Enhancing influenza vaccination in older people


Influenza
Seasonal influenza disease can be particularly severe in older people, but conventional trivalent and quadrivalent inactivated influenza vaccines can be ineffective in this age group when influenza A(H3N2) strains predominate. New enhanced trivalent vaccines are available and should be used in people aged 65 years and over.
- In Australia, the vast majority of cases of serious influenza disease and influenza-related deaths occur in adults aged 65 years and over; long-term sequelae that impact on activities of daily living are also common in this group.
- Standard influenza vaccines induce suboptimal antibody titres and show suboptimal levels of effectiveness in older adults. Two enhanced influenza vaccines are now available in Australia and should be used in older people; both have a good safety profile.
- During the 2019 influenza season in Australia, an adjuvanted trivalent vaccine that has been shown to provide enhanced protection in older adults is recommended and funded under the National Immunisation Program (NIP) for people aged 65 years and over.
- A high-dose version of the standard trivalent vaccine also provides enhanced protection in older people and is recommended for use in this group but is not funded under the NIP this year.
- The additional benefit of extra influenza B coverage and hence the need for a quadrivalent vaccine in older people has not been established. However, the benefit would be substantially less than the additional protection provided by enhanced vaccines.
- Influenza vaccine coverage in older people is about 75% each year; general practice staff are key partners in increasing this level of vaccination.
Illness due to influenza virus infection poses a severe burden on Australian healthcare systems. Globally, the WHO estimates that seasonal influenza causes three to five million cases of severe illness and 290,000 to 650,000 deaths annually.1 Influenza is a disease that affects both industrialised and developing countries. Although data from the developing world are limited, it is estimated that each year 99% of deaths in children under 5 years of age with influenza-related lower respiratory tract infections occur in developing countries.2 However, influenza more often results in severe disease in people with chronic underlying conditions and in older people and most influenza-associated mortality occurs in older adults.3
In 2017, the largest nonpandemic influenza season on record in Australia, more than 90% of the reported 1100 influenza- related deaths were in adults aged over 65 years.4 Much of the impact of influenza in older people is hidden and manifests as previously undetected underlying medical conditions or as a worsening of existing conditions, especially cardiovascular disease.5 For example, acute influenza can lead to decompensation in patients with congestive heart failure or diabetes mellitus and to an increased risk of myocardial infarction and stroke. As patients with these conditions are rarely tested for influenza, the burden of disease is greatly underestimated.6
Influenza can present differently in older adults, who often have a lower incidence of fever, more frequent lower respiratory symptoms such as cough, wheezing and chest pain, and atypical disease, with anorexia, mental status changes or unexplained fever as the only presenting symptoms.7,8 Patients with underlying chronic obstructive pulmonary disease (COPD) may experience worsening respiratory status. Heart failure may be an unrecognised complication. Pneumonia is a relatively common complication, especially in people with chronic cardiopulmonary disease.
Of great importance are recent data that show influenza causing hospitalisation negatively affects functional status in older people and leads to a decline in capacity for activities of daily living after the infection.9 As populations age, the occurrence of permanent disabilities due to influenza-related illness is increasing, causing major suffering and mandating the search for effective prevention programs.
Influenza viruses
There are two major influenza virus types that cause human illness, influenza A and B viruses, each with their own characteristics and effect on different community groups. Most severe human illness is due to influenza A viruses, further subdivided into A(H1N1) and A(H3N2) subtypes according to the two surface proteins haemagglutinin (H) and neuraminidase (N). Influenza A has its greatest impact on older adults and young infants, whereas influenza B is more likely to occur in the under 20 years age group.10
The highest rates of influenza-related morbidity and mortality occur in people aged over 65 years infected with A(H3N2) strains. There is a direct relationship between seasons when an influenza A(H3N2) strain is the predominant strain in circulation and increased hospitalisations with influenza-associated respiratory and circulatory conditions.11
No link has been shown between levels of circulation of influenza B viruses and excess mortality or seasonal surges in hospitalisations.12
When I first diagnose a patient with diabetes, I don’t ask them if they feel like taking insulin. Similarly, in winter when flu vaccine becomes available, I tell patients it has arrived and that I will give it to them while they are there. I get very few discussions or refusals. This is best practice.
