoglobin and can treat facial telangiectasias, port-wine stains, haemangiomas and vascular growths (Figure 7). Off-label uses of pulsed dye lasers include treating rhytids, actinic keratosis and Bowen’s disease (Figures 8a and b). Side effects include transient purpura, hyperpigmentation and atrophic scarring.45
{kind=link}
{kind=link}
Another type of nonablative device uses intense pulsed light (IPL). This is not a laser but a polychromatic flashlamp-based device used to treat vascular and pigmented lesions.43,46 It emits light in the 500 to 1200 nm wavelength range and is useful in treating large regions and the decolletage area.47 The indications for IPL therapy include photodamage, lentigines, hyperpigmentation and vascular lesions including telangiectasias. Long-term IPL treatments have been linked to youthful changes in gene expression and retardation of skin ageing. IPL devices are used mainly in patients with skin phototypes I to III and are generally avoided in darker-skinned patients because of the risk of epidermal injury and melanin chromophore competition.47
Special considerations for skin phototypes IV to VI
The development of the novel radiofrequency device to deliver energy in electrical current mode has added to the armamentarium of photoageing therapies for different skin types. Its main advantage is the minimal risk of postinflammatory hyperpigmentation in darker skin types. The radiofrequency device relies on the electric property of the target tissue, as the impedance of subcutaneous fat to electric currents generates heat. This leads to an immediate tightening effect from collagen contraction and long-term neocollagenesis.36
A comparative study examining the efficacy of radiofrequency, IPL and carboxy therapy in 60 patients (16 with skin phototype IV) resulted in a statistically significant decrease in Glogau score after intervention in the radiofrequency treatment group.48 Radiofrequency energy can also be combined with optical energy such as IPL to improve facial hyperpigmentation, telangiectasias and skin texture.49
Conclusion
Many interventions are available for the management of photoageing. These include topical therapies, chemical peels and laser, light and other nonlaser treatments. The development of fractional and nonablative rejuvenation and radiofrequency techniques has allowed regimens with shorter healing times and reduced side effects that are suitable for a wider range of skin phototypes. The Glogau Scale for severity of photoageing is a useful tool in treatment planning. Clinicians should consider the patient’s goals, severity of photoageing and skin phototype when referring patients for photoageing therapy. MT
COMPETING INTERESTS: Associate Professor Shumack is an investigator and advisory board member for Leo Pharma and Sanofi. Dr Lai: None.
Acknowledgement
The authors wish to thank Professor C.E.M. Griffiths, University of Manchester, UK, and Dr Belinda Welsh, Complete Skin Specialists, Melbourne, for providing clinical photographs.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.