Janus kinase inhibitors in inflammatory arthritis: what the GP needs to know

Drugs that inhibit the intracellular janus kinase (JAK) enzyme systems are the latest addition to the armamentarium of disease-modifying antirheumatic drugs (DMARDs). Members of this class have been approved for use and are cost-subsidised in Australia for selected patients with rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis.
Drug treatment is the most effective way to manage inflammatory arthritis. A range of medications have been shown to modify the natural history of inflammatory rheumatic diseases such as rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis. These medications are termed disease-modifying antirheumatic drugs (DMARDs). DMARDs not only reduce symptoms of inflammation, such as pain, swelling, stiffness, fatigue and poor overall health, but also decrease structural joint and other musculoskeletal damage. In addition, they modify the long-term consequences of systemic inflammation, including osteoporosis and cardiovascular disease.
Drugs that inhibit the intracellular janus kinase (JAK) enzyme systems are the latest addition to the DMARDs. JAK inhibitors, also known as jakinibs, are effective in reducing local and systemic inflammation and its consequences in a range of inflammatory arthritides. Members of this class have been approved for use and are cost-subsidised in Australia for selected patients with rheumatoid arthritis (tofacitinib, baricitinib and upadacitinib) or psoriatic arthritis (tofacitinib). Upadacitinib has also been approved for patients with psoriatic arthritis or ankylosing spondylitis.
This review describes the place in therapy of the JAK inhibitors for patients with inflammatory arthritides such as rheumatoid and psoriatic arthritis and ankylosing spondylitis, as well as important clinical issues related to their use, particularly for GPs.
DMARD nomenclature
The most commonly used DMARDs are termed conventional synthetic DMARDs (csDMARDs) because they are synthesised in a standard drug manufacturing process. They include hydroxychloroquine, sulfasalazine, methotrexate and leflunomide.
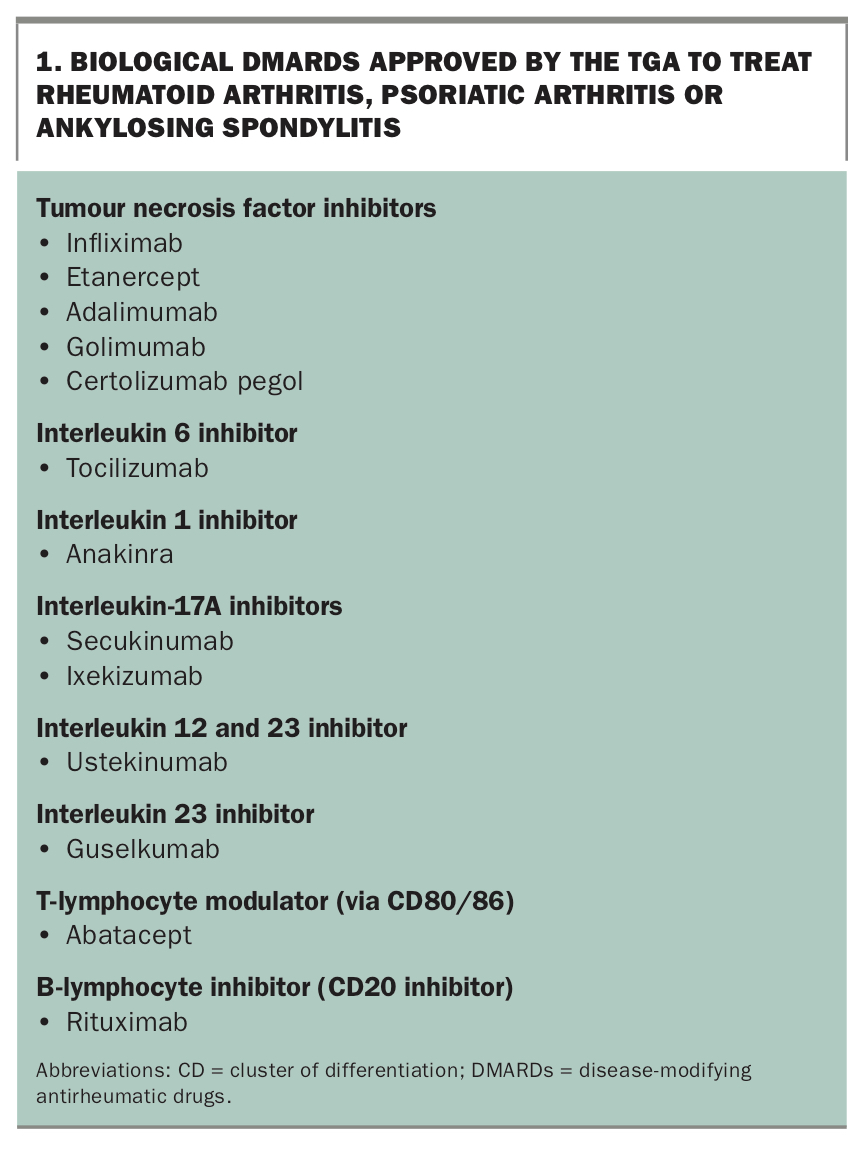
DMARDs manufactured in more complex biological systems are termed biological DMARDs (bDMARDs). Drugs in this class target specific immune-related cytokines or other immune processes involved in joint or related inflammation (Box 1).
