Strategies to increase vaccination rates in older people


Immunisation
Seniors' health
Coverage levels for recommended vaccines in older adults fall well below those in children. An important driver of vaccination is a recommendation from the person’s GP. Tips for talking about vaccines and addressing patient misconceptions and specific practice strategies may help GPs increase vaccination rates among their older patients.
- Vaccination rates for recommended vaccines in older adults fall well below rates seen in children.
- One of the most influential drivers of vaccination is a recommendation from the person’s GP.
- GPs can help increase vaccination rates by informing their older patients about the severity of vaccine-preventable diseases and the safety and effectiveness of vaccines.
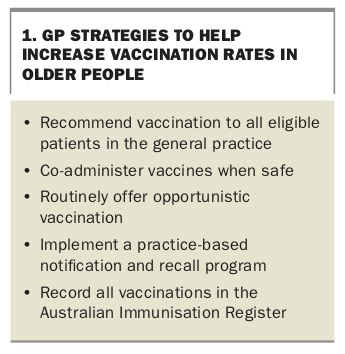
- Other strategies to help increase vaccination rates include: – co-administration of vaccines – opportunistic vaccination – patient notification and recall programs.
- All vaccinations of older people can now be recorded in the expanded Australian Immunisation Register.
Australia has not achieved acceptable vaccination rates in older people for vaccines listed on the National Immunisation Program (NIP). More can be done to achieve vaccine coverage comparable to that in children, of whom about 94% are fully vaccinated. Suggested strategies for GPs to help improve vaccination rates among older people are summarised in Box 1 and discussed in this article.
{kind=link}
Recommend vaccination to all eligible patients
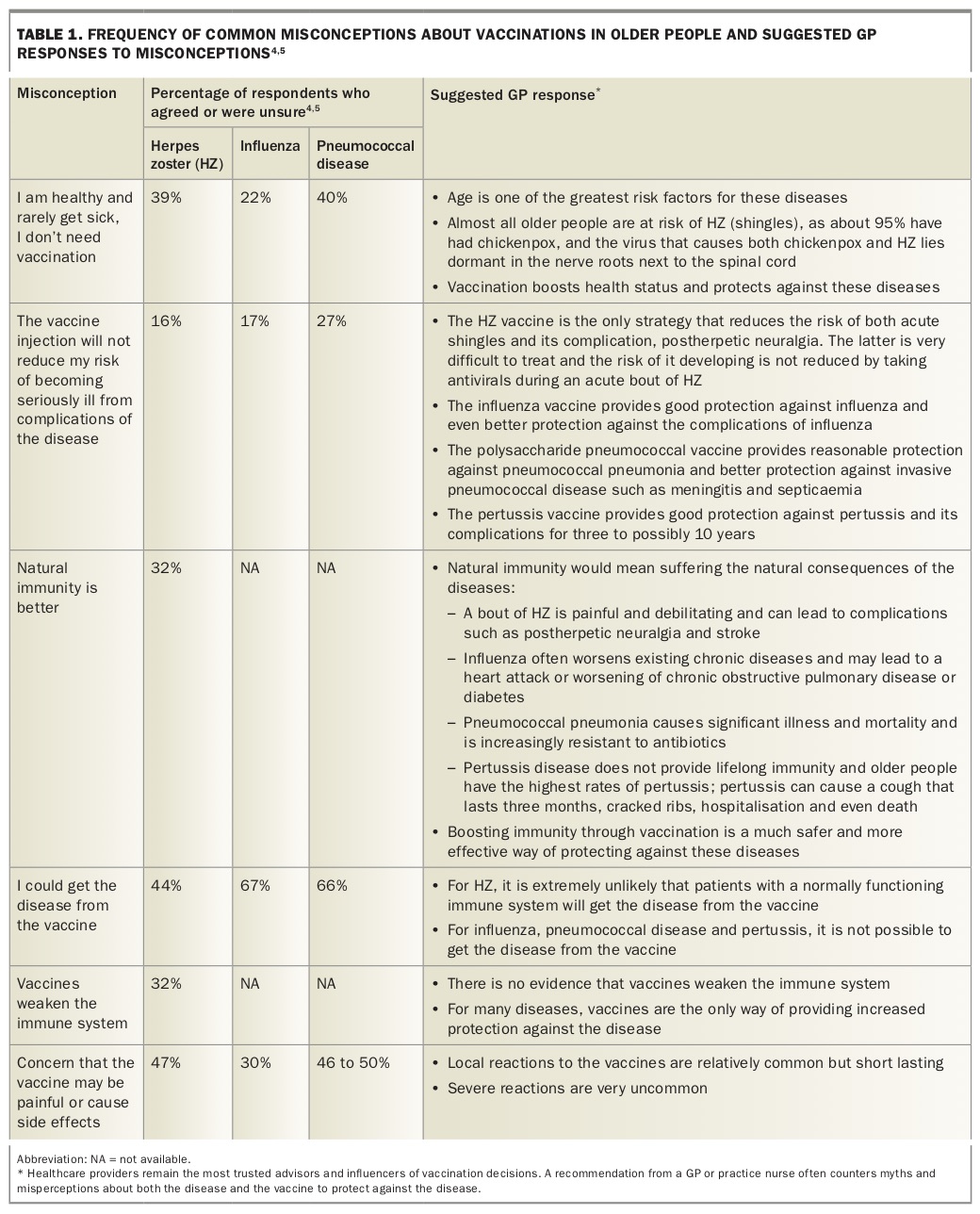
Studies show that the most influential driver of vaccination is a recommendation from the person’s healthcare provider. This can increase the likelihood of vaccination against