Established rheumatoid arthritis – achieving remission

Dr Ng is a Visiting Rheumatologist, Westmead Hospital, Sydney.
Associate Professor Wong is Senior Staff Specialist, Department of Rheumatology, Westmead Hospital, Sydney, NSW; and a Conjoint Associate Professor in the UNSW Rural Clinical School, Coffs Harbour, NSW.
Rheumatoid arthritis
Arthritis

The aim of treating established rheumatoid arthritis is sustained disease remission and prevention of joint destruction. In addition to modifying lifestyle factors such as diet and exercise, remission is usually achievable with combination therapy using conventional synthetic disease-modifying antirheumatic drugs (DMARDs) and biologic DMARDs or newer, oral, targeted synthetic DMARDs.
- The aim of treating established rheumatoid arthritis (RA) is sustained clinical remission (absence of clinically inflamed joints and normal inflammatory markers) and prevention of joint destruction.
- Clinicians should be aware of how to manage disease and treatment-related complications.
- Lifestyle factors such as diet and exercise should be addressed to improve symptoms, maximise physical function, enhance treatment response and reduce cardiovascular risk.
- Disease remission is usually achievable with combination therapy using disease-modifying antirheumatic drugs (DMARDs) – conventional synthetic DMARDs and biologic DMARDs or newer, oral, targeted synthetic DMARDs.
- Clinicians should be aware of the increased risk of infection with DMARDs and implement measures such as early treatment of infection and timely vaccination.
- Patients with established RA also experience noninflammatory pain, including mechanical, neuropathic and fibromyalgia-related pain.
- Mental health issues such as depression are more common among patients with chronic disease and should be considered an important part of overall management.
Rheumatoid arthritis (RA) is a chronic systemic inflammatory condition that affects 1.9% of Australians, predominantly middle-aged females.1 It is associated with pain, physical disability, fatigue and sleep disturbance. Prolonged active disease leads to progressive irreversible joint damage, functional deterioration and increased mortality from accelerated cardiovascular (CV) disease.2
Although the exact cause of RA is unknown, understanding the molecular pathogenesis has allowed development of targeted treatment using biologic disease-modifying antirheumatic drugs (bDMARDs) such as etanercept and adalimumab and targeted synthetic DMARDs (tsDMARDs) such as tofacitinib and baricitinib. This has revolutionised the management of RA and resulted in disease remission (no clinically inflamed joints and normal systemic inflammatory markers) being achievable in many patients using early intensive therapy. Although this has resulted in significantly less morbidity, the likelihood of disease remission is lower in patients with established disease compared with those with early disease.3,4 It is therefore crucial to start conventional synthetic DMARD (csDMARD) therapy as early as possible and escalate to b/tsDMARDs, if appropriate (Case vignette: Part 1).
{kind=link}
Lifestyle changes
Diet
There is growing evidence that patients with inflammatory arthritis display gut dysbiosis with imbalance of microorganisms compared with healthy controls, suggestive of a link between immune responses, nutrition and gut microbiota.5 A diet high in fish oil along with csDMARD therapy was effective in settling joint inflammation.6 A handful of prospective studies have identified beneficial effects of the Mediterranean diet in reducing pain and increasing physical function in people living with RA.7 Although there is currently insufficient evidence to support widespread recommendation of the Mediterranean diet for prevention of RA, there is general consensus that a diet low in salt but high in vegetables and fish and less red meat is beneficial.8
Smoking
Smoking has been linked to an increased risk of seropositive RA.9 Patients with RA who are current smokers are less likely to respond to csDMARD or bDMARD therapy.10 Besides, smoking cessation is also important for CV risk modification. Therefore, all patients with RA should be actively advised on smoking cessation.
Exercise
RA is associated with accelerated muscle wasting and reduction in strength. Structured exercise incorporating aerobic and resistance training has CV benefit and improves fatigue in patients with RA (Figure 1).11,12 Resistance exercise also improves muscle mass and physical function in patients with RA.13 Fear of aggravating disease or causing joint damage is a barrier to exercise in patients with RA.14 Promoting physical activity using motivational interviewing techniques and addressing barriers to exercise has beneficial effects on weight, wellbeing, mobility and mood.15
{kind=link}
Secondary complications in established rheumatoid arthritis
Cardiovascular risk
Prolonged active inflammatory arthritis is associated with higher CV risk, which could result in myocardial infarction, stroke and death.2 Clinicians should regularly address CV risk factors by providing dietary advice, encouraging regular exercise and smoking cessation, optimising lipid profile, ensuring tight blood pressure control and minimising corticosteroids and NSAIDs.8 This is a particularly important role for GPs involved in the care of patients with RA.