{kind=link}
Drugs that inhibit JAK-related enzymes are synthesised by conventional manufacturing (nonbiological) processes but target specific enzymes involved in inflammatory joint disease, distinct from the broader immune-modulating effects of the csDMARDs. This drug class is thus known as targeted synthetic DMARDs (tsDMARDs), also termed jakinibs.
What is janus kinase?
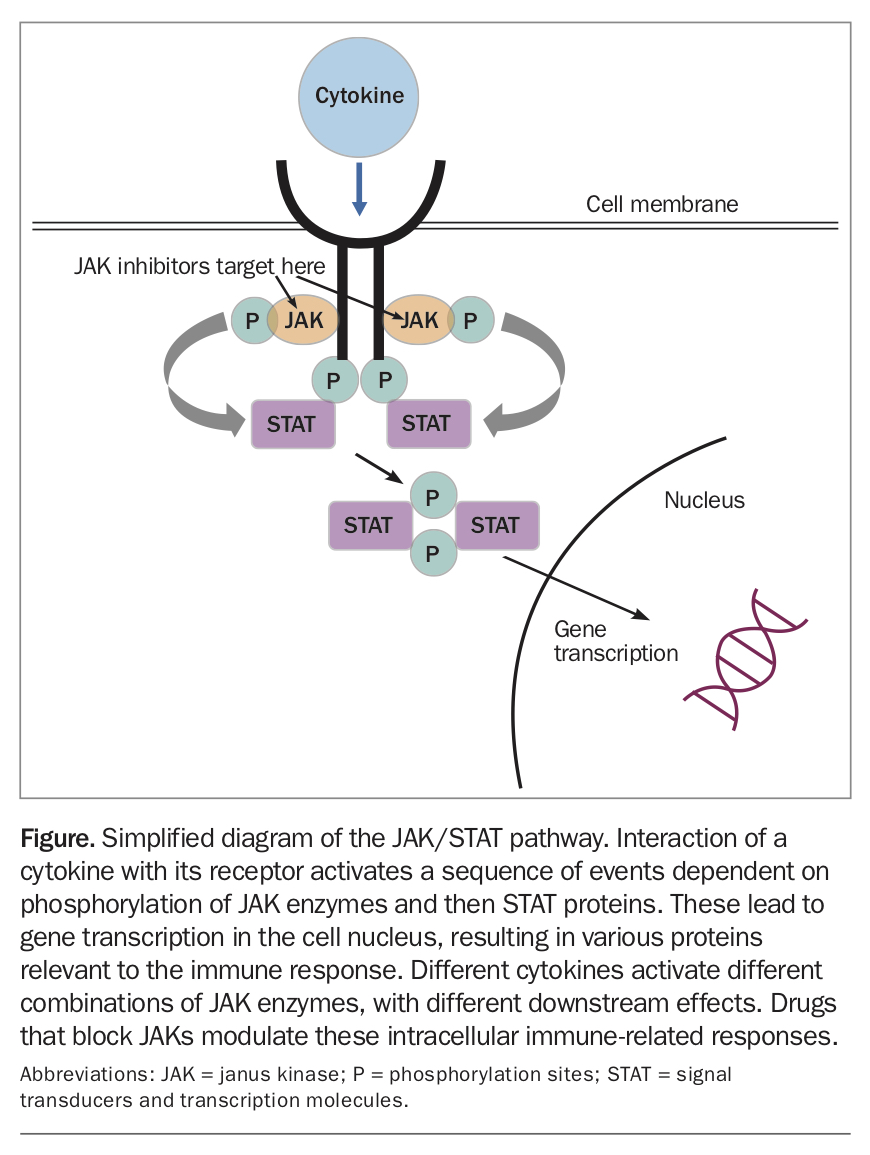
The janus kinase (JAK) enzyme system takes its name from Janus, the Greek god of doorways, who looks both into and out from a room. The JAK enzyme systems facilitate signals, such as those caused by inflammatory cytokines, that interact with the cell surface to initiate intracellular responses, including activation of signal transducers and transcription molecules (STATs) that subsequently allow regulation of gene expression in the cell nucleus.1 Thus, the JAK/STAT system is a direct mechanism for translation of extracellular inflammatory signals to transcriptional responses by the cell.