US geriatrician
Influenza vaccine responses in older people
Immunosenescence, an age-related decline in immune function, impairs the ability of older adults to fight natural infections and also results in suboptimal immune responses to influenza vaccines.13 Both adaptive and innate immunity decline with increasing age in the population aged over 65 years.
Although some studies have found little protection from the use of standard influenza vaccine in this older age group, conclusions are clouded by the mismatch in some years between viral strains in the vaccine and those circulating in the population, and the different outcomes evaluated. Indeed, studies have shown that inactivated influenza vaccine may halve the incidence of laboratory-proven and clinical influenza.14 Even when vaccination failed to stop infection, it did decrease the severity of disease, as evidenced by lower hospitalisation rates and fewer admissions to intensive care units.15
Influenza vaccine effectiveness in older people varies with the circulating strain, being lower in years when influenza A(H3N2) predominates. Older adults have the poorest antibody-mediated immune responses to the A(H3N2) components of vaccines and also display lower cellular immunity to influenza A(H3N2).
Influenza vaccines
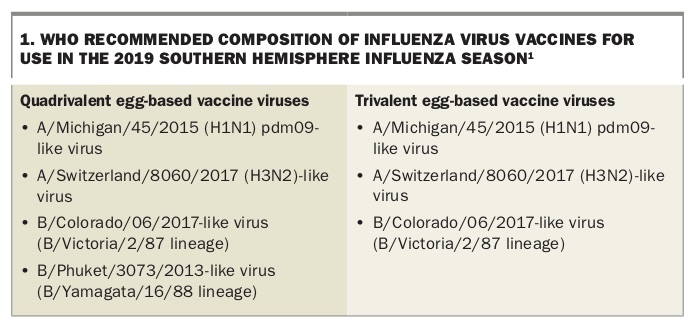
Influenza vaccination is recommended and funded in Australia for all people aged 65 years and over. Previously, the most widely used influenza vaccines were trivalent formulations of inactivated haemagglutinin and neuraminidase antigens representative of the predominant A(H1N1), A(H3N2) and B strains, using the selected strains recommended by WHO for each season. More recently, both influenza B strain lineages (B/Yamagata and B/Victoria) have been included in new quadrivalent influenza vaccines. The WHO recommended strains for the trivalent and quadrivalent influenza vaccines for the 2019 southern hemisphere influenza season are listed in Box 1.
{kind=link}
Quadrivalent influenza vaccines may have benefit in children, who experience the highest burden of influenza B. However, they are relatively less advantageous for older people, in whom most serious disease is attributable to influenza A(H3N2), with little disease or serious disease being due to influenza B. Adding additional lineage coverage for influenza B to vaccines for older people would be of little benefit, as it has no impact on overcoming immunosenescence and improving effectiveness against influenza A disease.
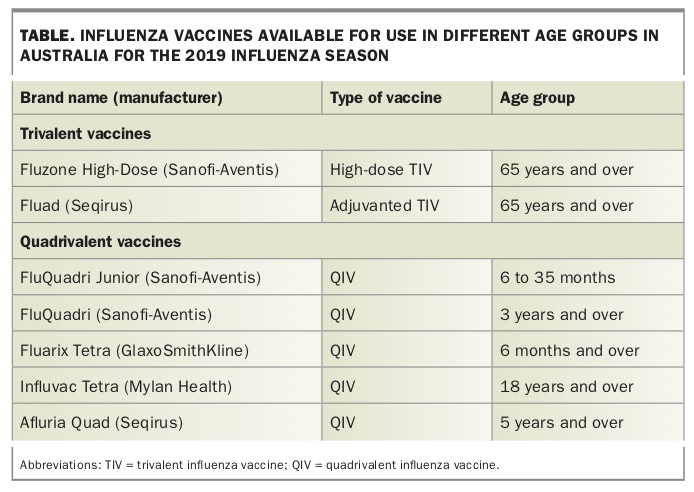
Enhanced vaccines are required to provide adequate protection in older people.16,17 The Australian Government funded two new enhanced vaccines for people aged 65 years and over for the first time in 2018: an adjuvanted trivalent vaccine and a high-dose trivalent vaccine. Both vaccines showed improved effectiveness in real-world studies and elicited greater antibody responses in clinical trials. In September 2017, the Chief Medical Officer of Australia issued guidance on the importance of vaccinating older patients and also of using the new enhanced vaccines in this specific age group.18 Vaccines available in Australia in 2019 are shown in the Table.
