How to optimise therapy for heart failure with reduced ejection fraction

Heart failure
Heart diseases
The prognosis for patients with heart failure is poor, with high rates of hospitalisation and mortality. It is essential to optimise pharmacotherapy and device therapies that improve the prognosis for patients with heart failure with reduced ejection fraction.
- Pharmacotherapy for heart failure with reduced ejection fraction principally comprises ACE inhibitors or angiotensin receptor blockers (ARBs), followed by beta blockers, mineralocorticoid receptor antagonists and angiotensin receptor-neprilysin inhibitors (ARNIs).
- These medications should be uptitrated to target doses to achieve optimal benefit.
- ARBs should be considered only for patients who are intolerant of ACE inhibitors.
- ARNIs are indicated if patients with heart failure remain symptomatic despite treatment with an ACE inhibitor or ARB.
- Several devices, including implantable cardioverter defibrillators and left ventricular assist devices, have also been shown to improve outcomes in patients with heart failure.
- Patients who have been hospitalised with heart failure should be reviewed by their GP, cardiologist and heart failure nurse within seven days of discharge.
Heart failure (HF) is associated with high mortality and hospitalisation rates. A third of patients with HF die within one year of discharge from hospital and a quarter of patients are readmitted within 30 days of discharge.1-3 However, these outcomes can be improved for patients with HF with reduced ejection fraction (HFrEF) through optimisation of pharmacotherapy and device therapy.
The cornerstone of pharmacotherapy for HFrEF comprises ACE inhibitors, or angiotensin receptor blockers (ARBs) if the patient is intolerant of ACE inhibitors, followed by beta blockers, then mineralocorticoid receptor antagonists (MRAs), then angiotensin receptor-neprilysin inhibitors (ARNIs).4 However, less than a third of patients are prescribed at least three of the recommended first-line medications for HF.5 Clinicians should aim to uptitrate the dose of these medications to target doses to ensure optimal benefit.
This article focuses on pharmacotherapy and devices associated with improved outcomes in patients diagnosed with HFrEF, along with the follow up needed after patients have been hospitalised for HF.
Pharmacotherapy
ACE inhibitors and angiotensin receptor blockers
ACE inhibitors reduce mortality, hospitalisation and symptoms, and are first-line therapy in patients with HF, including asymptomatic patients.4 In patients with HF, they reduce the risk of myocardial infarction by 20%, cardiovascular death by 26% and overall mortality by 16%.6
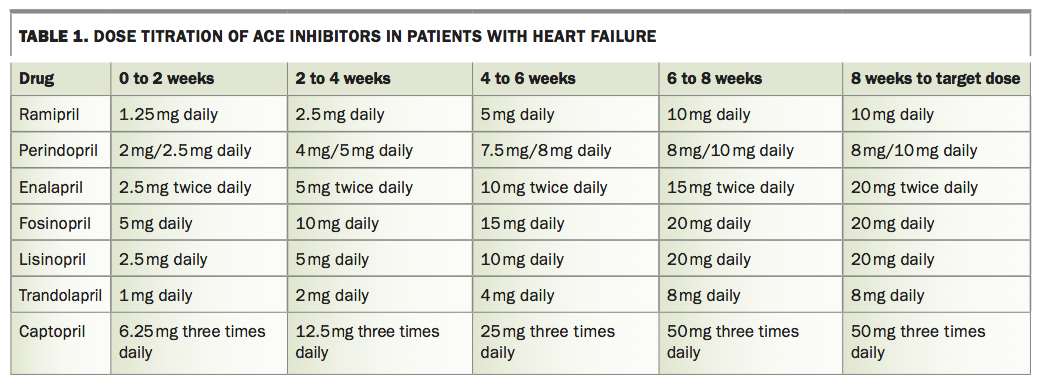
ACE inhibitors should be initiated at low doses and uptitrated over three to four weeks to the highest tolerated dose (Table 1). Renal function and electrolyte levels should be checked two weeks after commencement, then after one month and then every three to six months. Volume status should be assessed and the need for other drugs that lower blood pressure or affect renal function and potassium levels, such as calcium channel blockers, nitrates, NSAIDs, diuretics and potassium supplements, should be reviewed if the patient develops symptomatic hypotension, their estimated glomerular filtration rate (eGFR) decreases by more than 30% or serum potassium level rises above 5.5 mmol/L. If unsuccessful, ACE inhibitors may need to be decreased or discontinued. Reasons for discontinuation include cough (in 20% of patients), symptomatic hypotension, renal or electrolyte disturbance or angioedema. Daytime hypotension may be reduced by taking the ACE inhibitor at night.