influenza, pneumococcal disease and herpes zoster (HZ) 11-fold.1-5 However, patient surveys have found that myths and misconceptions about vaccines in older people are common (Table 1).4,5 These myths and misconceptions can act as barriers to vaccination. They include beliefs that:
{kind=link}
- healthy people are not at risk of the disease targeted by the vaccine
- the disease is not serious
- the vaccine is ineffective or can itself cause the targeted disease
- natural immunity is better
- the risk of adverse effects is too high.
These misconceptions can be addressed by high-quality educational programs, ranging from one-on-one discussions through to societal-level campaigns. Both healthcare providers and patients need evidence-based information on the risks associated with the various vaccine-preventable diseases, the effectiveness and safety of the vaccines and ways of achieving high levels of vaccine coverage.
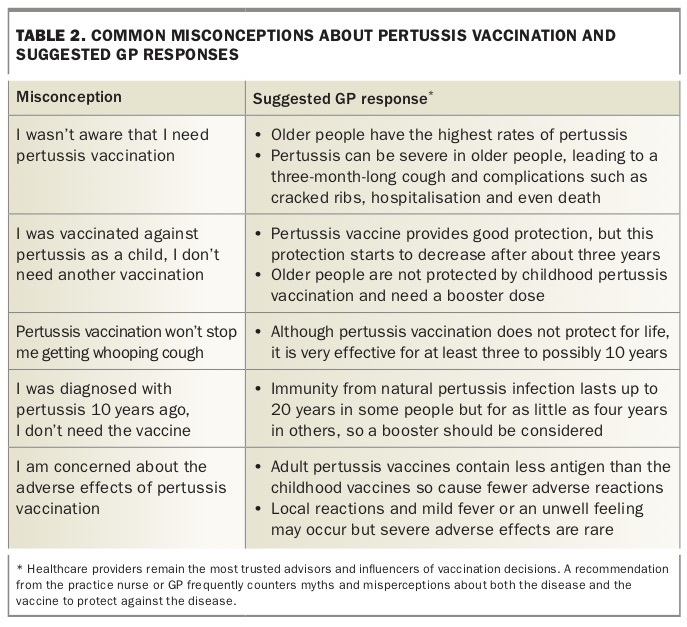
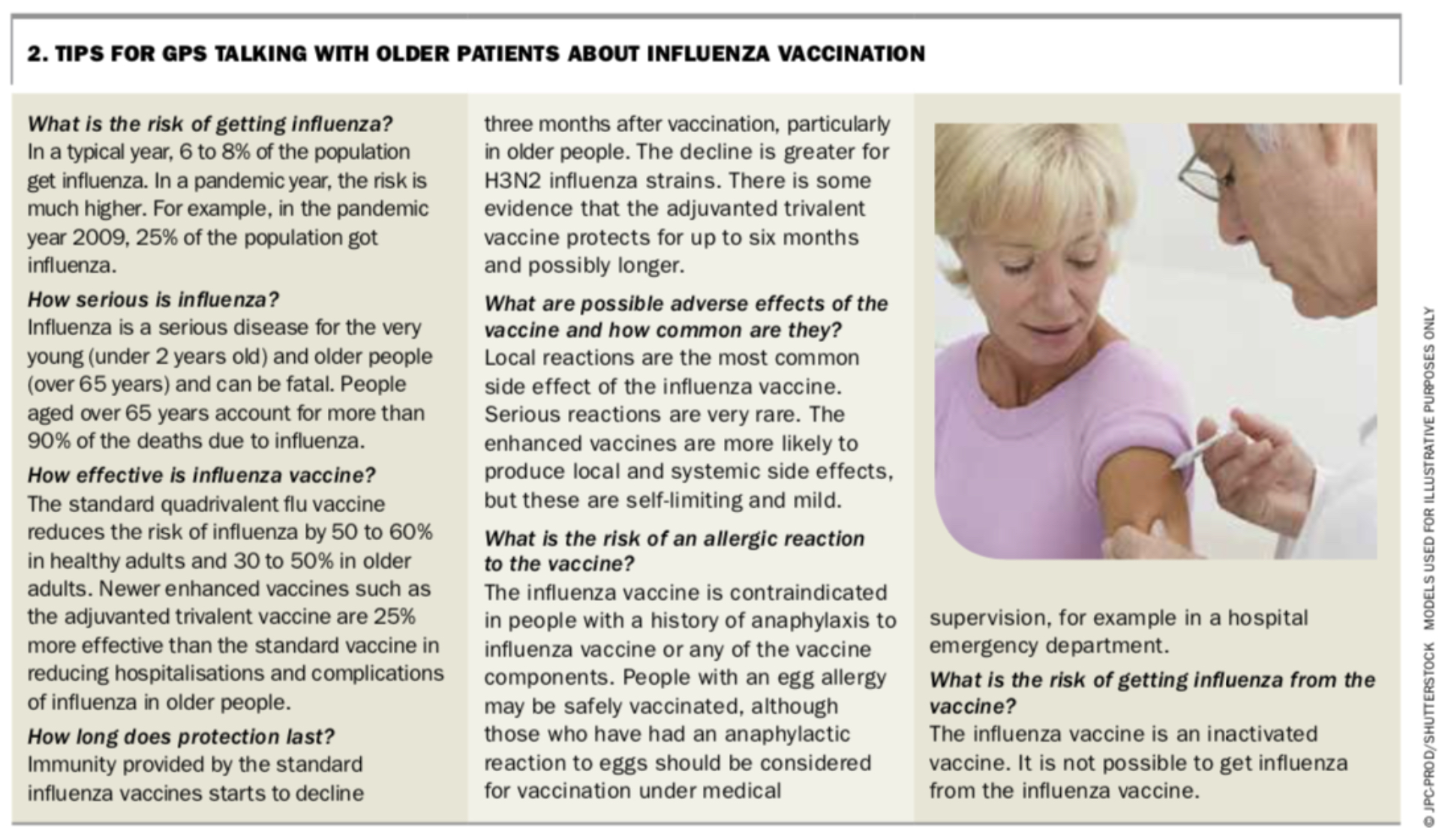
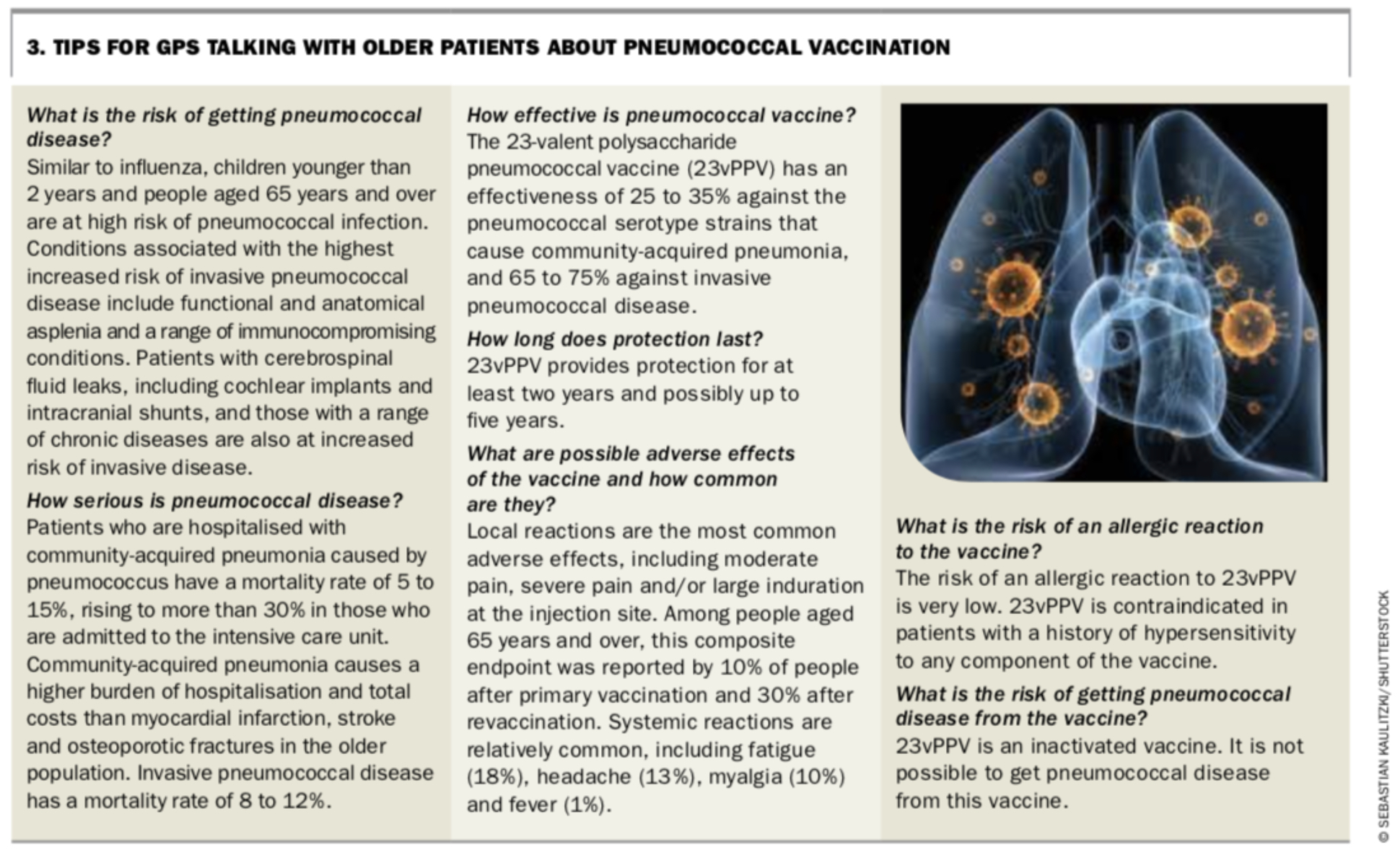
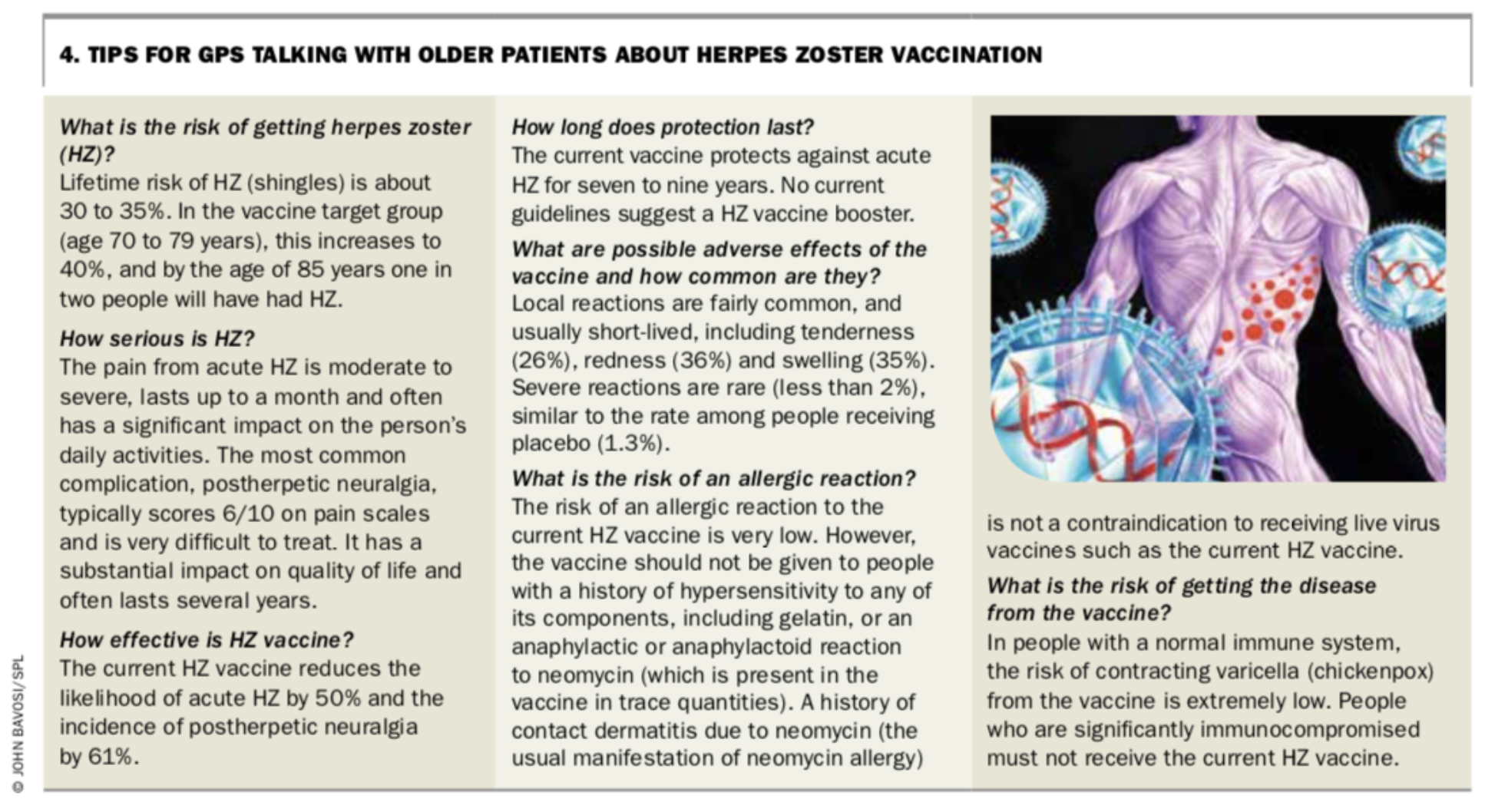
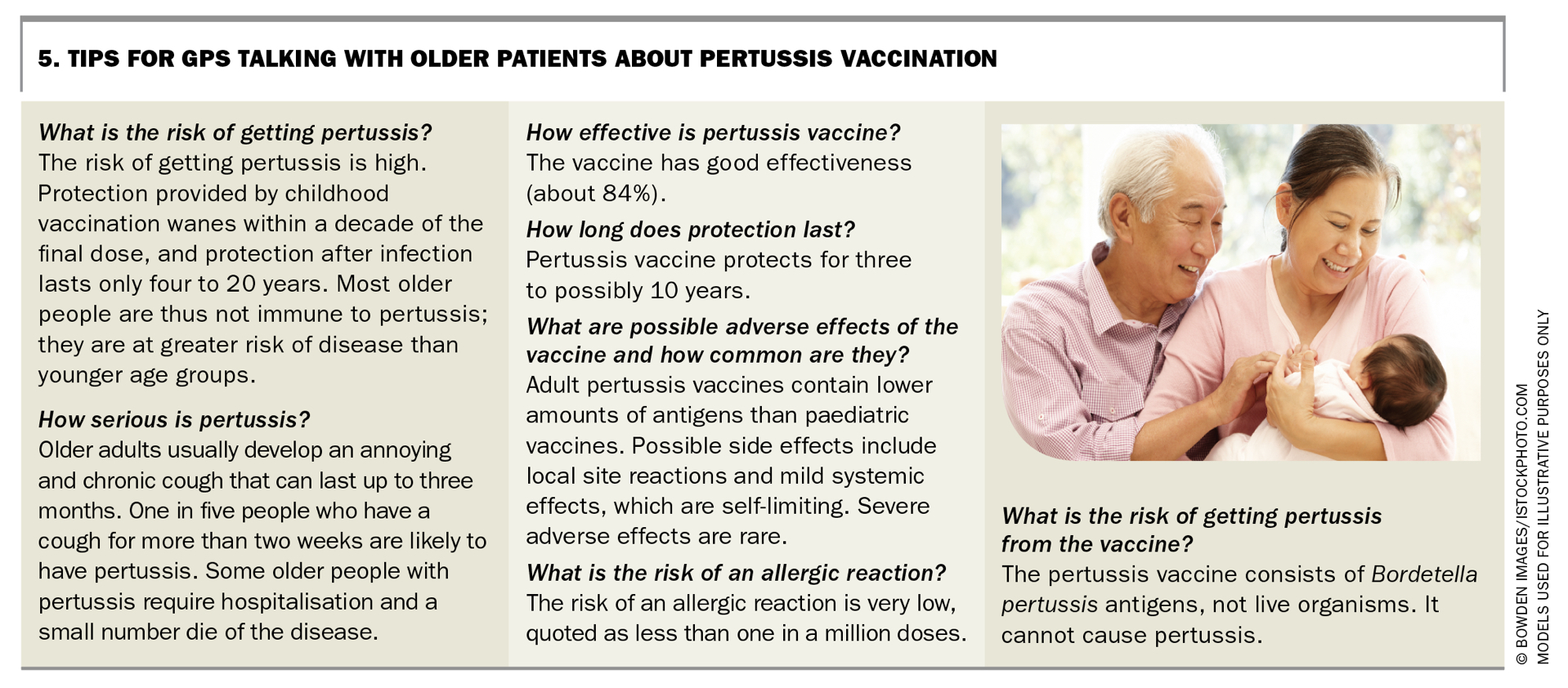
Some suggested GP responses to common patient misconceptions about vaccination are shown in Table 1 and Table 2. Tips for GPs talking with patients about influenza, pneumococcal, HZ and pertussis vaccination are shown in Box 2, Box 3, Box 4 and Box 5. A suggested patient handout about vaccination for people aged 65 years and over appears on page 33 of this supplement.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Other useful resources include the Australian Immunisation Handbook, National Centre for Immunisation Research and Surveillance fact sheets and the Australian and New Zealand Society for Geriatric Medicine position statement on Immunisation of Older People.6-8
