What to expect in the end stages of heart failure

Heart failure
Heart diseases
Heart failure is a progressive life-limiting condition with worse five-year survival than many cancers and an uncertain trajectory in its advanced stages. Advance care planning and shared decision making for delivering palliative care are important but are often left too late or neglected. Early planning and open communication with patients and their caregivers are essential to ensuring best care for patients with end-stage heart failure.
- End-stage heart failure should be thought of as a terminal condition.
- The patient’s journey is characterised by a nonlinear deterioration, with an often unpredictable clinical course and prognosis.
- Early multidisciplinary input, including advance care directive planning and early palliative care input, is the key to effective management.
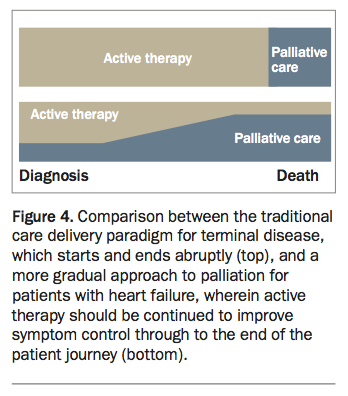
- Many heart failure therapies also have a significant symptom control benefit and should be part of the palliation strategy, rather than being abruptly stopped, as in palliation for other illnesses.
- When further mortality benefits can no longer be achieved, it is crucial to focus on symptom control and avoiding hospitalisation.
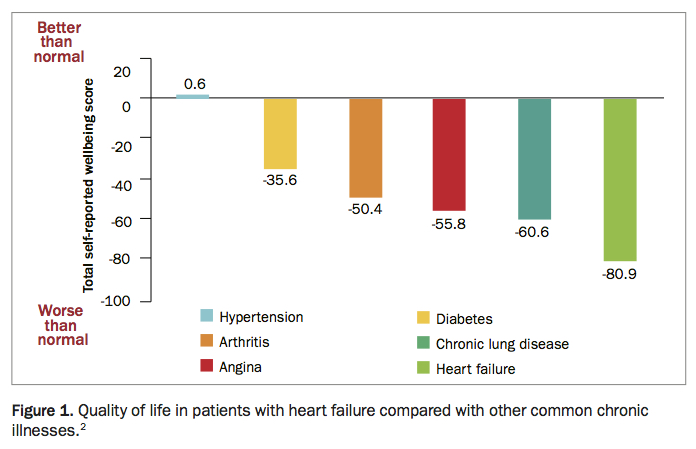
Heart failure (HF) affects an estimated 480,000 Australians, with an additional 40,000 new diagnoses each year.1 In its advanced stages, HF significantly decreases both quality (Figure 1) and length of life.2 There has been an overall reduction in the number of hospitalisations and deaths of patients with HF since the 1990s, but, because of the ageing population of people who are living longer with significant coronary disease, obesity and diabetes, the number of patients who will develop end-stage HF is set to rise.3
{kind=link}
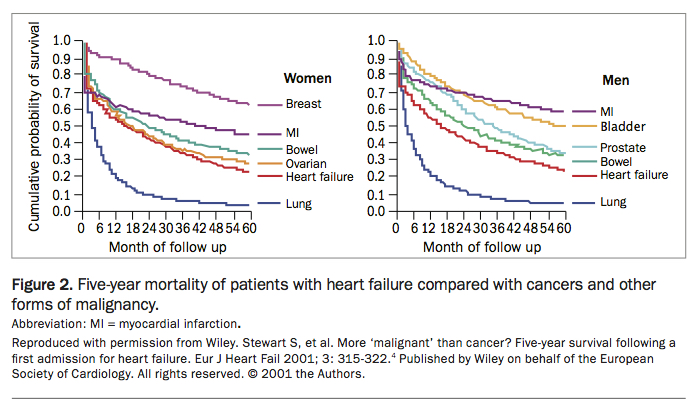
The condition’s terminal trajectory mirrors that of many malignancies. With the exception of advanced lung cancer, HF has worse five-year mortality than many major cancers, including breast, endocrine, bowel and ovarian cancer (Figure 2).4
{kind=link}
The patient journey
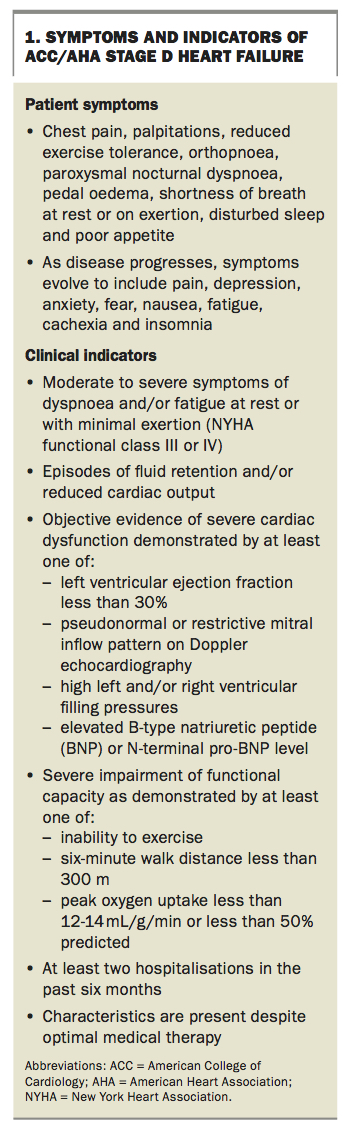
Typically, a patient with end-stage HF presents with severe symptoms of dyspnoea and/or fatigue, even at rest. This is often multifactorial, with contributions from the haemodynamic effects of HF itself and associated comorbid conditions, including chronic obstructive pulmonary disease (COPD), asthma, thoracic kyphosis, basal atelectasis, pneumonia, anaemia or generalised frailty and deconditioning. Patients may describe an inability to perform activities of daily living (including grooming, dressing and showering) and may present with a variety of other symptoms (Box 1). A detailed history is invaluable in monitoring response to therapy.
