Treating mild COVID-19 – what therapeutic options are available?

Associate Professor Barber is an Infectious Diseases Physician at Royal Brisbane and Women’s Hospital, Brisbane; Team Head of the Clinical Malaria Group at QIMR Berghofer Medical Research Institute, Birsbane, Qld; and Co-chair of the Drug Treatment and Chemoprophylaxis Panel of the National COVID-19 Clinical Evidence Taskforce (NC19CET).
Associate Professor Tari Turner is an Associate Professor (Research) in the School of Public Health and Preventive Medicine, Monash University, Melbourne; and Director of the NC19CET.
Mr White is the Deputy Director of Evidence and Methods at the NC19CET; and Evidence Lead for the Living Evidence for Diabetes Program, School of Public Health and Preventive Medicine, Monash University, Melbourne.
Professor Cheng is Professor of Infectious Diseases Epidemiology in the School of Public Health and Preventive Medicine, Monash University; and Director of the Infection Prevention and Healthcare Epidemiology Unit, Alfred Health, Melbourne.
Associate Professor McGloughlin is an Intensive Care Physician and Infectious Diseases Physician at the Alfred Hospital, Melbourne; Adjunct Clinical Associate Professor in the School of Public Health and Preventive Medicine, Monash University, Melbourne, Vic; and Executive Director of the NC19CET.
Infectious diseases
With the rapid introduction of new treatments for mild COVID-19, GPs need to be aware of the latest information to help them recognise which patients are candidates for available therapies. Treatment options for suitable patients with mild COVID-19 include antivirals and monoclonal antibodies, with the oral antivirals being most relevant for GPs. GPs should always refer to COVID-19 living guidelines to ensure they provide accurate advice to their patients.
The COVID-19 pandemic has stimulated an unprecedented number of clinical trials evaluating new therapeutics for COVID-19. Keeping abreast of the evidence relating to these new therapeutics has presented a major challenge for GPs. This has been compounded by the emergence of new variants, which has reduced the effectiveness of some treatments.
A number of therapeutic agents are now approved by the Therapeutic Goods Administration (TGA) to treat COVID-19, some of which are available on the PBS for specific patient groups. Of most relevance to GPs are the oral antivirals nirmatrelvir-ritonavir and molnupiravir. However, GPs should also be familiar with the intravenous antiviral remdesivir, so that they are able to refer patients if oral antivirals are not appropriate. Monoclonal antibodies are also available, and although some (e.g. sotrovimab and casirivimab-imdevimab) are no longer recommended because of reduced activity against the current SAR-CoV-2 Omicron variants, tixagevimab-cilgavimab is predicted to retain efficacy.1-3 Tixagevimab-cilgavimab is currently only approved by the TGA for pre-exposure prophylaxis; however, it is recommended by the National COVID-19 Clinical Evidence Taskforce (NC19CET) as one of the treatment options for patients with mild COVID-19.
Recommendations for the use of COVID-19 therapeutic agents are changing rapidly with the emergence of new data, and GPs are advised to refer to the NC19CET’s living guidelines for the most up-to-date information.4 This article reviews the current recommended treatments for mild to moderate COVID-19, and provides guidance on which patients should be offered these treatments.
Who should be offered a therapeutic agent for COVID-19?