Co-administer vaccines
Presentation of a patient for one vaccine, such as annual influenza vaccine, provides an opportunity to check current vaccination status and offer other vaccines. Despite some product information advice to the contrary, pneumococcal vaccine can be given at the same time as the live attenuated HZ vaccine (although they are best administered in different arms), and each of these can be given at the same time as influenza vaccine. However, the safety and efficacy of administration of all three together has not been established.
Support opportunistic vaccination
Other strategies that can help GPs increase vaccine coverage among older people in their practices include opportunistic vaccination and notification and reminder programs, which can act synergistically. Opportunistic vaccination captures the patient when they attend the practice; the vast majority of the older population visit a GP several times a year.4,9
A successful opportunistic vaccination program requires some planning. Suggested steps for GPs and practice staff to support opportunistic vaccination include:
- Display posters and leaflets about vaccinations for older people in the GP’s waiting and consulting rooms.
- Routinely inform all eligible patients about each vaccine. A strategy is for the practice nurse to flag attending patients who are due for a vaccine in the appointment system after checking their vaccination status in the electronic record.
- Integrate vaccination into health assessments (e.g. ensure HZ vaccination is part of the age 75 years health assessment).
- Administer the vaccine and document this in the patient’s electronic health record as well as the Australian Immunisation Register (AIR, see below).