{kind=link}
Other common associated disorders include valvular heart disease, coronary artery disease, cardiac arrhythmia, arthritis, chronic renal impairment, COPD, anaemia, iron deficiency, malignancy, diabetes, thromboembolism and gout.3
Red flags in patients with end-stage HF include:
- recurrent hospitalisations (i.e. at least two hospitalisations in the past six months), with dyspnoea at rest despite optimal medical therapy
- one or more comorbidities that are hallmarks of a low cardiac output state (conduction disease, polypharmacy, depression, poor renal function, anorexia, constipation, cardiac cachexia, sleep disturbance and refractory hypotension)
- low serum sodium, potassium, magnesium and albumin concentrations, with a high uric acid level, in keeping with decreasing dietary intake and large diuretic doses – these represent powerful markers of poor prognosis.3
Objective evidence of severe cardiac dysfunction is detailed in Box 1. Severe impairment of functional capacity is shown by an inability to exercise (i.e. walking less than 300 metres in a six-minute walk test) or peak oxygen uptake less than 12 to 14 mL/g/min or less than 50% predicted.
Many patients with advanced HF reluctantly spend their final few weeks of life in hospital, at great cost to the health service, with health providers fighting the inexorable disease progression. However, with consideration of the patient’s wishes and forward planning, this scenario can be averted. It is therefore crucial for GPs and all care providers to adopt an early and proactive approach to advance care planning.
Management of end-stage heart failure
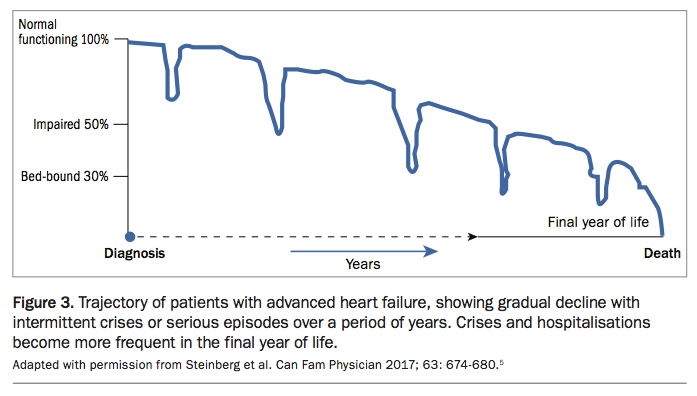
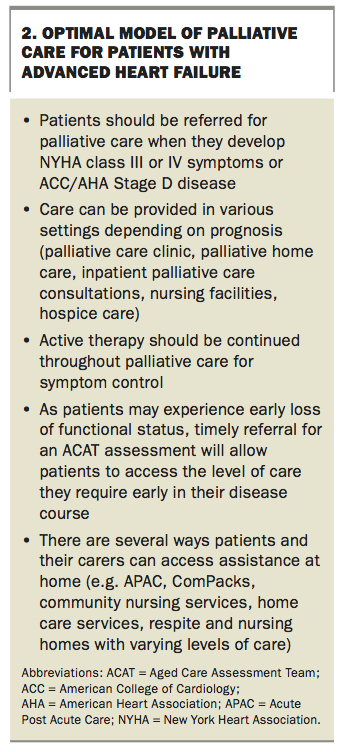
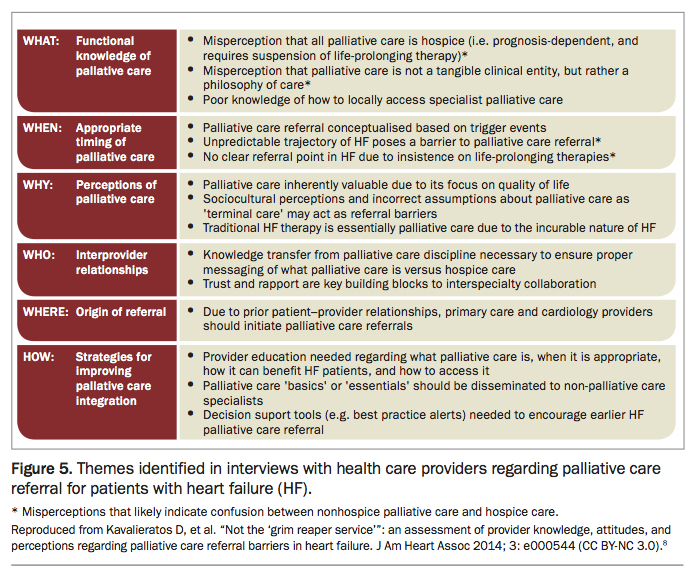
Patients with end-stage HF and their caregivers face unique challenges. The trajectory of patients with advanced HF is unpredictable (Figure 3) compared with other terminal illnesses, such as malignancy, in which patients experience a more linear decline.5 This makes it more difficult to determine a specific point at which a patient should be palliated (Figure 4).6 There are also differences between the traditional model of palliative care, which was developed for oncology patients, and the optimal model of palliative care for patients with advanced HF (Box 2).7 Several barriers to palliative care referral for patients with HF have been shown to be caused by misperceptions of healthcare providers (Figure 5).8 The emphasis should be on having early and proactive discussions about advance care planning and palliative care input before the patient has advanced disease. This conversation is much better handled by a patient’s GP ahead of a critical deterioration during an acute hospital admission.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Unlike patients with malignancy, in whom active therapy (e.g. chemotherapy) is stopped as palliation commences, active therapy (e.g. beta blockade, ACE inhibition, spironolactone) is still recommended towards the end of the patient journey for those with HF, as it improves symptom control.9 If patients are experiencing dyspnoea at rest, consideration may need to be given to further optimisation of medical therapy.