The SARS-CoV-2 Omicron variants are associated with significantly lower severity of disease compared with the previously dominant Delta variant, and most patients with COVID-19 now develop only mild disease.5,6 Although vaccine efficacy against symptomatic infection is lower for Omicron compared with Delta variants, effectiveness remains high against hospitalisation and death.5,7 At the time of writing, in Australia, about 1.4% of patients with COVID-19 are hospitalised, and the overall fatality rate for notified COVID-19 cases has remained at below 0.1% since the onset of the Omicron wave in December 2021.8,9
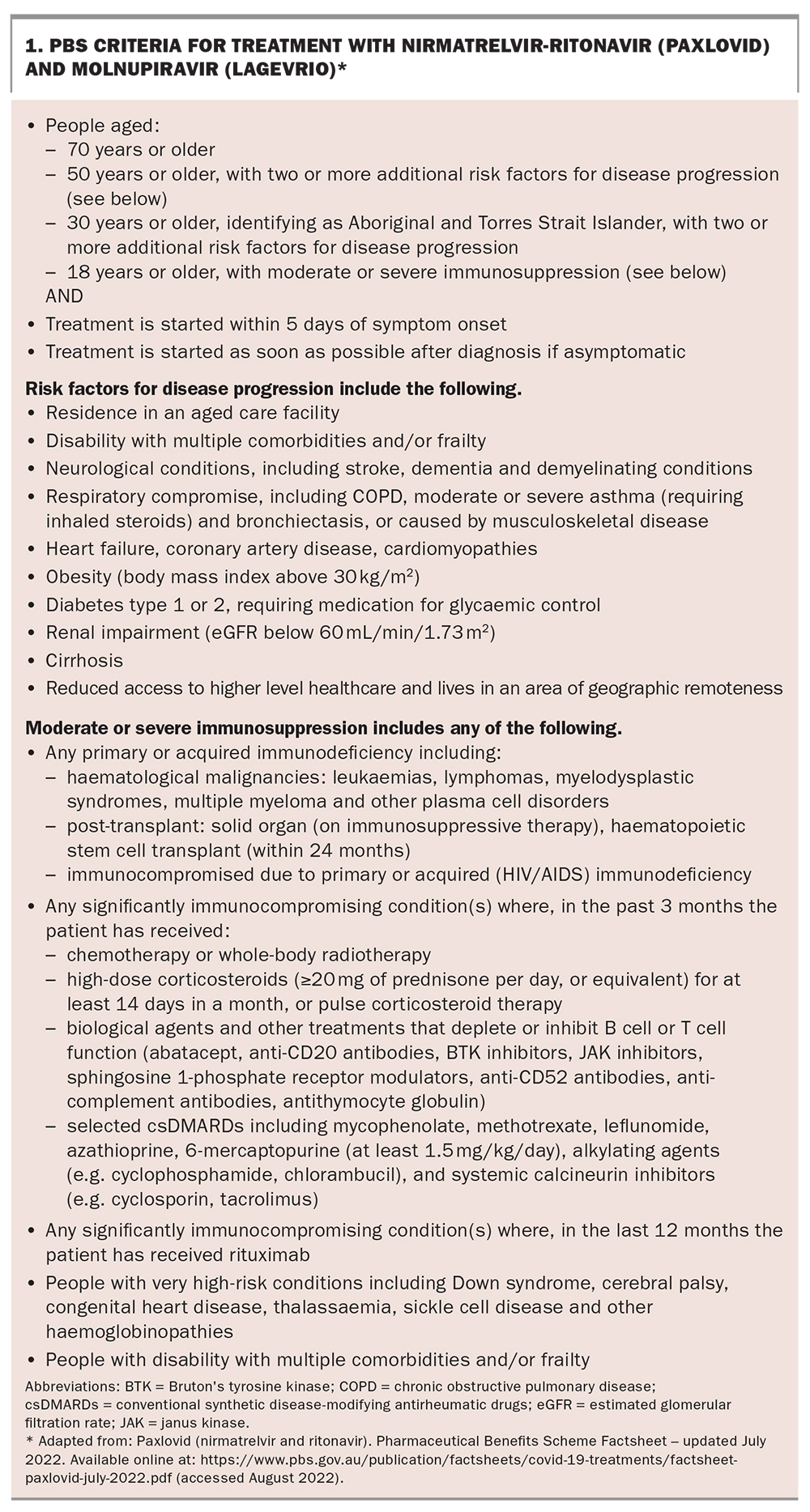
Given this low severity of disease, most patients with mild COVID-19 do not need a specific therapeutic agent. However, it is important for GPs to be aware of the factors that may increase an individual’s risk of progressing to more severe disease, such as age, comorbidities, Aboriginal and Torres Strait Islander status and whether a patient is immunosuppressed. Based on these factors, the Pharmaceutical Benefits Advisory Committee has provided eligibility criteria for PBS access to oral antivirals (Box 1). Patients who are under 50 years of age (or under 30 years for Aboriginal and Torres Strait Islander people) with no risk factors for disease progression do not meet PBS eligibility criteria and do not need antiviral treatment. Patients meet PBS eligibility criteria if they are:
{kind=link}
- over 70 years old
- over 50 years old with two or more additional risk factors for progression
- over 30 years, of Aboriginal and Torres Strait Islander descent and with two or more comorbidities
- over 18 years old with moderate or severe immunosuppression.
