Maxillofacial fractures in general practice

Maxillofacial fractures are a common presentation within general practice, particularly fractures associated with low-impact trauma, and in rural and remote settings. Recognising the key clinical features of different types of maxillofacial fractures and red flags for urgent referral can help GPs investigate and manage patients with these injuries.
Maxillofacial trauma, including facial fracture, is a common presentation to Australian emergency departments and general practices, with such injuries associated with significant morbidity. As a result, identification and referral to an appropriate surgical unit is crucial to the optimal management of patients presenting with these injuries. This article outlines the key features of maxillofacial fractures that may be seen in general practice, and the role of the GP in their identification and management. An example case study of how to assess and manage a patient with maxillofacial trauma in rural general practice is shown in Box 1.
{kind=link}
Prevalence of maxillofacial fractures
Epidemiological review of maxillofacial fractures shows a predominance within the male population (up to 80%), with a significant grouping of patients within the younger age bracket (15 to 24 years).1,2 Of relevance to presentations in general practice, overall rates of maxillofacial fractures increased in recent years, with the leading causes of injury comprising direct facial trauma (including sporting injuries and assault) and falls, followed by motor vehicle accidents and transport accidents (nonmotor vehicle accidents).1,3 Because of variations in the cause and extent of such injuries, presentation to a GP in the first instance is not uncommon.