{kind=link}
Enhanced influenza vaccines
Adjuvanted influenza vaccine
The adjuvanted trivalent influenza vaccine not only enhances the magnitude of the immune response but also broadens the response to improve protection during years when vaccine strains do not match circulating viruses. The adjuvant MF59 is an oil-in-water emulsion based on squalene, which enhances both antigen presentation and T-cell priming. Importantly, a number of international studies of adjuvanted influenza vaccine found a significant increase in the response to influenza A(H3N2) in people aged over 65 years.19,20 In 2019, the adjuvanted trivalent influenza vaccine is recommended as one of the two preferred vaccines for use in older people and is funded under the National Immunisation Program (NIP).
High-dose influenza vaccine
The high-dose trivalent influenza vaccine contains 60 mcg haemagglutinin per strain, instead of 15 mcg, and produces a dose-dependent increase in antibody response. Several studies have shown that it induces higher immune responses in older adults, with improved efficacy in clinical trials against influenza infection compared with the standard trivalent influenza vaccine. The high-dose vaccine also shows improved efficacy in clinical trials.21,22 Although high-dose influenza vaccine is recommended as a preferred vaccine for use in older people, it is not funded under the NIP in 2019.
Benefit of enhanced vaccines.
The attributable additional benefit of using an enhanced vaccine will vary from year to year depending on the predominant circulating strain (H3N2 or not) and the degree of match with the vaccine strains. However, in several real-life effectiveness studies in older people, enhanced vaccines have shown on average about 25% extra protection against disease and even higher additional protection against severe disease.20 Given the burden of disease associated with influenza in older people, this additional protection has enormous implications. During the severe 2013-14 influenza season in the US, the Centers for Disease Control and Prevention estimated that each 5% increase in vaccine effectiveness saved 86,000 hospitalisations in that year.
Safety of enhanced vaccines
In the two decades since the adjuvanted trivalent influenza vaccine was licensed, it has established a good safety record. An integrated analysis by the manufacturer of data from 20,000 vaccinees in the safety database obtained in the strict monitoring conditions of clinical trials of the vaccine revealed a higher risk of solicited local or systemic reactions, but no increase in severe adverse effects or longer-term consequences.23
Similarly, safety studies with high-dose trivalent influenza vaccine showed a small increase in local injection site reactions, most commonly pain at the site, and some increase in systemic adverse event rates. These reactions were largely mild and self-limiting. Again, no increase in the rate of serious adverse events was seen.24
Timing of influenza vaccination in older people
Recent data on influenza vaccine effectiveness over the course of the influenza season suggest that in a predominant H3N2 season, vaccine effectiveness falls about 8% per month; vaccine may no longer be effective four months after administration. This has led to debate about delaying vaccination until around May in older people in Australia to ensure they remain protected later in the influenza season.
Data show continued immunological markers for more than six months after administration of adjuvanted trivalent influenza vaccine, so timing may be less crucial with this vaccine. Nevertheless, substantial influenza activity before June is uncommon, and delaying vaccine until May appears reasonable.
Role of general practice
Vaccination is an important component of promoting healthy ageing. Current coverage rates with influenza vaccine in older people are too low, at about 75%.25 This coverage level would not be accepted in children, and in view of the clear benefit of vaccination and the amount of influenza- associated disease in older people, 75% coverage should not be accepted in this age group either. GPs are key to improving vaccination rates.26 Having a clear rationale about the high risk of influenza in older people and the benefit of vaccination with a new safe enhanced vaccine, and sharing this with all patients in target groups is important. This is particularly the case for those with chronic disease. Two case studies on influenza vaccination that illustrate this approach are shown in Box 2.
{kind=link}
Conclusion
Influenza remains a major public health problem in Australia that causes significant severe disease, long-term disability and mortality in older people. The theoretical advantages of increasing the antigen content (high-dose trivalent influenza vaccine) or adding an adjuvant (adjuvanted trivalent influenza vaccine) has translated in real-world studies to improved protection for older people.
For this reason, the Australian Government Department of Health has made available and recommended the use of high-dose trivalent influenza vaccine or adjuvanted trivalent influenza vaccine in people aged 65 years and over. Adjuvanted trivalent influenza vaccine is also currently funded under the NIP for this age group. Healthcare practitioners should note recent recommendations and ensure that their older patients are offered seasonal vaccine designed specifically to protect older people. MT