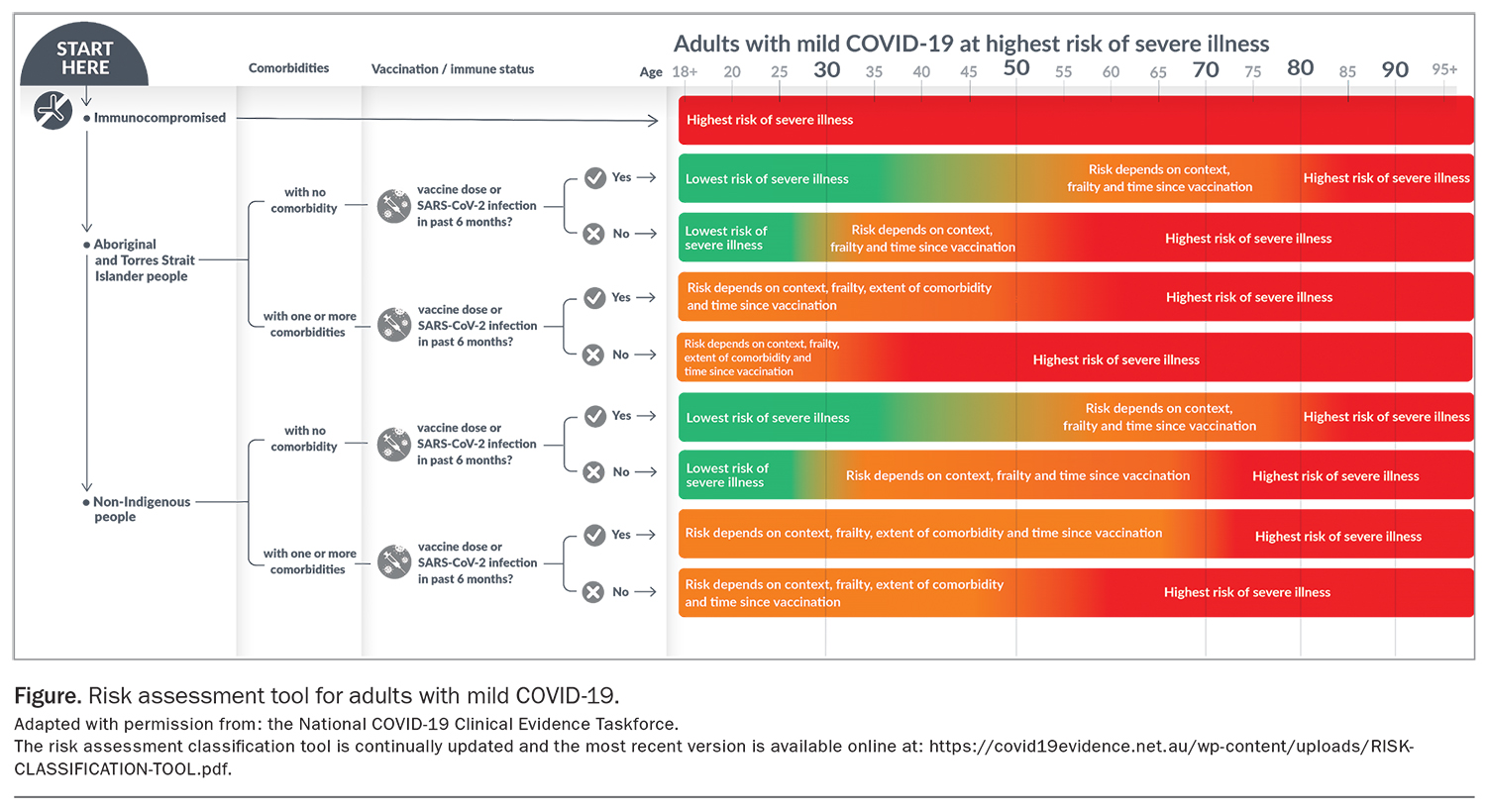
For patients who meet these PBS eligibility criteria, GPs are still advised to consider vaccination status and to conduct an individual risk assessment to determine which patients will benefit most from treatment. A risk assessment tool has been has been developed by the NC19CET to assist GPs with this assessment (Figure), and may be used in conjunction with the NC19CET Clinical Flowchart for drug treatments for at risk adults with COVID-19 who do not require oxygen (https://covid19evidence.net.au/wp-content/uploads/DECISION-TOOL-DT-FOR-ADULTS.pdf?=220721-51024). It is important to note that this risk assessment tool is continually updated and GPs should check for the most recent version online (https://covid19evidence.net.au/wp-content/uploads/RISK-CLASSIFICATION-TOOL.pdf).