The most common maxillofacial fracture is that of the nasal bone (55.8%). Other significant sites of fracture include the zygomatic and maxillary bones, orbit and mandible, with closed fractures presenting at significantly greater rates than open fractures.1
History and assessment
In the setting of a traumatic presentation, early assessment to identify life-threatening injuries is paramount. A primary survey using the following ABCDE framework can identify significant concerns:
- airway maintenance with cervical spine protection
- breathing and ventilation
- circulation with haemorrhage control
- disability and neurological status, including the Glasgow Coma Scale score
- exposure and environment.4
Patients identified as being unstable should be urgently transferred to an appropriate tertiary hospital for management. For patients who are stable, a prompt and systematic approach to information gathering must be used, such as the SAMPLE method:
- signs and symptoms
- allergies
- medications
- past illness
- last meal
- events and environment related to injury (including mechanism of injury).
A detailed history using collateral sources can be collected after further assessment. Key examinations relevant to maxillofacial trauma involve head and neck examination, including ophthalmological assessment, cranial nerve examination and examination of the oral cavity.
Presentation of facial fractures
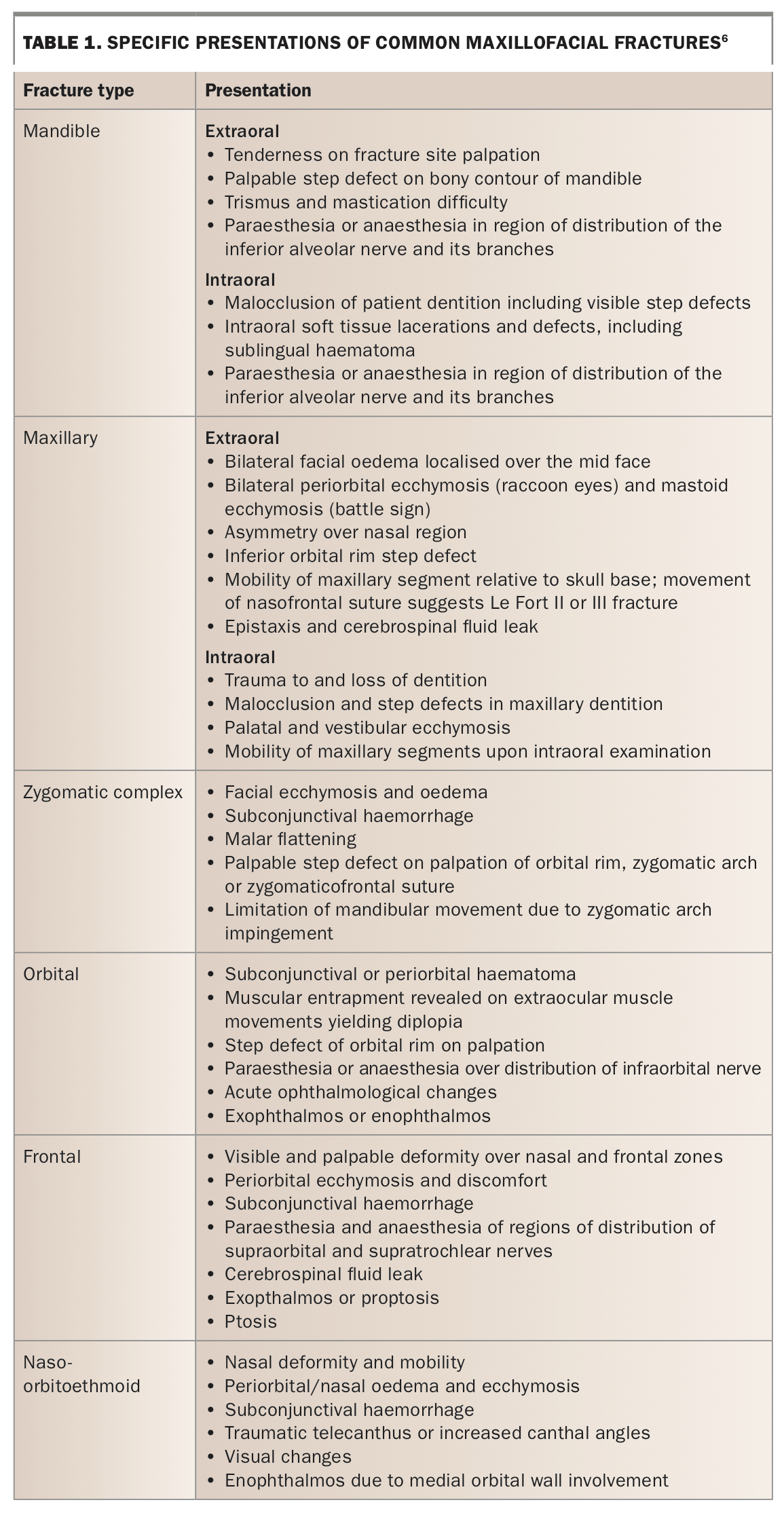
Examination of the head and neck region allows appropriate identification of suspected fracture location within the maxillofacial region, with subsequent classification as lower, mid and upper face fractures. Recognising soft tissue trauma that is commonly associated with facial fractures is an important part of examination. The presence of oedema and haematomas may increase the difficulty in identifying fractures. Common maxillofacial fractures are outlined below and their presenting features summarised in Table 1.
{kind=link}
Mandible fractures
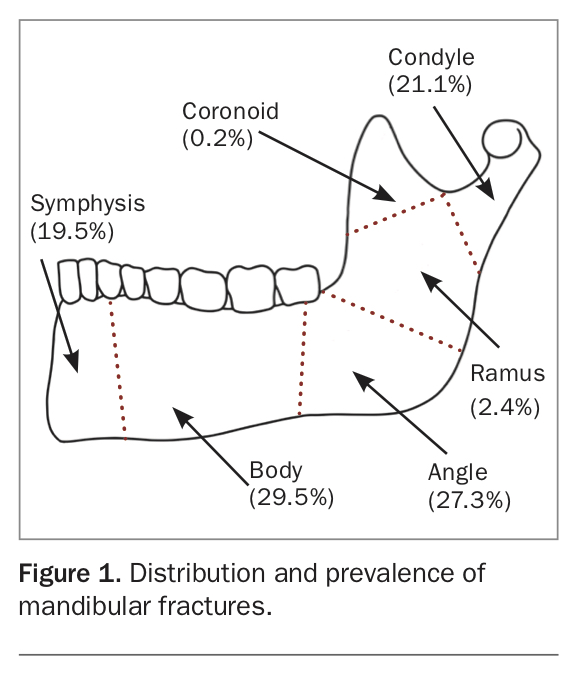
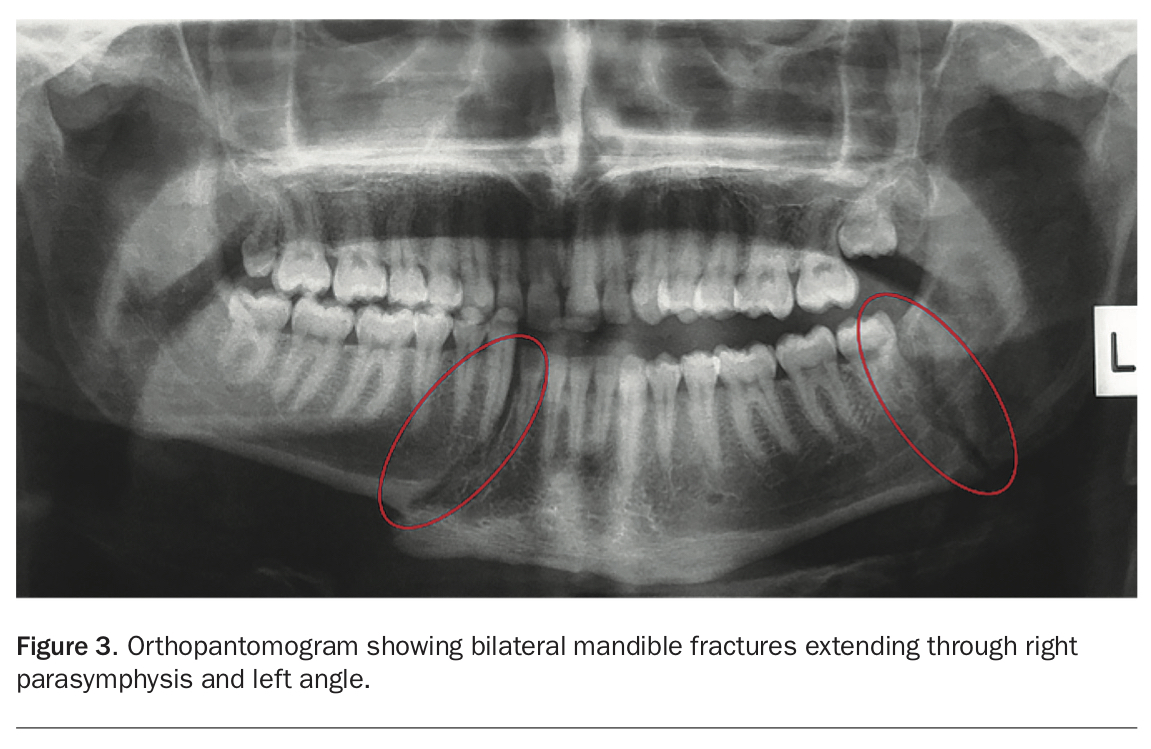
The mandible is a common region of maxillofacial fracture (Figure 1).5 Importantly, multiple sites of fracture within the mandible following trauma are common. Therefore, when a single site of fracture is identified, additional investigation should be undertaken to rule out a concurrent fracture on the contralateral aspect of the mandible.1
{kind=link}
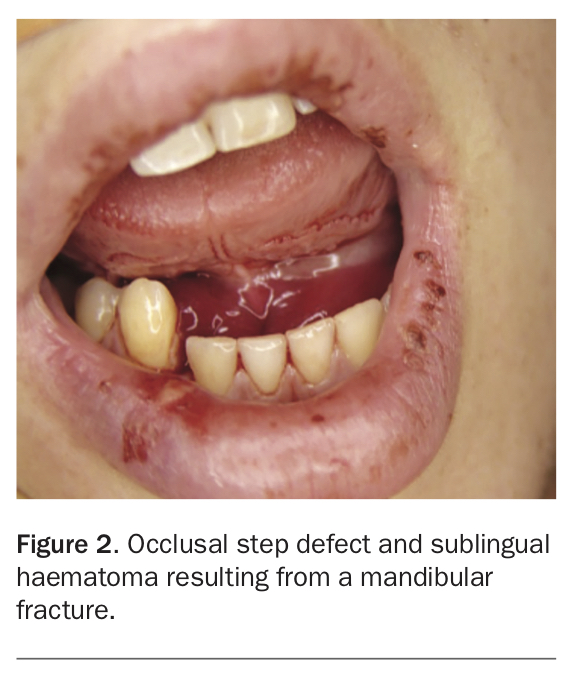
Of relevance to GPs are condylar fractures, which may present after low-impact trauma with limited symptoms, such as altered mouth opening or pain on jaw movement. Condylar fractures are routinely conservatively managed and thus identification and subsequent review after referral is typically carried out by GPs. Examples of common mandibular fractures seen in general practice are shown in Figure 2 and Figure 3.