In mammals, the JAK/STAT signalling mechanism is the principal pathway for a wide assortment of cytokines and growth factors to incite cell division, differentiation, migration and programmed death, all events crucial in immune activation. Inhibiting this pathway can control unwanted or overactive immune responses, such as those that occur in inflammatory rheumatic diseases (Figure).
{kind=link}
The JAK family comprises four members: JAK1, JAK2, JAK3 and tyrosine kinase 2 (TYK2). The various combinations of these respond to different cytokines, in turn resulting in different downstream intracellular responses. For example, the cytokines active in rheumatoid arthritis interact with different JAKs from those that accompany viral infection, with different cellular responses.
The JAK inhibitor drugs differ in their reversible dose-dependent enzyme selectivities and thus may have different effects on cytokine blockade, growth factors and other JAK/STAT-dependent cell functions.
Drug management algorithm in inflammatory joint disease
PBS cost subsidisation of bDMARD and tsDMARD therapy depends on the patient fulfilling a specific therapeutic treatment algorithm. This generally requires significant ongoing clinically defined inflammatory joint or spinal disease (self-reported by the patient) despite an adequate trial of other standard therapies that include csDMARDs for rheumatoid arthritis and psoriatic arthritis, and NSAIDs for ankylosing spondylitis. PBS subsidy for prescription of these drugs is available only to rheumatologists or clinical immunologists. Although these drugs are expensive, the clinical benefits are considerable, and they are consequently cost effective.
A wide choice of bDMARDs and tsDMARDs is available to the prescribing clinician for patients with rheumatoid arthritis, psoriatic arthritis or ankylosing spondylitis. Drug selection is complex and depends on several factors, including disease activity, previous response or side effect from a bDMARD or tsDMARD, contraindications, comorbidities, age, pregnancy planning, medication adherence, route of delivery, patient preference and clinician experience and judgement.2,3
Management of a patient taking one of these drugs is also complex and requires ongoing interaction between the patient, specialist and GP.
Clinically available jakinibs
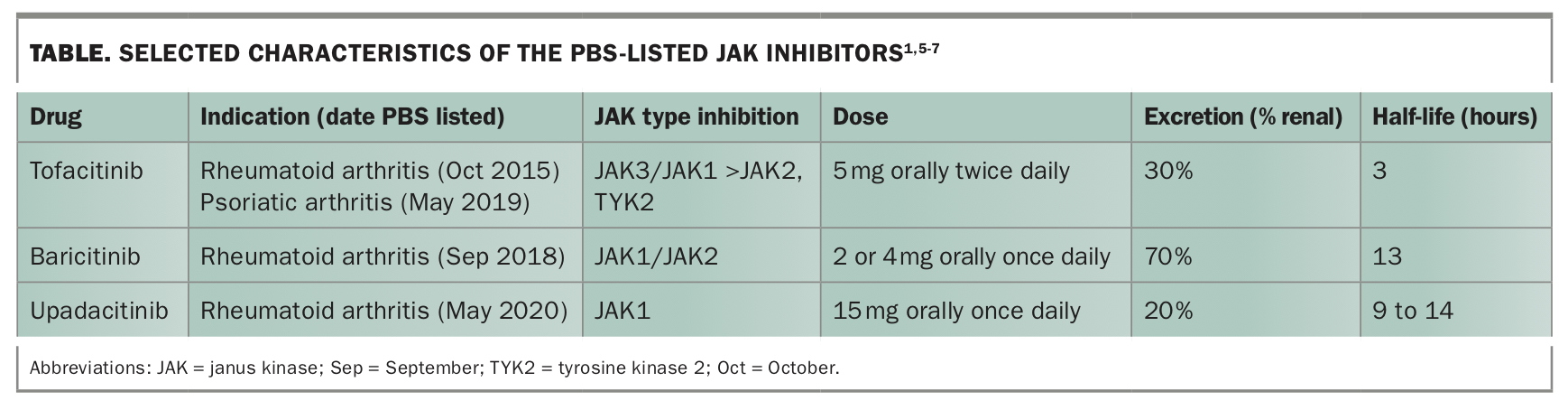
The jakinibs are increasingly used as first- or second-line DMARDs by rheumatologists in Australia.4 Three jakinibs are currently approved for rheumatological indications in Australia: tofacitinib, baricitinib and upadacitinib.5-7 Others are in the process of evaluation.