{kind=link}
ARBs show similar reductions in mortality, hospitalisation and symptoms as ACE inhibitors.4 They should be considered only for patients who are intolerant of ACE inhibitors, as most of the evidence is based on ACE inhibitors and the largest trial comparing the two agents was slightly in favour of ACE inhibitors.7 Recommendations for titration of ARB doses and measurement of renal function and electrolyte levels are similar to those for ACE inhibitors.
Beta blockers
Beta blockers are indicated in all New York Heart Association classes of HF and inhibit the adverse effects of sympathetic activation. They reduce mortality by about 34% (on top of background therapy including ACE inhibitors or ARBs).4 HF-specific beta blockers include carvedilol, bisoprolol, nebivolol and extended-release metoprolol.4
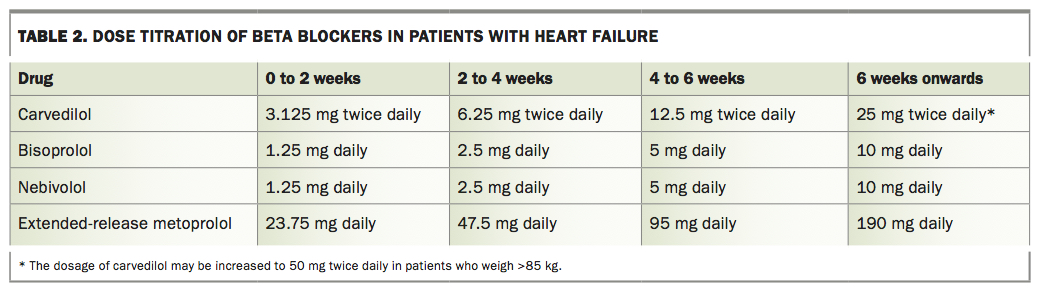
Beta blockers should be commenced at low doses once the patient is euvolaemic and uptitrated over one to two months (Table 2). Patients should be haemodynamically stable with a systolic blood pressure greater than 85 mmHg (without postural drop), minimal peripheral oedema and no pulmonary crackles before prescribing beta blockers. Rapid uptitration may lead to adverse effects or inappropriate discontinuation. The beta blocker dose may need to be reduced if the patient’s heart rate falls below 50 beats/min, after first undertaking an ECG to document the rhythm and reviewing other drugs that lower heart rate (e.g. digoxin and amiodarone). Hypotension can be treated by reducing diuretics or other vasodilators, rather than reducing the beta blocker dose. Beta blockers should generally be avoided in patients whose heart rate is higher than the systolic blood pressure; these patients are dependent on their heart rate to maintain their blood pressure, and beta blockers may precipitate acute decompensation.
{kind=link}
Beta blocker side effects include hypotension, fatigue, bronchoconstriction in patients with reversible airway obstruction (greater than 15% improvement in forced expiratory volume in one second with bronchodilators) and mild initial worsening of HF symptoms. Cardioselective beta blockers (e.g. bisoprolol, nebivolol) are tolerated by more than 85% of patients with chronic obstructive pulmonary disease without reversible airway obstruction.8 Patients with true asthma or who are receiving cortico-steroid treatment may not tolerate beta blockers. Combining beta blockers with an inhaled steroid and a long-acting muscarinic antagonist (e.g. tiotropium) may improve tolerability, but combining beta blockers and beta agonists may be counterproductive. Long-acting muscarinic anta-gonists may reduce bronchoconstriction in response to pulmonary congestion.