Osteoporosis
Postmenopausal status, active RA, glucocorticoid use and physical inactivity increase the risk of osteoporotic fracture.16 Bone mineral density (BMD) assessment by dual-energy x-ray absorptiometry (DXA) is helpful for fracture risk stratification and monitoring treatment. In Australia, bisphosphonate therapy (e.g. risedronate 35 mg or alendronate 70 mg once weekly) is reimbursed under the PBS for primary prevention of osteoporosis (in patients 70 years of age or older with a BMD T-score of 2.5 or less), prevention of glucocorticoid-induced osteoporosis and secondary prevention of osteoporosis following low trauma fracture. Denosumab therapy is reimbursed under the PBS for primary prevention of osteoporosis (in patients 70 years of age or older with a BMD T-score of 2.5 or less) and secondary prevention of osteoporosis following low trauma fracture. Vitamin D replacement should be advised, aiming for a serum 25-hydroxyvitamin D level of more than 50 nmol/L, as well as adequate calcium intake, preferably by dietary means (Figure 2) (Case vignette: Part 2).
{kind=link}
{kind=link}
Conventional synthetic disease-modifying antirheumatic drugs
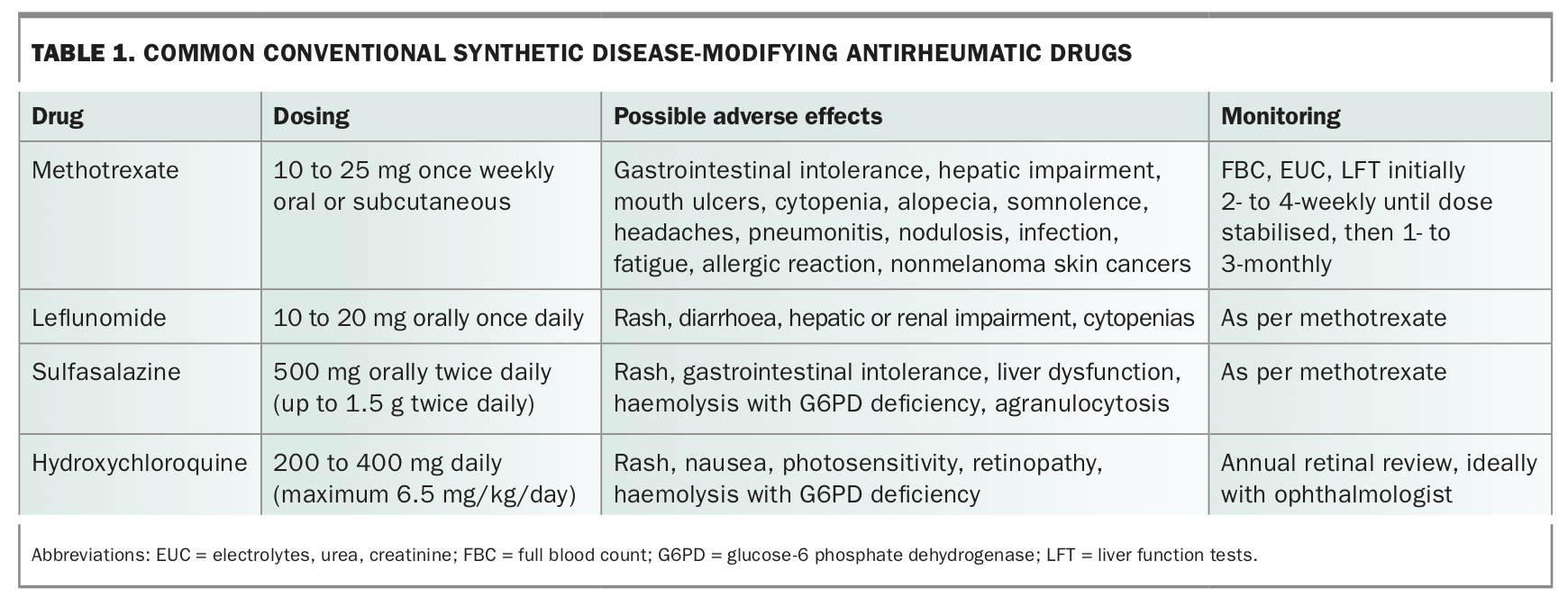
Methotrexate remains the cornerstone of RA management, as it is usually well tolerated and effective at preventing radiographic progression (erosions and joint damage). It is usually used as the first-line csDMARD and even continued in combination with bDMARDs to prevent formation of neutralising antidrug antibodies to the bDMARD. Parenteral methotrexate can be used if the oral preparation is not tolerated or is ineffective. However, other csDMARDS are available (Table 1). Folic acid reduces methotrexate side effects, especially oral ulceration. Although there are many folic acid supplementation regimens in use, there is no strong evidence to favour one over the other. The important message is to take some, rather than none. Although patients and other health professionals may have concerns regarding methotrexate side effects, it is a safe and effective first-line csDMARD if prescribed and monitored appropriately.