{kind=link}
Although PBS criteria do not take into account vaccination status, individuals who have recently received a fourth dose of a COVID-19 vaccine are at significantly lower risk of progression to severe disease than unvaccinated individuals. Therefore, for fully (and recently) vaccinated patients who meet PBS eligibility criteria but are at lower risk of disease progression (for example, a 70-year-old with no other risk factors, or a 50-year-old with a body mass index of 32 kg/m2 and well-controlled type 2 diabetes mellitus), the potential benefits and harms of treatment should be discussed, and a shared decision made with the patient.
GPs should also ask patients about the duration of their symptoms. COVID-19 therapeutics are most effective if given early in the course of disease, and GPs should ensure that their patients know to contact them as soon as possible if they test positive for SARS-CoV-2. The time-frame (from symptom onset) within which therapeutics may be administered varies slightly based on the inclusion criteria of the relevant clinical trials, being five days for nirmatrelvir-ritonavir, molnupiravir and tixagevimab-cilgavimab; and seven days for remdesivir.10-13
Patients who do not need specific therapy for COVID-19 can be reassured that, because of their age, vaccination status or lack of comorbidities, they are at low risk of severe disease, and can be managed with simple symptomatic treatments such as paracetamol and anti-inflammatories.
Which agent should be offered to patients who meet the treatment criteria?
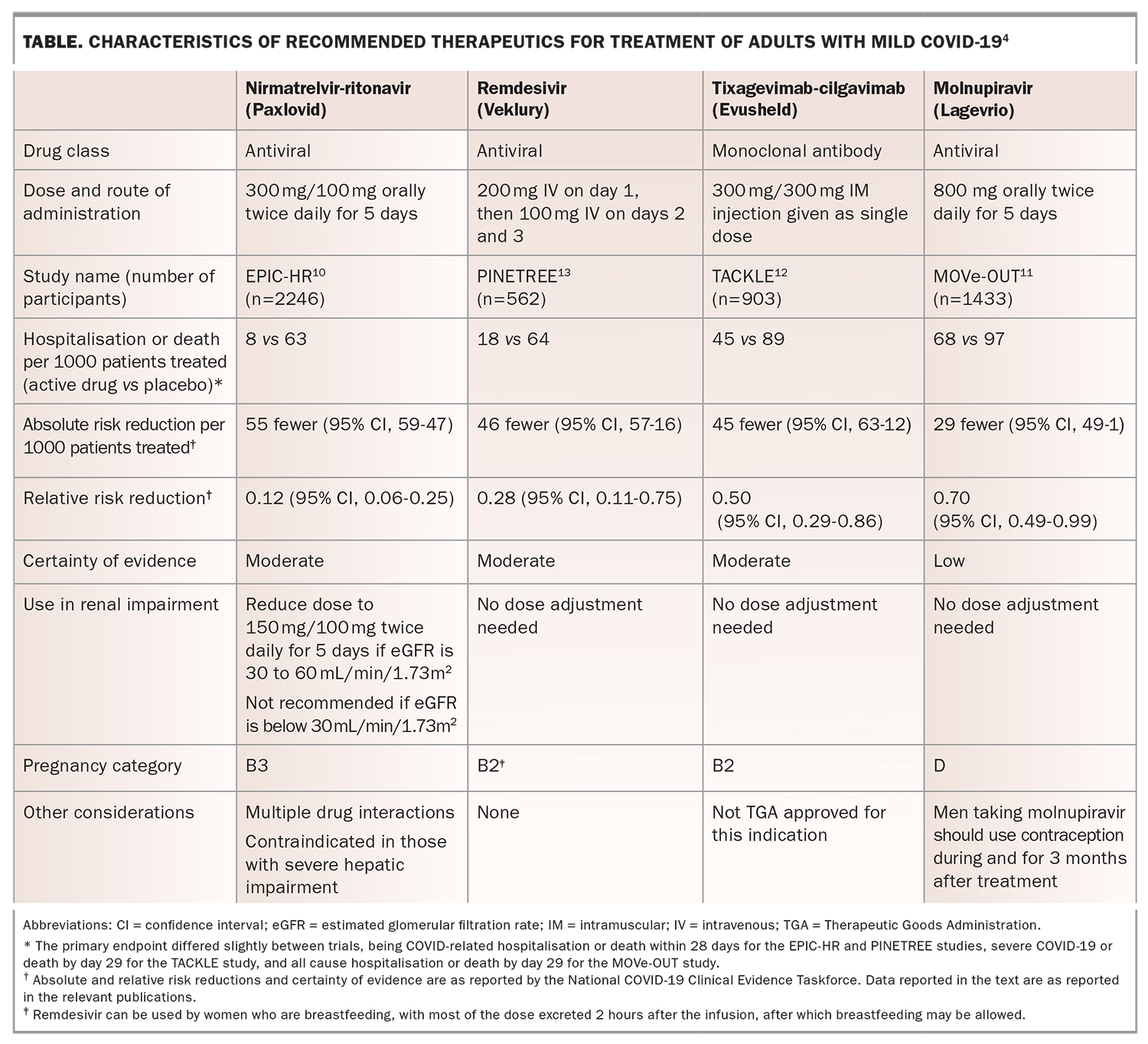
If a decision is made to offer a specific therapeutic for treatment for mild COVID-19, the choice of which agent to offer depends on a number of factors, including availability, drug interactions and other contraindications such as pregnancy. The key characteristics of the currently recommended agents, as reported by the NC19CET, are summarised in the Table. However, with the rapid emergence of new data, and the likelihood of changing variants, GPs are advised to refer to the NC19CET guidelines for the most up-to-date recommendations. As with all medications, patients prescribed oral medications for COVID-19 should be reminded of the importance of using these medications solely for their own use.
{kind=link}
Nirmatrelvir-ritonavir