Nebivolol has been shown to be effective in patients over 70 years of age, regardless of ejection fraction, and is the most beta-1-selective beta blocker.4 It also has a nitrate-like moiety that can be useful in treating secondary pulmonary hypertension and myocardial bridging (and erectile dysfunction). Because of its alpha-blocking effects, carvedilol is very effective in patients who have elevated blood pressure. The alpha-blocking effect of carvedilol may cause rhinorrhoea, diarrhoea or urinary incontinence, which is not the case with beta-1-selective agents. Beta-1-selective beta blockers without vasodilatory effect, such as bisoprolol or extended-release metoprolol, may be more appropriate in patients who are tachycardic and relatively hypotensive, particularly if they have postural hypotension.
Mineralocorticoid receptor antagonists
Aldosterone antagonism has been shown to reduce mortality and morbidity in all classes of HF, including after myocardial infarction.4 Eplerenone is a selective MRA that, unlike spironolactone, does not cause gynaecomastia. Monitoring of electrolyte levels and renal function (at one week after initiation, then one month, then three-monthly) is important because MRAs can cause hyperkalaemia. These drugs are relatively contraindicated in patients with severe renal impairment. Low doses of spironolactone (25 mg daily) are recommended for patients with mild to moderate renal impairment (one to three times a week if eGFR is less than 40 mL/minute/1.73m2).9 When combined with ACE inhibitors, ARBs or other diuretics, they cause synergistic neurohormonal blockade and diuresis, so renal function and electrolyte levels should be monitored carefully.
Angiotensin receptor-neprilysin inhibitors
ARNIs act on the renin-angiotensin-aldosterone system and the neprilysin peptide system. They are a combination of valsartan, an ARB that blocks the angio-tensin II receptor type 1, and sacubitril, which is a prodrug that is converted into a neprilysin inhibitor, promoting a higher concentration of circulating natriuretic peptides. It is recommended that symptomatic patients diagnosed with HFrEF with a left ventricular ejection fraction (LVEF) of less than or equal to 40% are prescribed an ARNI to replace ACE inhibitors and ARBs.4 To minimise the risk of angioedema, it is recommended that ACE inhibitors be ceased for at least 36 hours before an ARNI is initiated. ARNIs are indicated only if patients with HF remain symptomatic despite treatment with an ACE inhibitor or ARB.
The ARNI dose should be gradually increased every two to four weeks until the optimal dose is reached. It may be useful to stop or reduce vasodilators to ‘buy’ blood pressure if a patient is hypotensive. Unless a patient has fluid overload, reducing the dose of diuretics may also help avoid hypotension and dehydration. If a patient cannot tolerate uptitration of the ARNI dose, it may be necessary to initially increase the night-time dose, but not the morning dose, until further review; however, once-daily dosing is not recommended. Initiation of an ARNI rather than an ACE inhibitor or ARB can be considered for patients hospitalised with new-onset HF or decompensated congestive HF to reduce the short-term elevations of natriuretic peptide levels and possibly the risk of rehospitalisation.10 Adverse effects of ARNIs include symptomatic hypotension, hyperkalaemia, renal impairment, cough and, rarely, angioedema.
Diuretics
Diuretics, such as furosemide, treat congestive symptoms by preventing sodium accumulation and reducing plasma volume, venous return and cardiac preload. They have not been shown to improve survival.4 In patients with volume overload, a reasonable goal is weight reduction of 1.0 kg/day. Diuretics should be used sparingly, and dose reduction can be attempted carefully. Diuretic reduction may allow initiation of drugs with a proven mortality benefit (e.g. beta blockers and ACE inhibitors). Diuretics stimulate the renin–angiotensin system and aldosterone production, increase sympathetic tone, cause low potassium, magnesium and sodium levels, worsen renal function and exacerbate postural hypotension.
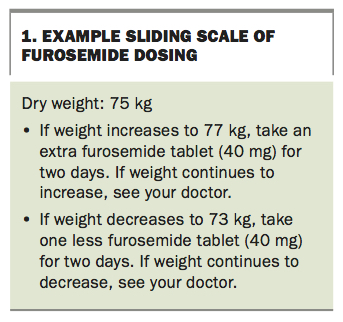
Once patients are managing their HF, a sliding scale that enables patients to adjust the dose of furosemide according to their weight can be developed. Box 1 gives an example of a sliding scale of furosemide dose.