Selected characteristics of tofacitinib, baricitinib and upadacitinib are presented in the Table.1,5-7 These medications have the advantage of oral administration, and are taken once or twice daily, depending on the drug. The short half-life of the jakinibs enhances management of any adverse events compared with bDMARDs. Detailed differences between the individual jakinibs will not be discussed in this article.
{kind=link}
Efficacy of jakinibs
All of the above jakinibs have been extensively evaluated in standard clinical trial templates, with clinical outcomes similar between drugs.8 There have been no head-to-head studies directly comparing jakinibs. The drugs have been shown to be superior to placebo and methotrexate and on average to have at least similar and often greater efficacy compared with bDMARDs, such as adalimumab and abatacept.8,9
Onset of benefit is usually relatively quick, with lessening of fatigue, stiffness, joint pain and swelling usually being evident within two to four weeks. Studies show better drug persistence of jakinibs over time compared with bDMARDs, implying greater effectiveness. However, rates of discontinuation because of intolerance appear higher.10
Adverse effects and other considerations
Gastrointestinal effects
There is a small increase in nausea, vomiting or diarrhoea with jakinib therapy compared with placebo. Dose adjustment may be needed to manage these effects.
Blood tests
Jakinib therapy may lead to a decrease in white cell count or haemoglobin concentration, or an increase in platelet count, all of which usually return to normal with dose cessation or adjustment. Liver function test results or creatine kinase levels may increase, usually only mildly. As with other drugs that effectively suppress inflammation, there may be a rise in LDL cholesterol level, which may require intervention depending on the overall lipid profile. Because of these possibilities, regular blood test monitoring is necessary. The recommended frequency ranges from monthly to six-monthly, depending on other medications and comorbidities, such as renal dysfunction.
Infections and vaccination
Acute infections
Like other DMARDs, jakinibs are associated with an increased rate of infections. These are mainly upper respiratory viral infections but can also include bacterial infections, such as urinary tract infections. Rates of severe infection are about 2.7 per 100 patient-years, a similar rate to that seen with bDMARDs.
Tuberculosis
Reactivation of tuberculosis is rarely seen with jakinibs, in contrast to tumour necrosis factor (TNF) inhibitors. However, it is usual to screen for latent tuberculosis with an interferon gamma release assay and to assess other risk factors. Any possible subsequent treatment (e.g. with TNF inhibitors) is dependent on this assessment.
Herpes zoster
As a drug class, the jakinibs are associated with an increased rate of herpes zoster compared with placebo, csDMARDs and bDMARDs.11 The number of events is in the range of 2 to 3 per 100 patient-years of treatment with jakinibs, compared with 1 to 2 per 100 patient-years for bDMARDs. The rate is higher in some population groups, such as Koreans and Japanese. It is also influenced by coprescription of csDMARDs and particularly glucocorticoids.
Rates of herpes zoster vary between the individual jakinibs. Selectivity for JAK1 may be associated with a lower risk of herpes zoster. If herpes zoster occurs, it is usually mild and limited to a single dermatome.
Shingles vaccination before commencement of a jakinib should be considered, bearing in mind that the shingles vaccine Zostavax is a live attenuated vaccine, and that the patient may already have immunosuppression caused by other currently used DMARDs. Most csDMARDs and low-dose prednisolone are not themselves contraindications for vaccination, but bDMARDs and tsDMARDs need to be stopped for several weeks before vaccination with Zostavax. The availability of the non-live shingles vaccine Shingrix will simplify vaccination in this setting, but flares of rheumatoid arthritis have been seen in a small proportion of patients after vaccination with Shingrix. Discussion between the rheumatologist and the GP is advised if vaccination is considered.
Patients who present with clinical features suggestive of herpes zoster need prompt assessment and rapid implementation of antiviral therapy.
Hepatitis
Infection with hepatitis B or C virus needs to be assessed and treated but is not necessarily a contraindication to jakinib therapy.