Nirmatrelvir-ritonavir (Paxlovid) is a combination of two protease inhibitors (with ritonavir used as a ‘pharmacokinetic enhancer’), administered orally twice daily for five days. Evidence for its use comes from the EPIC-HR trial, which enrolled nonhospitalised adults aged 18 years and above, with confirmed SARS-COV-2 infection, who were within five days of symptom onset and had at least one risk factor for developing severe disease (with age 60 years and greater included as a risk factor).10 Nearly all (98%) patients were infected with the Delta variant and, as with most COVID-19 clinical trials, vaccinated patients were excluded from enrolment. The primary endpoint of COVID-related hospitalisation or death within 28 days occurred in 0.72% (5/697) of patients in the nirmatrelvir-ritonavir arm compared with 6.54% (44/682) in the placebo group, amounting to a 5.8% absolute reduction (95% confidence interval [CI], 3.8-7.8%) and an 88.9% relative reduction. No deaths occurred in the nirmatrelvir-ritonavir arm, compared with nine in the placebo arm. Based on these data (graded by the NC19CET as of moderate certainty), nirmatrelvir-ritonavir is the preferred oral antiviral to offer to at-risk patients with mild COVID-19 who are within five days of symptom onset.
Nirmatrelvir-ritonavir is available on the PBS; however, several points need consideration before prescribing it to patients. First, nirmatrelvir-ritonavir is both an inhibitor (primarily because of the activity of ritonavir) and a substrate of the CYP3A enzyme, and may interact with a number of medications. It is therefore essential that GPs review patients’ prescribed and over-the-counter medications (including herbal supplements) and assess for possible drug interactions. GPs should refer to the TGA product information sheet for Paxlovid, and drug interactions should also be checked using an online tool, such as the University of Liverpool’s drug interaction checker (https://covid19-druginteractions.org/checker) or UpToDate’s Lexicomp Drug Interaction tool (www.uptodate.com/drug-interactions; available only to subscribers). Nirmatrelvir-ritonavir should not be used if patients are taking strong CYP3A inducers, even if they are able to withhold taking that medication, as the concentrations of nirmatrelvir will be reduced and the nirmatrelvir-ritonavir may be ineffective. For patients who are taking CYP3A substrates, it may be possible to prescribe nirmatrelvir-ritonavir. Depending on the indication, therapeutic index and half-life of the CYP3A substrate, it may be possible to withhold, dose-reduce or continue it with close monitoring.