{kind=link}
If the patient is already receiving an MRA and has persistent congestion that is resistant to furosemide, rather than changing to another loop diuretic with a similar mechanism of action, it is recommended to first slowly maximise the oral dose (up to 160 mg every morning and midday) and consider intravenous furosemide. If the patient’s fluid overload persists, addition of hydrochlorothiazide (25 mg one to three times a week) may be useful. In patients with extremely resistant congestion, addition of acetazolamide (250 mg one to three times a week) may be helpful in achieving diuresis. Electrolytes and renal function should be closely monitored in such patients.
Ivabradine
Ivabradine is a sinus node inhibitor that usually lowers the heart rate by 12% (i.e. 8 beats/minute) without a reduction in blood pressure or acute changes in cardio-vascular haemodynamics. It reduces the rate of spontaneous depolarisation of the sinoatrial node and is therefore only effective if the patient is in sinus rhythm. Ivabradine is recommended for patients with HFrEF, an LVEF of 35% or below and a sinus rate of 70 beats/minute or greater who are receiving the maximal tolerated dose of a beta blocker, or who cannot tolerate a beta blocker because of true asthma or hypotension.
Ivabradine has been shown in the Ivabradine and Outcomes in Chronic Heart Failure (SHIFT) study to reduce cardiovascular mortality and HF hospitalisation in patients with an LVEF less than 40% and heart rate greater than 70 beats/min (in sinus rhythm) and to improve survival if patients have a heart rate above 77 beats/min.11 Ivabradine should not be used in haemo-dynamically unstable patients. In the Study Assessing the Morbidity-Mortality Benefits of the If Inhibitor Ivabradine in Patients with Coronary Artery Disease (SIGNIFY), ivabradine was associated with a non-significant increase in the chance of developing atrial fibrillation and subsequent stroke compared with placebo.12
Digoxin
Digoxin reduces symptoms (fatigue, dyspnoea and exercise intolerance) in patients with HF and reduces hospitalisation in patients with symptoms that persist despite the above therapies, but it has no effect on mortality.4 Digoxin is particularly valuable when the patient has atrial fibrillation. Low doses (e.g. 62.5 mcg daily, or every two to three days in those with renal impairment) are recommended. Rather than using beta blockers in patients whose heart rate is higher than their systolic blood pressure, digoxin with or without amiodarone can be useful to stabilise the patient until a beta blocker can be added later, when the digoxin-amiodarone can then be withdrawn.
Other drug therapies
Nitrates and hydralazine
When used in combination, nitrates and hydralazine provide vasodilation in patients who are intolerant of ACE inhibitors and ARBs. They are useful in patients with significant renal impairment or hyperkalaemia, as they do not worsen renal function or cause electrolyte abnormalities.
Nitrates reduce nocturnal dyspnoea, peripheral oedema, secondary pulmonary hypertension and myocardial ischaemia via venodilation, as well as improving venous capacitance and reducing right ventricular preload.6,13 Nitrate patches are less well absorbed in patients with HF because of poor peripheral perfusion. Isosorbide mononitrate can be started at a dose of 30 mg at night, titrating to 60 mg and later 120 mg over one to two weeks.
Hydralazine reduces nitrate tolerance, improves nitrate sensitivity and controls hypertension in patients with HF not adequately controlled using first-line medications. Hydralazine can be started at a dose of 12.5 mg twice daily and increased to a maximum of 100 mg three times daily over one to two months. Hydralazine can cause drug-induced lupus, so antihistone antibodies should be checked every three to six months as part of extractable nuclear antigen antibody tests.
Amiodarone
Amiodarone has not been shown to reduce mortality but may control atrial and ventricular arrhythmias in patients with HF. Complications include thyroid dysfunction, pulmonary fibrosis, hepatic dysfunction, corneal deposits, peripheral neuropathy, photosensitivity and skin discolouration.14 Amiodarone should be initiated by, or in consultation with, a specialist. Intravenous amiodarone should be avoided in haemodynamically unstable patients because it may cause a sudden drop in systolic blood pressure.