{kind=link}
Standard therapy is to add other csDMARDS to methotrexate, if monotherapy does not result in RA remission (absence of swollen and tender joints with normal inflammatory markers). Subject to patient comorbidities, disease remission is the goal for many patients.
Drug adherence
Adherence to csDMARDs and bDMARDs is variable in patients with RA.17 Factors associated with nonadherence include fear of side effects and pre-existing beliefs from information available in the general media.18 Patient education is important in addressing poor medication adherence through identifying concerns and fostering shared decision-making. This can be an important role of the treating GP.
Management of flares
Systemic corticosteroids (e.g. oral prednisone less than 15 mg daily, rather than 50 mg daily) or intra-articular steroid injections are often used to manage disease flares. However, given the range of csDMARDS and b/tsDMARDS available, long-term corticosteroid use is not recommended due to the significant risk of complications (Box).
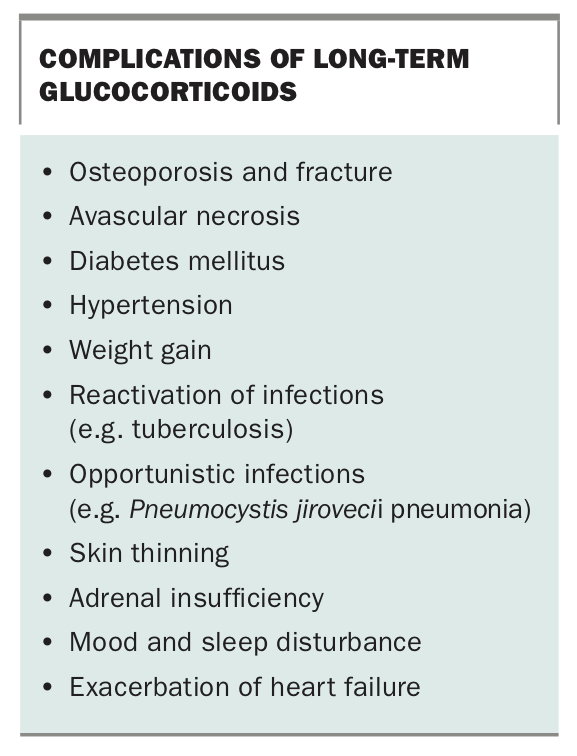{kind=link}
Escalation to bDMARD or tsDMARD therapy should occur when disease remission is not achieved with combination csDMARDs or intolerance to multiple csDMARDs. Although a GP can prescribe csDMARDs, bDMARDs and tsDMARDs require authority prescription by a rheumatologist. Due to the high cost of b/tsDMARDs, the PBS in Australia mandates the presence of active RA (activity in four large joints or 20 small joints despite more than three months of combination csDMARD therapy) before a b/tsDMARD is subsidised.
Pretreatment screening
Screening for chronic infections, such as hepatitis B (including the Hep B cAb test), hepatitis C, HIV and tuberculosis (Quantiferon Gold blood test and chest x-ray) is important to guide the need for antimicrobial therapy before starting b/tsDMARDs (Case vignette: Part 3).
{kind=link}
Choice of biologic or targeted synthetic disease-modifying antirheumatic drug therapy
The increasing number of b/tsDMARDS available makes it difficult to decide which agent to use (Table 2). Despite much research, it is impossible to know which patient will respond best to a particular b/tsDMARD. As most b/tsDMARDS have similar efficacy because they act on a common pathway, namely, the proinflammatory cascade, drug choice is usually determined by physician familiarity with the drug, national regulatory prescribing guidelines, side effect profile and route/frequency of administration. Recently, biosimilars (e.g. for etanercept and infliximab) have entered the market. These medications are similar but not identical to the originator bDMARD and have demonstrated bioequivalence to obtain regulatory approval. Due to their cheaper cost, it is hoped they will reduce the overall financial burden to the PBS and improve patient access to bDMARDs. However, there is limited data on the effect of interchanging these with the originator bDMARD.