{kind=link}
{kind=link}
Maxillary fractures
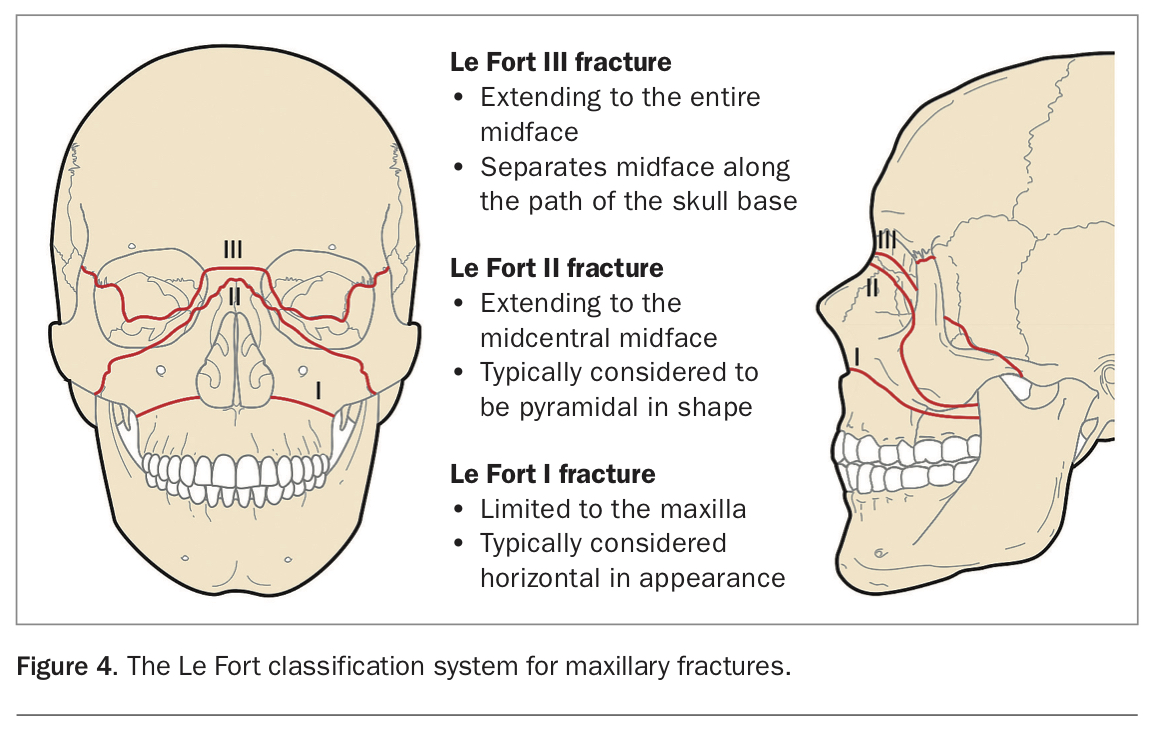
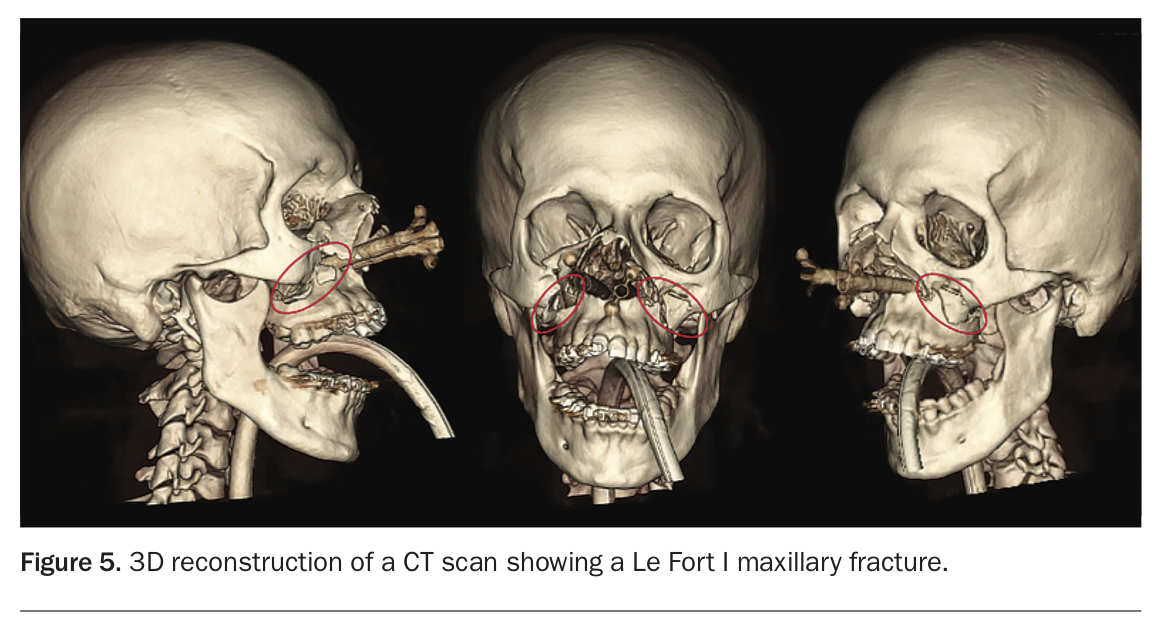
Multiple maxillary fractures often occur concurrently, resulting in significant morbidity. These fractures are broadly classified using the Le Fort classification system, which aims to distinguish maxillary fractures according to the plane of injury, as shown in Figure 4 and Figure 5.6
{kind=link}
{kind=link}
Zygomatic complex fractures
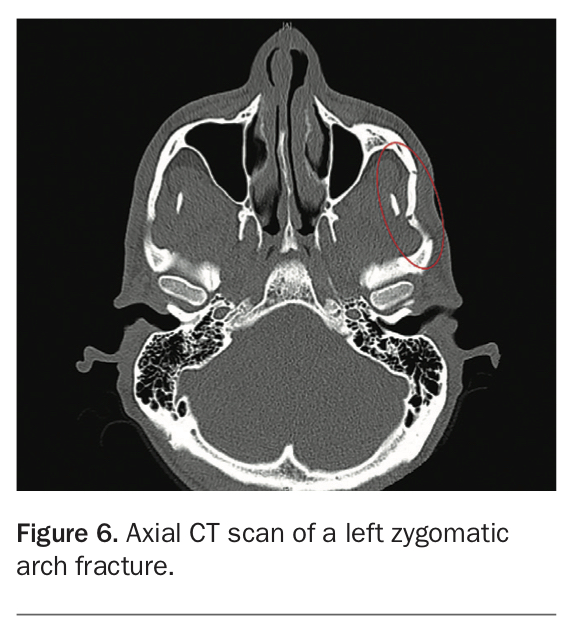
The zygomatic bone articulates with multiple bones in the midface. Of importance, it forms part of the orbital cavity and acts as a shock absorber or crumple zone for injuries to the midface and protects the orbital contents from damage. Its structural role and positioning within the face places it at increased risk of traumatic injury.7 Knowledge of the articulations of the zygomatic arch to the infraorbital rim and frontal, temporal and maxillary bones allows for understanding of the sites of possible fracture.