Anticoagulants
Warfarin, dabigatran, rivaroxaban or apixaban is indicated in patients with HF who have atrial fibrillation.4 Patients in sinus rhythm with ischaemic cardiomyopathy should receive aspirin, but there is no evidence for the use of anticoagulants or antiplatelets in patients with nonischaemic cardiomyopathy in sinus rhythm.13
SGLT-2 inhibitors
Sodium-glucose co-transporter-2 (SGLT-2) inhibitors should be considered for patients with type 2 diabetes who are receiving metformin and whose glycated haemoglobin level is greater than 7.0%, to prevent or delay the onset of HF. They are not currently indicated for the treatment of HF, although there is increasing evidence that patients with HF who receive SGLT-2 inhibitors benefit from reductions in HF hospitalisation and cardiovascular mortality, regardless of whether they have diabetes.15
If starting SGLT-2 inhibitors, it is suggested to reduce or stop diuretics to avoid dehydration and excessive polyuria. There may be an early fall in eGFR, but there is then a plateau and the renal function tends to stabilise and not deteriorate, as it does in patients with diabetic kidney disease not treated with SGLT-2 inhibitors. There may also be an initial fall in blood pressure, requiring a reduction in blood pressure-lowering medications. Studies are ongoing to assess the use of SGLT-2 inhibitors in patients with HF but without diabetes. The effect of SGLT-2 inhibitors on glucose control, but not on cardiovascular outcomes, diminishes as renal function declines. The cardiovascular benefit persists down to an eGFR of 30 mL/minute/1.73m2 (although caution is needed with an eGFR between 30 and 45 mL/minute/1.73m2). Other glucose-lowering medication may need to be downtitrated to avoid hypoglycaemia.
SGLT-2 inhibitors should be avoided in patients with type 1 diabetes or if patients develop diarrhoea or other intercurrent illnesses, to reduce the risk of euglycaemic diabetic ketoacidosis. SGLT-2 inhibitors should be omitted for three days before surgery and for similar periods before procedures that require fasting, such as coronary angiography.
Omega-3 acid ethyl esters
Use of omega-3 acid ethyl esters (1000 mg daily) has been shown to lead to a 9% reduction in mortality in patients with HF in the Effect of n-3 Polyunsaturated Fatty Acids in Patients with Chronic Heart Failure (GISSI-HF) trial.16
Timing and medications to avoid
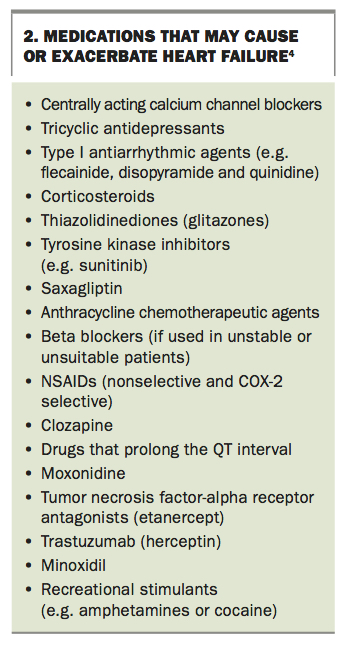
About 80% of sudden deaths, pulmonary oedemas and myocardial infarctions occur between 3 am and 8 am.17 The use of once-daily ACE inhibitors, ARBs, beta blockers and nitrates at night, rather than in the morning, may improve outcomes by antagonising the diurnal surges in adrenaline, noradrenaline, angiotensin II, cortisol and melatonin that contribute to the high risk in the early morning period. A summary of medications to avoid in patients with HF is given in Box 2.
{kind=link}
Management of refractory heart failure
Patients with systolic dysfunction and NYHA class III or IV symptoms who do not respond to optimal medical therapy or who experience rapid recurrence of symptoms may require hospitalisation for intensive management. A five-day course of intra-venous inotropic therapy (dobutamine or dopamine) may reduce symptoms, length of stay and rehospitalisation but may increase mortality. Dobutamine is best for left heart failure and pulmonary congestion in patients with HFrEF. Dopamine is preferred in patients with predominant right heart failure and renal impairment. Levosimendan works best if given after dobutamine and/or dopamine, as they increase intracellular calcium levels and levosimendan is a calcium sensitiser.