Vaccination
The use of live vaccines is contraindicated with jakinib therapy. Otherwise, standard approaches to vaccination apply.12
Venous thromboembolism
Patients with rheumatoid arthritis have a 50% increased risk of venous thromboembolism (VTE) compared with people without rheumatoid arthritis, although the baseline absolute risk is low. There is a slight increase in thromboembolic events in rheumatoid arthritis patients taking jakinibs, with the VTE rate increasing from the background rate of 5 to 6 cases per 1000 by an extra 1 to 2 cases per 1000. Patients need to be assessed for VTE risk before considering starting a jakinib. Patients taking a jakinib who develop any clinical features of VTE need to be quickly assessed and managed.
Malignancy
At this time, there are no data to suggest any increase in malignancy in patients taking jakinibs. Patients with previous malignancy need individual consideration before commencing a jakinib, but there appear to be no unique issues with this class of DMARD compared with others. In general, one would expect patients with a malignancy to have it fully treated, to be in remission and to obtain clearance from the oncologist before starting a jakinib.
Drug interactions
Jakinibs can be combined with csDMARDS, glucocorticoids (prednisolone or cortisone joint injection), or anti-inflammatory medication as indicated. No relevant clinical interactions with commonly prescribed drugs have been noted.
Renal considerations
Tofacitinib and baricitinib may need dose modification in patients with moderate renal impairment.
Stopping jakinibs
As jakinibs have very short half-lives, discontinuation results in drug elimination in several days. Short-term discontinuation is considered, for instance, when there is severe infection, including herpes zoster.
Surgery
There is little information on whether jakinibs increase the risk of perioperative infection or delay wound healing. Based on extensive experience with bDMARDs, these problems are not expected. Nevertheless, some surgeons and rheumatologists may adjust jakinib therapy in patients undergoing surgery, discontinuing the drug from a few days before surgery until wound healing has commenced a week after surgery.
Use in pregnancy
There is little information about the safety of jakinibs during pregnancy. The general advice is to avoid these medications in this setting.
Shared care considerations
The cost and complexity of drug management in patients with rheumatoid arthritis and other inflammatory rheumatic diseases has resulted in the restriction of csDMARD, bDMARD and tsDMARD prescribing to rheumatologists and clinical immunologists. However, to ensure the best outcomes for patients, GPs have a key role in their management. Crucial shared-care responsibilities include smoking cessation, weight control, promotion of exercise, mental health and bone health, lipid and cardiovascular risk management, and surveillance and treatment of herpes zoster and other infections.
Conclusion
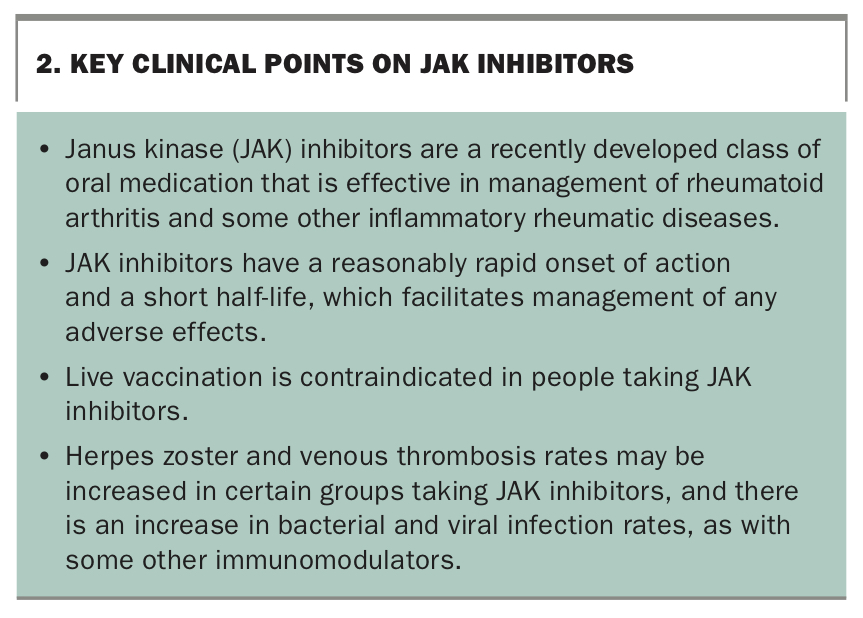
The jakinibs are a recent addition to the armamentarium used to control inflammatory rheumatic diseases. Key clinical points on the jakinibs are summarised in Box 2. Further clinical experience will clarify their efficacy, side-effect profiles, durability of effect and overall place in the management of these important high-impact diseases. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.