Because of the proximity of the zygomatic complex to the orbit, any patient with a zygomatic complex fracture (Figure 6) must receive an appropriate ophthalmological examination, including assessment of visual acuity, pupil reaction and reflexes, movement of the globe in all directions and evidence of diplopia, if suspicion of orbital fracture or injury exists.
{kind=link}
If any abnormal signs are present, an ophthalmological review should be sought. Intraocular injury should be excluded, particularly if surgical repair is planned.
Orbital fractures
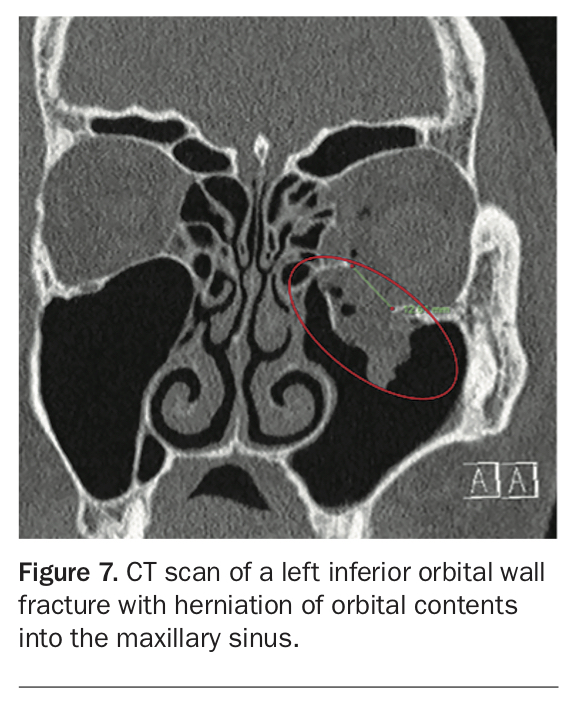
The thinness of the bones in the inferior and medial walls of the orbit compared with the lateral and superior walls explains the proportion of orbital fractures presenting at these surfaces. Additionally, orbital fractures are routinely associated with zygomatic, frontal, naso-orbitoethmoid (NOE) and maxillary fractures (Figure 7) but may occur in isolation after direct trauma. Identifying orbital fractures is important owing to the anatomical complexity within this region, and the potential for orbital contents to herniate through sites of fracture.