Nirmatrelvir-ritonavir requires dose reduction if used for patients with an estimated glomerular filtration rate (eGFR) of 30 to 60 mL/min/1.73 m2, and is not recommended for those with an eGFR below 30 mL/min/1.73 m2 or those with severe hepatic impairment (Child-Pugh score class C). Nirmatrelvir-ritonavir is not recommended in pregnancy, and patients should be advised to avoid breastfeeding during, and for seven days after, treatment. Nirmatrelvir-ritonavir should also be avoided in patients with uncontrolled HIV infection, because of the risk of developing protease inhibitor resistance. Nirmatrelvir- ritonavir tablets can be taken without or without food; they must be swallowed whole and not crushed.
Molnupiravir
Molnupiravir (Lagevrio), a nucleoside prodrug of N-hydroxycitidine, is, at the time of writing, the only other oral antiviral that may be considered for the treatment of mild COVID-19. It is available on the PBS for patients who meet eligibility criteria and, like nirmatrelvir-ritonavir, is administered twice daily for five days.
Evidence for the use of molnupiravir comes from the MOVe-OUT study.11 Inclusion criteria were similar to the nirmatrelvir-ritonavir EPIC-HR trial, with patients enrolled if they were unvaccinated, within five days of symptom onset and if they had one or more risk factors for severe COVID-19 or were aged 60 years or older regardless of risk factors. The benefit of molnupiravir was more modest than for nirmatrelvir-ritonavir, with the primary endpoint of all-cause hospitalisation or death occurring in 6.8% (48/709) of those in the molnupiravir arm compared with 9.7% (68/699) in the placebo arm, giving a relative risk ratio of 0.70 (95% CI, 0.49-0.99) and an absolute risk reduction of 3.0% (95% CI 0.1-5.9%). Based on these data and substantial variation between results in the first and second halves of the trial, the NC19CET have graded the certainty of evidence for a benefit of molnupiravir as low, and have provided a consensus recommendation (a recommendation made in the absence of strong evidence) that molnupiravir be considered for treatment of COVID-19 only where other treatments are not suitable or available.
Molnupiravir must not be used in pregnancy, as fetal toxicity has been reported in animal studies.14 Men should also be advised to use adequate contraception during, and for three months after, treatment. Breastfeeding is not recommended during, and for four days after, treatment. Unlike nirmatrelvir-ritonavir, molnupiravir can be crushed, or capsules opened and sprinkled into food or suspension made in water, which may be useful for administration in residential aged care facilities or for people with a disability who have issues with swallowing. Dose adjustment of molnupiravir is not required for patients with renal impairment.
There are no randomised controlled trials comparing nirmatrelvir-ritonavir and molnupiravir, or any other treatments for mild COVID-19. However, recent real-world observational studies suggest that the protective effects of nirmatrelvir- ritonavir in nonhospitalised adults are greater than those of molnupiravir, supporting the recommendations of the NC19CET.15,16
Remdesivir
Remdesivir (Veklury) is an intravenously administered antiviral that was first recommended for treating hospitalised patients with COVID-19 who required supplemental oxygen but were not mechanically ventilated, based on data from six randomised controlled trials, the largest of which was the WHO’s Solidarity Trial.17-22 For this patient group, remdesivir is administered as a once daily intravenous infusion for five days, with a 200 mg loading dose on the first day followed by 100 mg daily.
More recently, data from the PINE-TREE study showed that remdesivir is also beneficial for patients with COVID-19 who do not require supplemental oxygen.13 The study enrolled nonhospitalised patients who were 12 years and older with one or more risk factors for severe disease or were 60 years and older regardless of risk factors. In contrast to the EPIC-HR and the MOVe-OUT studies, patients could be within seven, rather than five, days of symptom onset. Remdesivir was administered for three days at 200 mg on the first day followed by 100 mg on days 2 and 3. The primary endpoint of hospitalisation or death occurred in 0.7% (2/279) of patients in the remdesivir arm compared with 5.3% (15/283) in the placebo arm, resulting in a hazard ratio of 0.13 (95% CI, 0.03-0.59) and an absolute risk reduction of 4.6% (95% CI, 1.6-5.7%), an effect size and certainty of evidence similar to those seen with nirmatrelvir-ritonavir in the EPIC-HR study.