Device therapies
In addition to optimisation of pharmacotherapy, several devices have been shown to improve outcomes in patients with HF. Patients with prior cardiac arrest or ventricular arrhythmias and HF have a high risk of recurrent events. In patients with an LVEF less than 35%, an implantable cardioverter defibrillator, for both primary and secondary prevention of ventricular arrhythmia, leads to a reduction in mortality in both cases.4
Cardiac dyssynchrony is seen in about one-third of patients with HF and leads to further impairment of left ventricular function, abnormal remodelling and secondary mitral regurgitation. Pacing the left and right ventricles simultaneously with cardiac resynchronisation therapy has been shown to reduce symptoms, HF hospitalisation and mortality and improve functional capacity. The criteria for cardiac resynchronisation therapy are an LVEF less than 35% and evidence of cardiac dyssynchrony (QRS greater than or equal to 130 ms).4
Left ventricular assist devices were initially developed for use as a bridge to cardiac transplantation in patients with severe HF, and they have been successful in achieving this aim. However, the results of several trials conducted in experienced centres, including the Randomization Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) I and II trials, have shown these devices to also be effective as destination therapy.18,19 Newer devices are able to prolong life as well as improve quality of life. Complications of left ventricular assist devices include infections and haemorrhagic complications.20
Follow up in the community
Early follow up after hospitalisation for HF is essential. The most vulnerable period, when patients are at greatest risk of re-presenting to hospital, is within the first two weeks after discharge.21 Clinical guidelines therefore now recommend that patients with HF be reviewed by their GP, cardiologist and heart failure nurse within seven days of discharge.4
HF clinics are a key component of postdischarge multidisciplinary HF management and have led to an improvement in health care delivery for patients with HF. This is mainly due to patients having increased access to a multidisciplinary team, optimisation of evidence-based therapy, management of comorbidities and referral to specialist HF services, including disease management and exercise programs and nurse-led titration clinics. HF clinics facilitate early assessment and management of acute exacerbations and allow rapid access to HF expertise.
These clinics are in an ideal position to develop a tailored HF management plan to optimise patients’ quality of life and reduce hospital readmissions and mortality. It is essential that these clinics are flexible and responsive to patients’ needs during periods of decompensation, to facilitate rapid review within an appropriate timeframe and prevent readmissions.
HF clinics are now a standard component of postdischarge care for patients with HF, with studies showing their benefits. However, there is little evidence about the frequency of follow-up clinic visits, and this should be guided by the patient’s clinical status and ability to self-care and manage their HF in the community. Patients who require optimisation of pharmacotherapy or further diagnostic investigations, who have recently been hospitalised or have signs and symptoms of an acute exacerbation, or who need assessment for device therapy or heart transplantation will require frequent reassessment in the clinic. Patients with stable HF may only require visits every three to six months to check symptoms and diagnostic test results. Any patient who experiences an exacerbation of HF, including an HF-related hospital admission, must be referred back to the clinic with an early follow-up appointment within seven days of discharge.
Patient education is also a vital component of management after discharge and is usually provided by the HF nurse in an HF disease management program. If it is appropriate for patients to receive titration of key medications, they may be referred to the nurse-led titration clinic for rapid optimisation of these medications.
Primary care also plays a vital role in the management of patients with HF. It is essential that all patients admitted to hospital with HF are scheduled to see their GP within one week of discharge. Management of these patients should ideally be through a shared care model where a cardiologist and GP work collaboratively with the patient. Alternatively, the GP may decide to implement a chronic disease management plan to optimise the patient’s care in the community. GP referrals to an HF disease management program and/or a community-based HF exercise program have been shown to be beneficial in reducing hospitalisations and improving survival and quality of life.22 In Australia, most large metropolitan public hospitals are associated with an HF disease management program.23 Optimal management of patients with HF in the community is key to preventing readmissions.
Conclusion
The poor prognosis of HF, with its high mortality and hospitalisation rates, can be improved with optimisation of pharmacotherapy and device therapy. Newer therapies, such as ARNIs and SGLT-2 inhibitors, are now recommended in the management of HF. For patients with HF who have been hospitalised, early follow up after discharge is essential and should include review by the patient’s GP, cardiologist and heart failure nurse. HF clinics are a key component of postdischarge multidisciplinary HF management. MT
Professor Driscoll is supported by a Heart Foundation Future Leader Fellowship (100472) from the National Heart Foundation of Australia and has received speaker or consultancy fees from, and is a member of the advisory board for, Novartis.
Acknowledgement
Thanks to James Sindone for his contribution to this article.