{kind=link}
Frontal and naso-orbitoethmoid fractures
Because of their close proximity to important anatomical structures, frontal bone and NOE fractures have the potential to cause significant functional and aesthetic morbidity.6 Determining the extent of a frontal bone fracture routinely requires CT imaging (Figure 8); however, clinical parameters such as cerebrospinal fluid leak can provide insight into posterior table involvement. As discussed above, NOE fractures involving the orbit require appropriate ophthalmological work up due to the propensity for significant morbidity.
{kind=link}
Emergency presentations
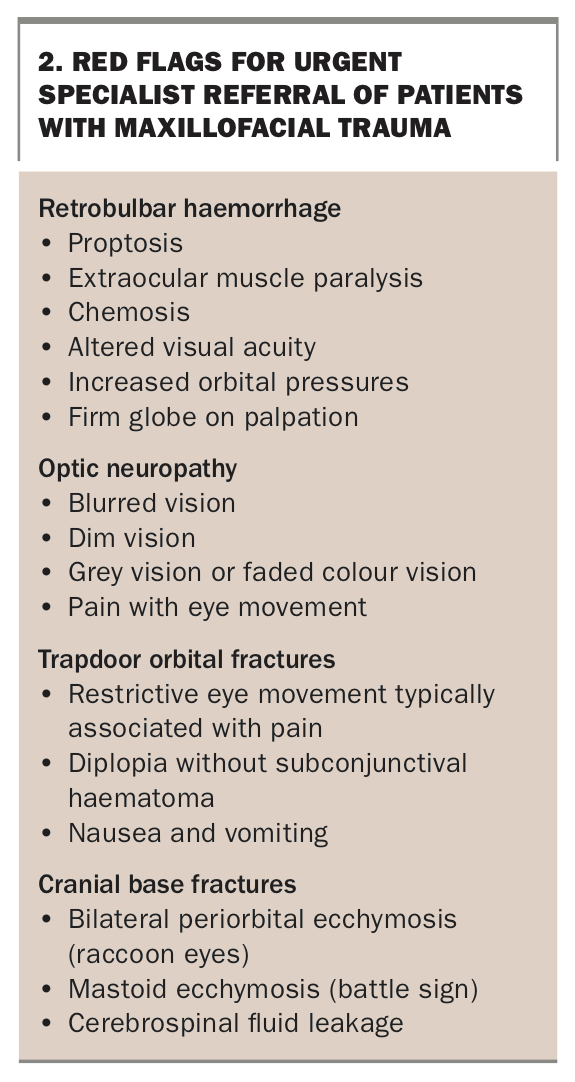
Maxillofacial trauma can result in significant morbidity; however, a few presentations require urgent intervention. These presentations are important to recognise and appropriately manage (Box 2).
{kind=link}
Retrobulbar haemorrhage
Orbital trauma may result in haemorrhage and development of a compartment syndrome within the orbit. As a result, the patient may present with proptosis, extraocular muscle paralysis, chemosis and altered visual acuity, in addition to increased orbital pressures and a firm globe on palpation. Such a presentation typically requires referral to an emergency department for decompression via lateral canthotomy by an oral and maxillofacial surgeon or ophthalmologist.
Trapdoor orbital (white eye blow out) fractures
These fractures present predominantly within the paediatric population due to bony elasticity of the orbital wall, resulting in trapping of orbital contents, including musculature, and can cause significant morbidity when not acutely managed. Features of trapdoor orbital fractures include restrictive eye movement typically associated with pain, diplopia with the absence of subconjunctival haematoma, nausea and vomiting. Management in under 48 hours is required for preservation of ocular movement.
