Aspirin therapy in diabetes: evidence and current recommendations

Diabetes type 2
Heart diseases--prevention
Although aspirin use has become an established therapy for the secondary prevention of cardiovascular disease, newer evidence has influenced recommendations regarding the use of aspirin for primary prevention of cardiovascular disease in high-risk patients.
Diabetes remains an ever-increasing global epidemic with over 422 million people affected worldwide and requiring over $827 billion of global health expenditure annually.1 In Australia, over 1.7 million people are living with diabetes, including an estimated 500,000 people who are currently undiagnosed.2,3 Diabetes is associated with a range of acute and chronic complications that contribute to increased morbidity and mortality.1
Aspirin has long been recommended for the primary and secondary prevention of ischaemic heart disease, stroke and peripheral vascular disease, the risks of which are increased in patients with diabetes. However, its efficacy and safety for primary prevention of cardiovascular disease (CVD) have been debated over the past decade. In this review, in light of several recently completed large-scale randomised controlled trials, we examine whether aspirin should still be recommended as a regular therapy for patients with diabetes.
Aspirin: a brief history
Aspirin derivatives, originally extracted from willow bark, have been used for over 3500 years for their analgesic and antipyretic properties. Today’s form of aspirin, acetylsalicylic acid, was first manufactured by German scientists in 1897.4
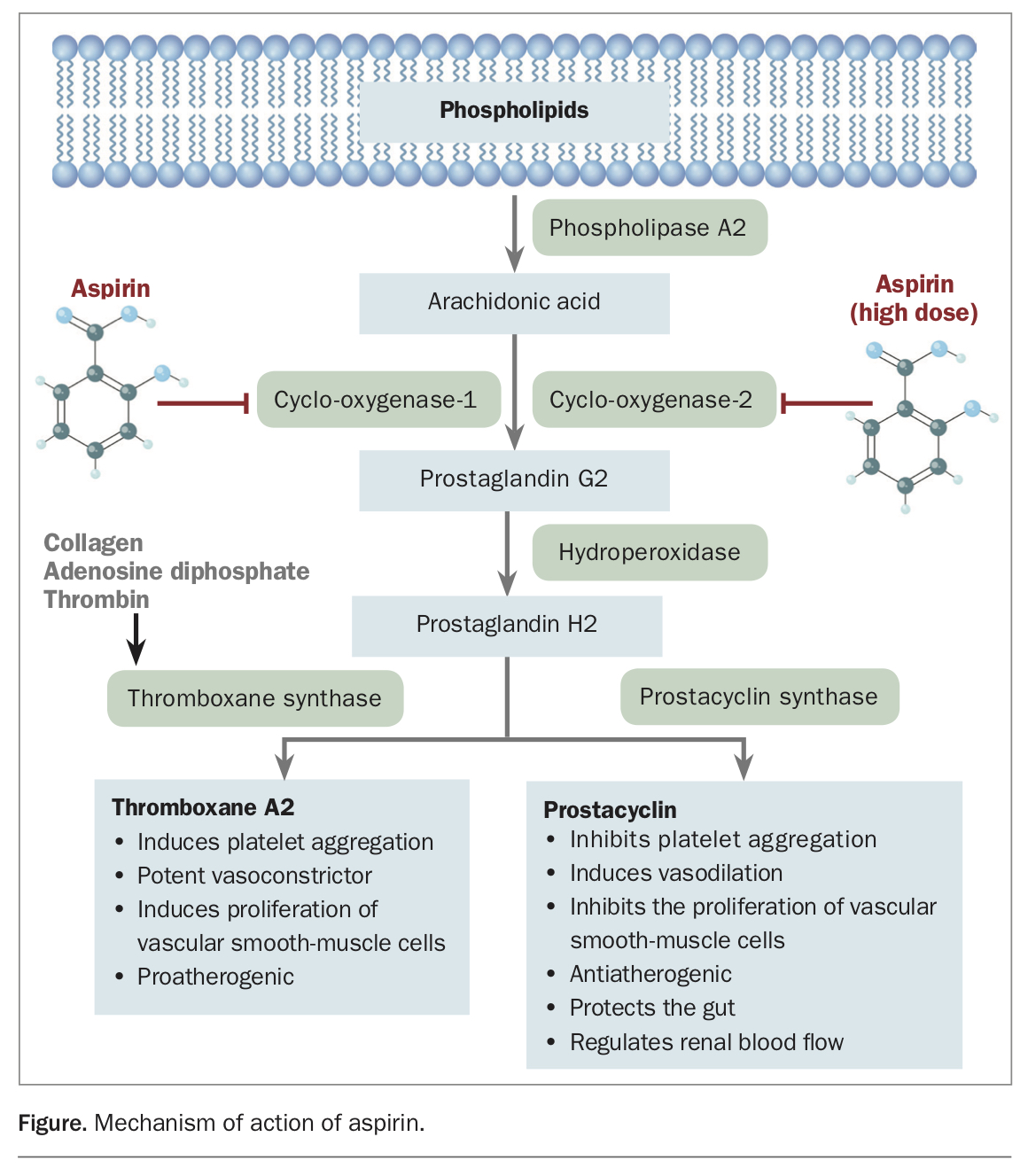
Aspirin works by irreversibly inhibiting activity of prostaglandin G/H synthase, also known as cyclo-oxygenase, the enzyme responsible for the first step in the conversion of arachidonic acid to prostaglandin G2. This results in decreased production of prostaglandin H2 and its downstream molecules prostaglandin GI2 (PGI2 – prostacyclin) and thromboxane A2 (TXA2), among others (Figure). PGI2 and TXA2 stimulate platelet aggregation, and their inhibition results in a significant reduction in the platelet response and a prolongation of bleeding time. This antiplatelet/antithrombotic effect reduces formation of blood clots, which is a seminal event in acute CVD.5
{kind=link}
In 1974 the first randomised controlled clinical trial evaluating aspirin for secondary prevention of CVD reported mortality benefits after myocardial infarction.6 This was followed by several other trials that firmly established the role of aspirin for secondary prevention of CVD, while also highlighting the potential for adverse bleeding events. Below, we list a summary of the key randomised placebo-controlled clinical trials investigating the use of aspirin in primary and secondary prevention of CVD.