As oral therapies begin to fail, consideration can be given to device therapies (e.g. cardiac resynchronisation therapy [CRT] or biventricular pacing) or valvular interventions (percutaneous or open surgical approaches), or even major cardiac surgery (e.g. ventricular assist devices or cardiac transplantation) if the patient’s condition is amenable. CRT may reduce morbidity and mortality, although the benefit is greatest if administered before the later stages of disease.10-12 CRT is only of benefit in those with significant interventricular conduction delay or bundle branch block. Appropriate physiological reserve (i.e. anaesthetic fitness) must be present to handle the stress of significant valve or major cardiac surgery. Given that the transition point from active to palliative treatment is not well understood, many patients will fail to meet the anaesthetic requirements. These strategies are therefore largely restricted to younger patients with a good chance of significant intermediate to longer term improvement in quality of life or prognosis (e.g. as a bridge to transplant).
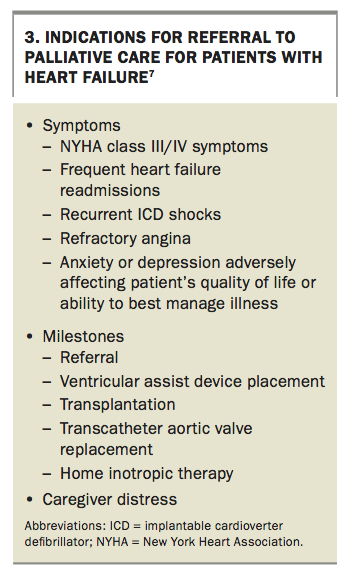
At some stage, the patient and doctors must make a collaborative decision to move the principal aim of care from prognostic improvement to symptom control, in accordance with the patient’s and family’s wishes (Box 3). Knowing when to initiate a discussion about goals of care and advance care directives is difficult and is influenced by many psychological, emotional, social and prognostic factors. It is important to recognise that a broad spectrum of patient perceptions, including religious, spiritual and cultural influences, will exist, and all perspectives should be respected and documented.
{kind=link}
A suggested approach to management
Several approaches to management of end-stage HF have been suggested, which broadly adopt the following steps.3,5,13,14
Set up the team
A collaborative multidisciplinary team-based approach with early palliative input is essential.5,13,15 This will ideally include primary care, cardiology and palliative care services, each represented by various health professionals – doctors, nurses, case managers and allied health staff – who communicate regularly. A primary care service may be best placed to regularly review the patient and co-ordinate advice at this stage, but this may vary depending on the circumstances.