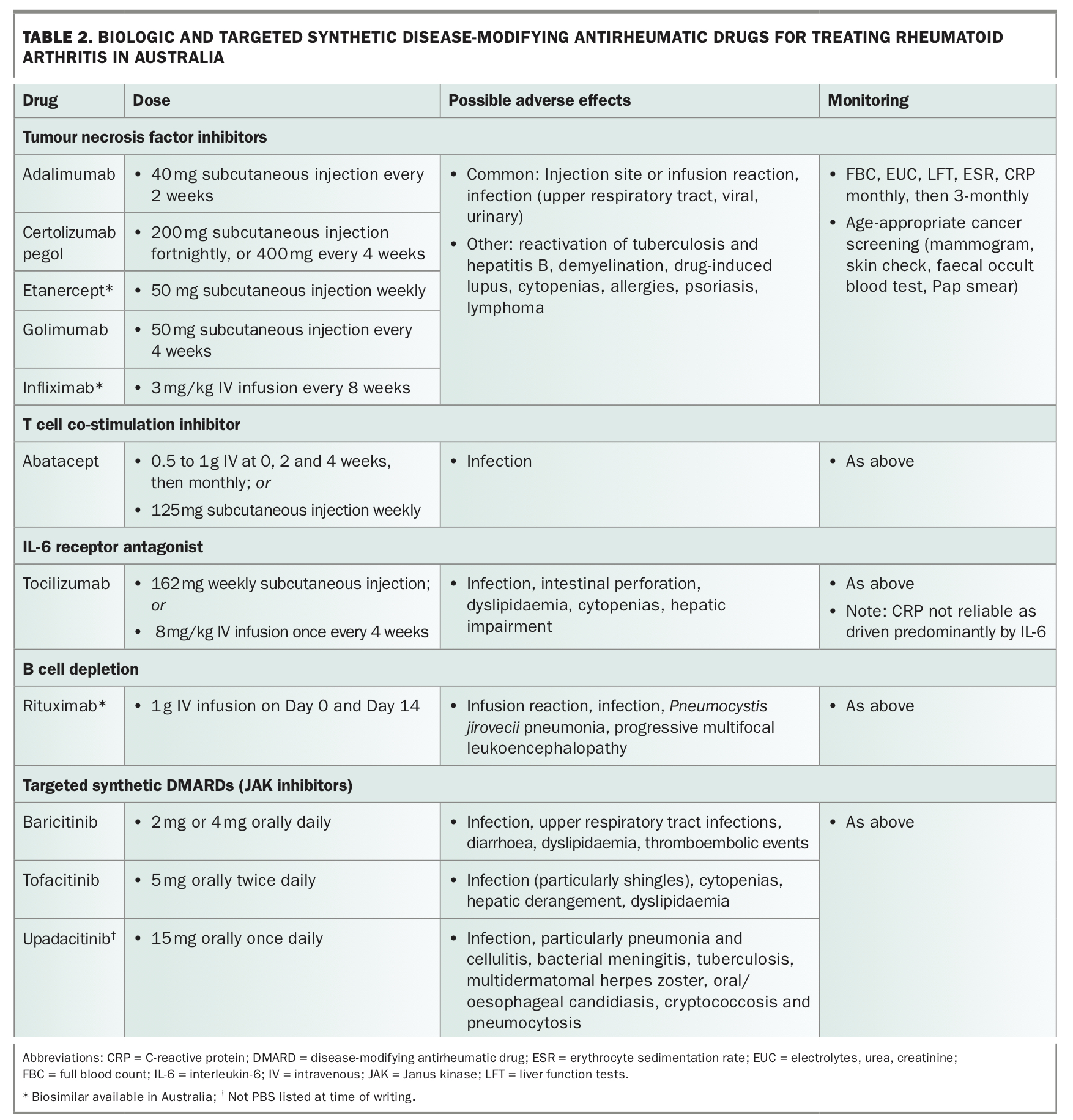{kind=link}
As tumour necrosis factor (TNF) inhibitors were the first class of targeted therapy available, most rheumatologists use these as first-line bDMARDS. Within this drug class, the convenient four-weekly administration of golimumab may improve drug adherence and is often preferred by patients who dislike injections. The weekly dose frequency of etanercept is useful in those at high risk of infection as cessation allows prompt drug clearance. Etanercept is also associated with a lower risk of mycobacterial infection. The fortnightly administration of adalimumab and certolizumab provides a compromise between the dosing frequency of golimumab and etanercept. Certolizumab has the added advantage of not crossing the placenta and hence, can be considered in young females of childbearing age and during pregnancy. Generally, TNF inhibitors are co-administered with methotrexate for better efficacy and to lower the risk of neutralising antidrug antibodies. As there is probably an increased risk of nonmelanoma skin cancers (NMSC) with csDMARDs and TNF inhibitors, regular (six to 12-monthly) skin checks are important and usually performed by the GP.19
It is reasonable to use tocilizumab (an IL-6 receptor inhibitor) as a first-line bDMARD, particularly in the setting of methotrexate intolerance. Tocilizumab appears superior to adalimumab as monotherapy. However, tocilizumab is best avoided in someone with previous diverticulitis due to the risk of intestinal perforation.20 The lack of association with NMSC means tocilizumab is preferable to a TNF inhibitor in patients with a history of skin cancer.