What does the evidence say?
Early key aspirin trial outcomes
- Early Treatment Diabetic Retinopathy Study (ETDRS) 1991, 1992. Aspirin use in patients with diabetes did not prevent progression of diabetic retinopathy.7 Aspirin use in patients with diabetes did not reduce all-cause mortality or fatal or nonfatal myocardial infarction. There was also no evidence of significant harm.8
- International Stroke Trial (IST) 1997. Aspirin use in the early stages following an acute ischaemic stroke decreased mortality after adjusting for baseline prognosis and reduced recurrent ischaemic strokes with no increase in haemorrhagic stroke.9
- Chinese Acute Stroke Trial (CAST) 1997. Aspirin use in the early stages following an acute ischaemic stroke reduced mortality and recurrent ischaemic stroke, with a small increase in haemorrhagic stroke.10
- Hypertension Optimal Treatment (HOT) Trial 1998. Aspirin use reduced the composite endpoint of major cardiovascular events and the individual secondary endpoint of myocardial infarction but not stroke. Adversely, nonfatal major bleeds almost doubled, although without an increase in fatal bleeds.11
- Thrombosis Prevention Trial (TPT) 1998. Aspirin use for primary prevention among high-risk men 45 to 69 years of age reduced the composite endpoint of ischaemic heart disease events, mostly due to a reduction in the secondary individual endpoint of nonfatal myocardial infarction.12
- Women’s Health Study (WHS) 2005. Aspirin use for primary prevention among women over 45 years of age did not reduce the composite endpoint of major cardiovascular events. Analysis of secondary individual endpoints showed reduced ischaemic stroke but not myocardial infarction or cardiovascular mortality. Subgroup analysis of those over 65 years of age showed the most consistent benefit with reductions in ischaemic stroke and myocardial infarction but an increase in gastrointestinal bleeding.13
- Prevention of Progression of Arterial Disease and Diabetes (POPADAD) Trial 2008. Aspirin use among high-risk patients with diabetes and asymptomatic peripheral artery disease did not reduce the composite endpoint of fatal myocardial infarction or stroke, nonfatal myocardial infarction or stroke, or above-ankle amputation due to critical limb ischaemia.14
- Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD) 2008. Aspirin use for primary prevention in patients with diabetes did not reduce the composite endpoint of atherosclerotic events. Secondary individual endpoint analysis showed reduced fatal coronary and cerebrovascular events but not all-cause mortality.15
Meta-analyses including the above articles were not conclusive on the effects of aspirin for primary prevention among patients with and without diabetes.16-19 In response, several large-scale clinical trials were designed and completed, as summarised below.