Optimise medical and, if appropriate, device and interventional therapy
Patients should begin treatment with medication that has symptom and mortality benefit, unless contraindicated. They should also be maximally managed for cardiac and noncardiac comorbidities, with defined physiological targets, and referred for device therapy or intervention if appropriate.3,16 Failing all these, and if meeting criteria for end-stage HF, the following steps should be considered.
Daily monitoring, fluid balance and foreseeing trouble
Instructing patients and caregivers on how to monitor weight daily, restricting fluid to 1.2 to 1.5 L/day, how to monitor symptom progression and how to interpret changes will forewarn patients and their treating teams of impending decompensation.3,5 Symptom progression can include worsening dyspnoea and exercise tolerance, pitting oedema, weight gain of 2 to 3 kg over target dry weight, more pillows being required at night and decreasing activity levels.
Adapt ongoing therapy
Although goals of therapy may change, strict control of blood pressure and heart rate (especially in the presence of arrhythmia) is important to control symptoms and prevent decompensation. However, as the disease progresses, patients will eventually show a progression in their symptoms and require uptitration of their medications to manage symptoms. Some patients may become intolerant or unresponsive to certain treatments. A cardiology service may be best placed to co-ordinate care at this stage and negotiate a stepwise approach to common problems (e.g. symptomatic hypotension may require first reducing or ceasing vasodilators, then beta blockers, then ACE inhibitors).3,5,16
Advance care directives and implantable cardioverter defibrillator deactivation
As noted above, it is important that an advance care plan be put in place early, in discussion between the GP, patient and family, before disease progression. When a patient’s quality of life becomes poor and they express a wish to receive no further shocks from their defibrillator, and the family agrees, a group decision may be made to disable the defibrillator shock capacity. This should be assessed on an individual basis and in accordance with the patient’s and family’s wishes.
Helping patients to face the reality of their diagnosis is challenging but will help to crystallise their wishes moving forward. Explaining the realities of escalating hospital-based therapy in unexpected periods of deterioration (i.e. inotropic therapy, intensive care admission, intubation, ventilation and defibrillation) will give patients insight into their journey and provide autonomy for those who wish to exercise more control. If implantable cardioverter defibrillator deactivation is considered, this may require returning to a device specialist.5,13
Exacerbation management plan
Similar to other terminal illnesses, priorities for symptom control include pain, depression, anxiety, fear, nausea, fatigue, cachexia and insomnia. A palliative care service may be best placed to co-ordinate care at this stage; however, other teams will still be involved in holistic patient management (e.g. a cardiology service may provide a diuretic escalation plan, while primary care may manage comorbid diseases and co-ordinate complex care pathways and advice from other specialties, such as endocrinology, renal medicine, respiratory medicine and psychiatry).5,17
Pain is often underrecognised or is not dealt with for fear of destabilising brittle physiology. Hence, it is often undertreated in this patient group. Although some patients may have complex analgesic requirements, simple and appropriate analgesia will benefit many patients.
If the patient and family fully understand the nature of the illness as a terminal condition, fear is a common and logical reaction, and the source of this fear needs to be explored. This can be done by starting with open-ended questions, such as ‘How do you feel about your health?’ or ‘What do you fear most about your condition?’. More pointed questions may also be required, such as ‘Do you fear you will have pain? Or breathlessness? Or loss of independence?’, ‘Do you miss your favourite activity?’, ‘What is the best/worst part of your day?’, ‘In a week, how many good and bad days do you have?’ and ‘Are you afraid of dying?’. The solution has to be tailored to each situation and may be a combination of physical, pharmacological, social and spiritual therapies. Caregivers should screen patients using the validated K10 anxiety and depression questionnaire, and GPs may consider a selective serotonin reuptake inhibitor as first-line therapy. Interactions between antidepressants and cardiac medications do exist (especially with respect to prolonging the QTc interval), but this should not be prohibitive, especially after an advance care directive discussion. Further consideration of pharmacological therapies should be referred to a psychiatrist, and interactions may be discussed with a cardiologist.
Ultimately, all patients should have access to hospital-based management if required. Incorporating the above steps will ease the transition into a supportive care framework, while maximising survival, maintaining quality of life and respecting patient wishes.
Conclusion
End-stage HF is a progressive and life-limiting condition with a prevalence that is likely to rise. Recognising its clinical course, anticipating and planning for common problems and incorporating palliative care services early into a shared, multidisciplinary framework will ensure best care for patients with end-stage HF. MT