Abatacept (a T cell co-stimulation blocking agent) appears to have a lower risk of infection than a TNF inhibitor.21 It may be the bDMARD of choice in those at high risk of infection. The weekly administration also allows rapid drug clearance if infection occurs.
In Australia, rituximab (a B cell depleting antibody) is only subsidised by the PBS for use following TNF inhibitor failure. The two infusions at weeks 0 and 2, given every six months, are convenient. However, the long duration of B cell depletion (six to 12 months) means vaccination should occur before the first infusion. Its established use in lymphoma treatment means most rheumatologists are comfortable using rituximab in patients with previous malignancy.
The recent availability of the Janus kinase inhibitors tofacitinib and baricitinib as the first oral small molecule inhibitors is a major advancement. These agents are particularly useful for patients who struggle with injections. The increased risk of shingles, especially in Asians, means administration of the live shingles vaccine should be considered before starting tofacitinib.22
Complications of treatment with biologic or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs)
Reactivation of latent infection
Reactivation of latent tuberculosis infection (LTBI) is usually associated with TNF inhibitors. This is now uncommon due to widespread pre-treatment screening. Among the TNF inhibitors, etanercept has the lowest risk of LTBI reactivation. If detected (e.g. by a positive Quantiferon Gold test), isoniazid treatment should be given for at least one month before starting the b/tsDMARD and continued for up to nine months. Abatacept, tocilizumab, rituximab and tofacitinib all have lower rates of LTBI reactivation compared with the TNF inhibitors.23
Treatment of infection
As b/tsDMARDS are immunosuppressive, infections should be treated early. Severe or persistent infections should prompt cessation of the csDMARD or b/tsDMARD until resolution of the infection. Advice from the treating rheumatologist may be required.
Prevention of infection with vaccination
Live vaccines (e.g. for shingles, measles, mumps and rubella, and yellow fever) are contraindicated with b/tsDMARD use. Influenza vaccination should be administered annually and pneumococcal vaccination should be current. Ideally, vaccination should be administered before immunosuppression but, in practice, this is usually logistically difficult. Vaccination of the immunosuppressed rheumatology patient is a complex area and has been recently reviewed.24,25 It requires close collaboration between the GP, rheumatologist and, if required, an infectious diseases physician.
Malignancy
There is no convincing evidence that b/tsDMARDs result in an increased risk of primary or secondary malignancy, except for NMSC with TNF inhibitors.19 However, regular skin checks should be undertaken in those taking a b/tsDMARD and age-appropriate cancer screening performed as per national guidelines. This is best done by the GP.
Comorbid depression and chronic pain
Depression is very common among people with chronic diseases such as RA. Routine mood screening in patients with established RA is important to facilitate early intervention. Depression can be associated with poor medication adherence and pain sensitisation.26 This is an important issue for the GP to address (Case vignette Part 4).
{kind=link}
Conclusion
The management of established RA requires close collaboration between the GP, rheumatologist and other healthcare professionals; for example, the physiotherapist or psychologist. Disease remission is a realistic goal in many patients, especially if treatment is started early. The GP has a particularly important role in monitoring blood tests, pre-immunosuppression vaccinations and early treatment of infections. Addressing lifestyle factors such as diet, smoking cessation and exercise can help improve patient wellbeing and CV risk profile, and maximise treatment response in this population. Depression is common in patients with chronic RA and often requires treatment to improve function and quality of life. MT