Recent key aspirin trial outcomes
- Japanese Primary Prevention Project (JPPP) 2014. Aspirin use for primary prevention in patients 60 to 85 years of age with multiple atherosclerotic risk factors did not reduce the composite primary outcome of cardiovascular death, nonfatal myocardial infarction and nonfatal stroke. Secondary analysis of individual endpoints demonstrated reduced nonfatal myocardial infarction and transient ischaemic attack, and an increased risk of extracranial haemorrhage.20
- Aspirin to Reduce Risk of Initial Vascular Events (ARRIVE) Trial 2018. Aspirin use for primary prevention in patients with moderate cardiovascular risk (excluding those with diabetes) did not reduce the composite cardiovascular outcome of time to first myocardial infarction, unstable angina, stroke, transient ischaemic attack or cardiovascular death. However, the overall rate of cardiovascular events was lower than expected in the population studied, making the findings difficult to interpret. Aspirin increased gastrointestinal bleeding.21
- Aspirin in Reducing Events in the Elderly (ASPREE) Trial 2018. Aspirin use for primary prevention in patients over 70 years of age (including those with diabetes) did not prolong disability-free survival and unexpectedly increased all-cause mortality, primarily due to cancer-related deaths.22,23 Secondary analysis of cardiovascular endpoints did not demonstrate a reduction in the composite of cardiovascular events, defined as fatal and nonfatal myocardial infarction, fatal and nonfatal stroke or hospitalisation for heart failure. Aspirin increased major haemorrhage, mainly involving upper gastrointestinal and intracranial haemorrhages.24
- A Study of Cardiovascular Events in Diabetes (ASCEND) 2018. Aspirin use for primary prevention in patients with diabetes reduced the composite endpoint of serious vascular events, defined as myocardial infarction, stroke, transient ischaemic attack or death from any vascular cause excluding intracranial haemorrhage. However, the absolute benefit of aspirin use was counterbalanced by the risk of serious bleeding, mostly due to gastrointestinal bleeding and sight-threatening bleeding events in the eye.25
A meta-analysis including pooled data from these recent aspirin trials reported an 11% relative risk reduction and 0.41% absolute risk reduction in composite cardiovascular outcomes in patients without known CVD, without an associated reduction in cardiovascular or all-cause mortality. However, this was accompanied by a 43% relative risk increase and 0.47% absolute risk increase in major bleeding outcomes. This manifested as a number needed to treat of 241, compared with a number needed to harm of 210. Furthermore, a subgroup analysis of patients with diabetes failed to show any significant reduction in cardiovascular events or mortality. This suggests that it would be imperative to consider the potential benefits and risks, in consultation with each individual patient, before the addition of aspirin therapy as primary prevention.26
Current guidelines
In response to the new evidence, cardiovascular management guidelines relating to aspirin have been updated. The following recommendations have been summarised from several leading Australian medical authorities, including the Royal Australian College of General Practitioners and the National Vascular Disease Prevention Alliance.
- All adults with type 2 diabetes and known prior CVD should receive long-term antiplatelet therapy unless there is a clear contraindication.27,28
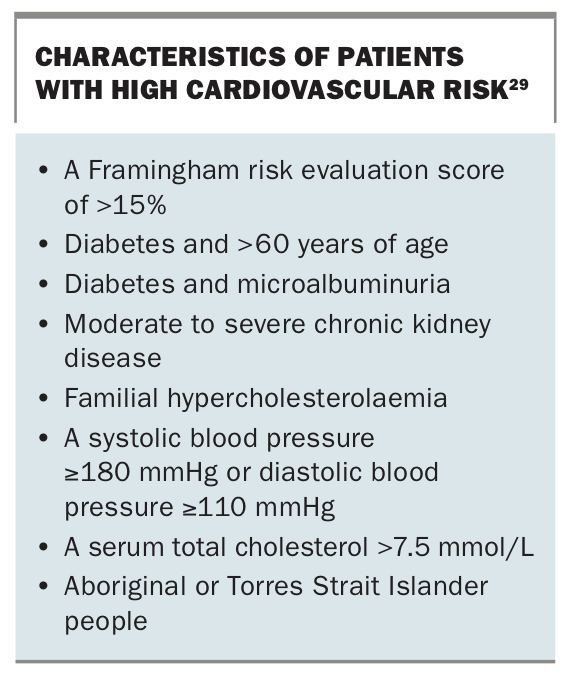
- Antiplatelet therapy is not routinely recommended for primary prevention of CVD in high-risk adults (Box), including those with diabetes.29-31
- Specific advice and support regarding diet, physical activity and smoking cessation remains the initial approach to cardiovascular risk reduction.29,30,32
- Adults with high cardiovascular risk should be simultaneously treated with blood pressure and lipid-lowering agents unless contraindicated or clinically inappropriate.29,30,32
- Target blood pressure is ≤130/80 mmHg in patients with diabetes and total cholesterol <4.0 mmol/L, low-density lipoprotein <2.0 mmol/L, high-density lipoprotein ≥1.0 mmol/L and triglycerides <2.0 mmol/L.29,30,32
- Response to treatment should be reviewed every six to 12 weeks, and medications adjusted as required, until either sufficient improvement or maximum tolerated dose is achieved.29
{kind=link}
Removal of aspirin as recommended therapy for primary prevention in patients with diabetes also aids in reducing the burden of polypharmacy and its accompanying potential for adverse events, which can be a common problem for patients with diabetes, who often have multiple comorbidities.
In accordance with recent cardiovascular outcome trials, diabetes management guidelines are now also recommending the addition of either a sodium-glucose cotransporter 2 (SGLT-2) inhibitor or a glucagon-like peptide-1 (GLP-1) receptor analogue in patients with diabetes who are either at high risk for, or already have, established CVD. This aims to not only improve glycaemic control, but also provide additional cardiovascular and mortality benefits to patients with diabetes.33
Conclusion
Aspirin has an established role for secondary prevention of CVD. Updated evidence does not support the routine use of aspirin for primary prevention among patients with diabetes because the risks of serious bleeding appear to counterbalance any modest reductions in cardiovascular events. MT