Cranial base fracture
Features suggestive of a cranial base fracture include bilateral periorbital ecchymosis (raccoon eyes), mastoid ecchymosis (battle sign) and cerebrospinal fluid leakage. Referral to a tertiary healthcare centre is needed for the management of cranial base fractures.
Investigations
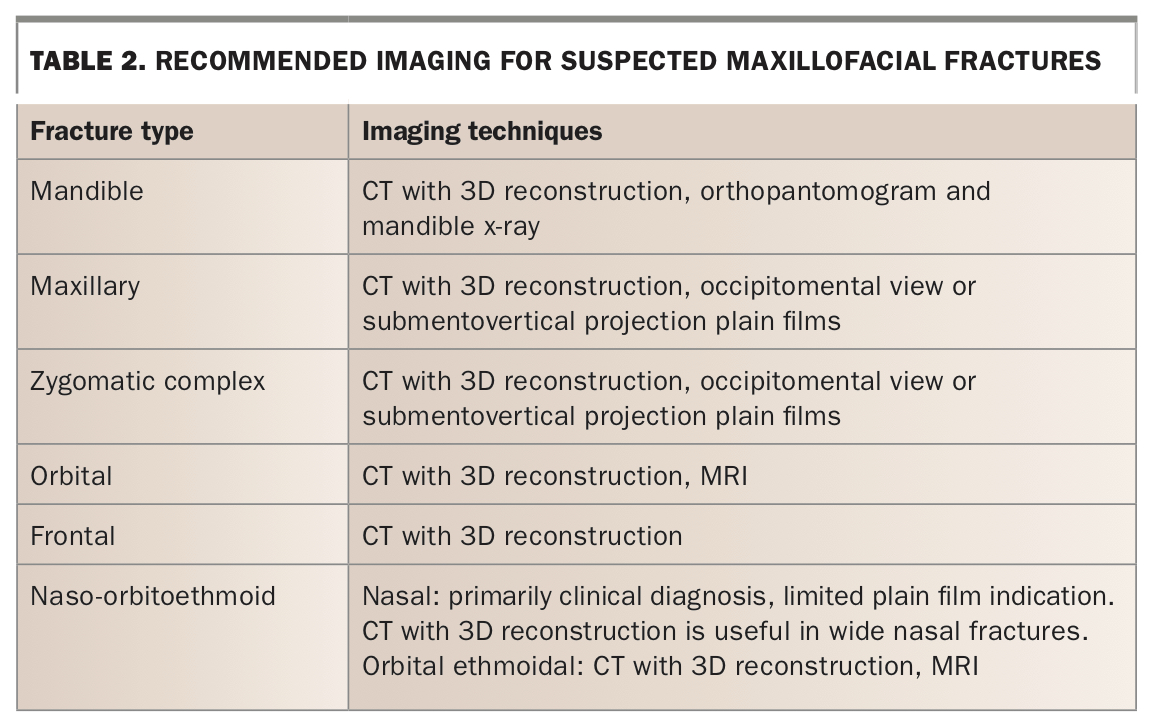
Radiographic imaging forms the mainstay of diagnostic investigations for maxillofacial trauma. In tertiary care, CT is the gold standard for diagnosis and surgical planning; however, the use of plain films and MRI are still of merit (Table 2).3 In the setting of associated dentoalveolar trauma, additional radiographic imaging is likely to be completed on assessment by a dental practitioner.8
{kind=link}
GP management
Presentation to a GP for assessment and management, particularly after low-impact maxillofacial trauma, is not uncommon. Hence GPs form a crucial component of the identification and management of maxillofacial fractures. The key role of GPs in acute maxillofacial trauma includes:
- triage of low-impact maxillofacial trauma in patients not immediately transferred to emergency department
- management of minor soft tissue trauma in the absence of maxillofacial fractures
- early radiographic investigation of facial fractures in unclear presentations
- identification of red flag conditions such as retrobulbar haemorrhage, optic neuropathy and trapdoor orbital fractures that require urgent referral (Box 2)3,9
- appropriate referral to a surgical unit for management of facial fractures and ophthalmological complications, or a dental practitioner for the management of concurrent dentoalveolar trauma
- provision of antibiotic therapy such as amoxicillin or clindamycin for mandibular and maxillary fractures that have delayed surgical management because of oral seeding of infection.10
The timeline for referral depends on the extent of suspected facial injury and patient symptoms. Urgent specialist referral is needed if red flag conditions are identified (Box 2), with painful and symptomatic mandibular and maxillary fractures often requiring referral within less than 24 hours. All other fractures not at risk of compromising patient vision or stability should be referred within seven days.3
In addition to managing acute presentations, GPs have a role in postoperative review after surgical intervention, including reviewing extended paraesthesia and anaesthesia and identifying late surgical complications such as infected hardware and altered growth.