- Give the patient information to take away that is relevant to their knowledge, interest and concerns or direct them to online patient information sites (e.g. www.ncirs.org.au/public, www.chop.edu/centers-programs/vaccine-education-center).
- Identify likely low-vaccination groups. Patients who attend the practice infrequently are less likely to receive recommended preventive care, such as vaccines. Reception staff can use the appointment system to generate a list of infrequent attenders (e.g. have not attended in the previous 12 to 18 months). This group could be sent an SMS or other electronic reminder suggesting they attend for vaccination.
- Implement standing orders to guide staff such as practice nurses to offer a range of vaccines after appropriate checks of eligibility and contraindications. Practice nurses could then administer the vaccine without the GP being present. Although this might mean patients are not billed, it will increase patient convenience and could be done in association with a GP appointment. For example, patients could see the practice nurse for vaccination while waiting to see the GP.
Occasionally, patients have strong views about vaccination and resist offers of vaccines. Although these views need to be respected, it is useful to understand the patient’s exact concerns and whether they might be amenable to further information. A strategy to help avoid giving offence when repeatedly offering a vaccine is to say ‘I understand your concerns about the […] vaccine and respect your decision. I find from time to time that patients change their mind, so raising the issue gives them an opportunity to discuss their wishes, address any concerns and possibly accept the vaccine if they wish’.
Implement notification and recall programs
Vaccination rates are likely to remain suboptimal, even with a planned opportunistic vaccination program, unless GPs also use a notification and recall strategy. This is particularly important for nonseasonal diseases, such as shingles. Suggested steps in a notification and recall/reminder program for GPs include:
- Appoint a co-ordinator. This increases the likelihood of teamwork, allocation of tasks and follow up of the impact.10,11
- Identify eligible patients. Practice software can be used to compile a list. GPs will need to determine whether they are the patient’s usual GP, for example by checking the patient’s electronic health record.
- Notify eligible patients about relevant vaccinations using one or more methods, ideally including an electronic strategy such as SMS messaging or an electronic reminder system. Examples of the latter include SmartVax (www.smartvax.com.au) and HotDoc (https://hotdoc.com.au). A birthday card reminder is another way of prompting patients to attend for vaccination.
- Administer the vaccine and record the vaccination in the patient’s electronic record as well as the AIR. It can also be useful to give patients a small immunisation card that lists all the vaccines they have received. These cards are available from most state health departments and have the advantage of providing a portable summary of the individual’s vaccine history.
- Send ongoing recalls and reminders to any missed or new eligible patients at appropriate intervals. A tailored phone call or SMS from the practice nurse coupled with a strong GP recommendation will further increase coverage rates and potentially save the practice the time and cost of sending repeated letters.10 It is important to document reminders in the patient’s electronic health record. Sending reminders is made easier for some patient target groups if they are captured in the electronic practice register; it is worthwhile setting up disease and high-risk practice registers for some conditions.10
Australian Immunisation Register
The AIR was extended to all age groups from November 2016, replacing the Australian Childhood Immunisation Register.12 The AIR can record vaccinations given through general practice and community clinics, including vaccines funded under the NIP and privately funded vaccinations. It provides an opportunity to record vaccinations of older people and to make this information available to other GPs and healthcare practitioners, for example if the patient moves to a new general practice.
The data could also be used, when sufficiently complete and reliable, to identify and target regions achieving lower vaccination rates, and to identify high vaccination regions that can be further interrogated to demonstrate best practices.
Conclusion
Despite official recommendations on vaccination in older people and inclusion of many vaccines on the NIP, coverage levels in older adults are well below those in children. Strategies that might increase uptake of recommended vaccines among older people include government actions, such as listing all recommended vaccines on the NIP and improving national surveillance of vaccination coverage levels and disease rates in the older population to inform funding discussions. However, GPs also have the opportunity to help increase vaccination rates among their older patients. Suggested strategies include informing their older patients about the risks and potential severity of vaccine-preventable diseases and the safety and effectiveness of vaccines, co-administration of vaccines where this is safe, and adopting systematic practice strategies to support opportunistic vaccination and patient notification and recall systems. MT
References