Although the administration of remdesivir requires GPs to refer patients to a health facility that can administer the intravenous infusions, this option may be considered for particularly high-risk patients who are not able to receive nirmatrelvir-ritonavir because of drug interactions, pregnancy or severe renal impairment.
Tixagevimab-cilgavimab
Tixagevimab-cilgavimab (Evusheld) is a combination of two monoclonal antibodies administered as a single 600 mg dose in two 300 mg intramuscular injections. Tixagevimab-cilgavimab has been provisionally approved by the TGA for pre-exposure prophylaxis for immunosuppressed patients, based on data from the PROVENT study, and may be considered for use in these patients.23 In addition, the NC19CET has recommend that it be considered an option for the treatment of mild COVID-19, although this indication has not yet been approved by the TGA.
Data supporting the use of tixagevimab-cilgavimab for mild COVID-19 comes from the TACKLE trial, which enrolled unvaccinated patients aged 18 years and older, with one or more risk factors for severe disease (including age 65 years or more) and who were within five days of symptom onset.12 The primary endpoint of severe COVID-19 or death occurred in 4% (18/407) of patients randomised to tixagevimab-cilgavimab, compared with 9% (37/415) of those randomised to placebo, giving a relative risk reduction of 50.5% (95% CI, 14.6-71.3) and an absolute risk reduction of 4.5% (95% CI, 1.1-8.0). Based on these data, the NC19CET recommends that tixagevimab-cilgavimab may be considered for treatment of immunosuppressed or unvaccinated at-risk adults with mild COVID-19. Although some in vitro studies suggest tixagevimab-cilgavimab has reduced neutralising activity against the BA.4 and BA.5 Omicron variants, recent modelling suggests that this antibody combination is likely to remain clinically efficacious.3,24
Other monoclonal antibodies: sotrovimab and casirivimab-imdevimab
The monoclonal antibodies sotrovimab and casirivimab-imdevimab (Ronapreve), both administered as single intravenous infusions, were previously recommended for the treatment of at-risk adults with mild COVID-19. Data for sotrovimab came from the COMET-ICE trial, while data for casirivimab-imdevimab came from the RECOVERY trial and one other randomised trial.25-27 However, these trials were conducted before the emergence of the Omicron variant, and both sotrovimab and casirivimab-imdevimab have been shown in vitro to be less effective against neutralising the Omicron BA.2 variant.28 More recent data also suggest reduced neutralisation activity of these antibodies against the newer variants BA.4/BA.5, thus their role for current treatment of COVID-19 remains limited.1,2
What about inhaled corticosteroids?
Inhaled corticosteroids, particularly budesonide, have been widely used for treating mild COVID-19, due, in part, to their low cost, ease of administration and good safety profile. However, data supporting their use are limited, primarily because of the lack of any placebo-controlled trial. A meta-analysis performed by the NC19CET found that inhaled corticosteroids may slightly decrease the need for supplemental oxygen, but have little impact on the rate of hospitalisation, compared with standard care. As such, inhaled corticosteroids should not be considered an alternative to preferred agents such as nirmatrelvir-ritonavir or remdesivir. However, given that some benefit of budesonide was noted in the PRINCIPLE trial when was used within 14 days of symptom onset, budesonide may be considered for at-risk patients who present with mild COVID-19 but have had symptoms for seven to 14 days, and are thus are not eligible for other agents.29 Patients with asthma should follow their personal asthma management plan for viral exacerbations.
Conclusion
Optimal management of mild COVID-19 requires GPs to be aware of which patients are at highest risk of severe disease and therefore should be offered a specific therapeutic, and which of the available therapeutics should be given. GPs may consider planning ahead for how to manage their patients if they develop mild COVID. Reference to living guidelines is advised, particularly given the emergence of new COVID-19 variants, which may necessitate rapid changes to guidelines. Practice points for managing patients with mild COVID-19 are summarised in Box 2. MT
{kind=link}