Management in a maxillofacial surgical unit
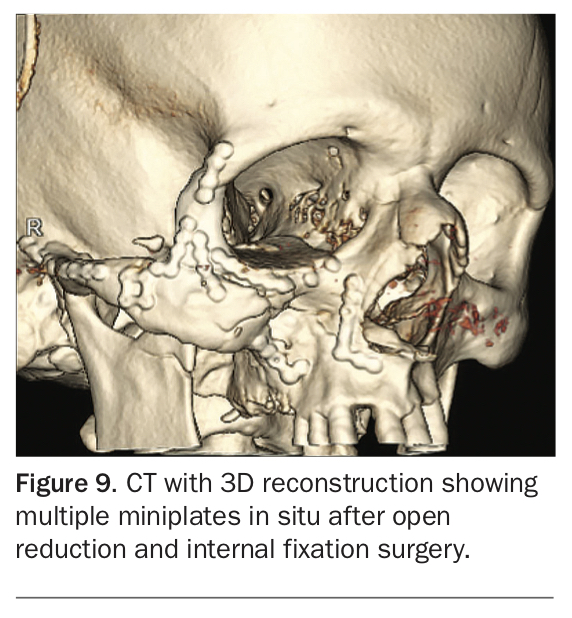
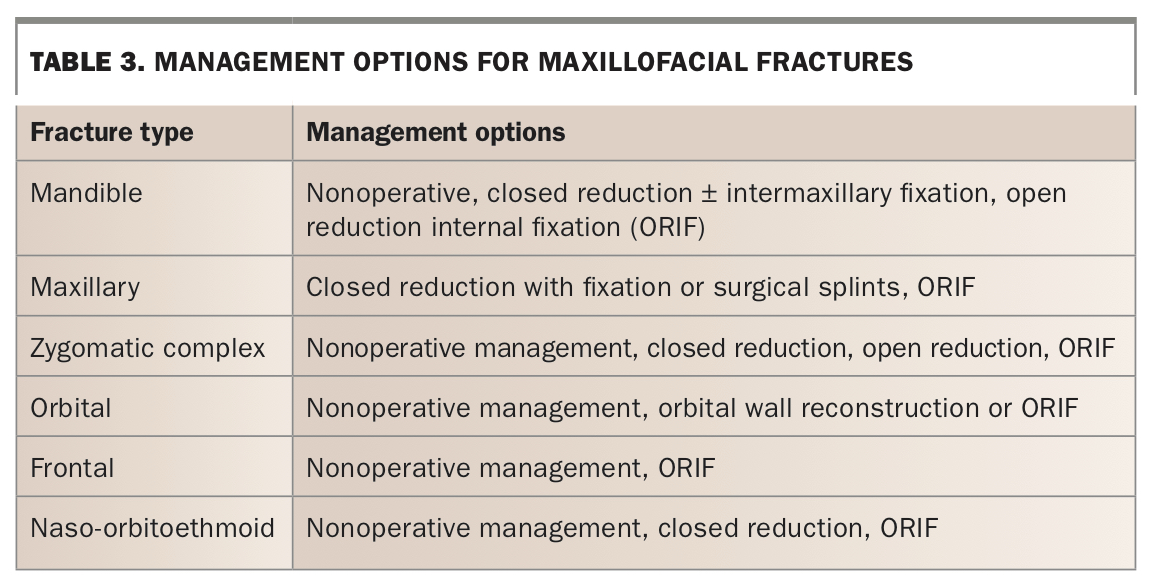
After presentation to a maxillofacial surgical unit, the outcome of assessment of facial fracture will determine appropriate management, including surgery or other treatment (Figure 9). Table 3 summarises the management options for the facial fractures discussed above.6,11
{kind=link}
{kind=link}
Conclusion
Early identification and management of maxillofacial fractures is crucial to reducing morbidity associated with delayed management. The ABCDE framework and an information gathering tool such as the SAMPLE method can help GPs assess suspected maxillofacial fractures and identify patients who need immediate hospital management and those who require appropriate referral to a surgical unit for timely management. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.