Resistant hypertension – updates, issues and approach to management

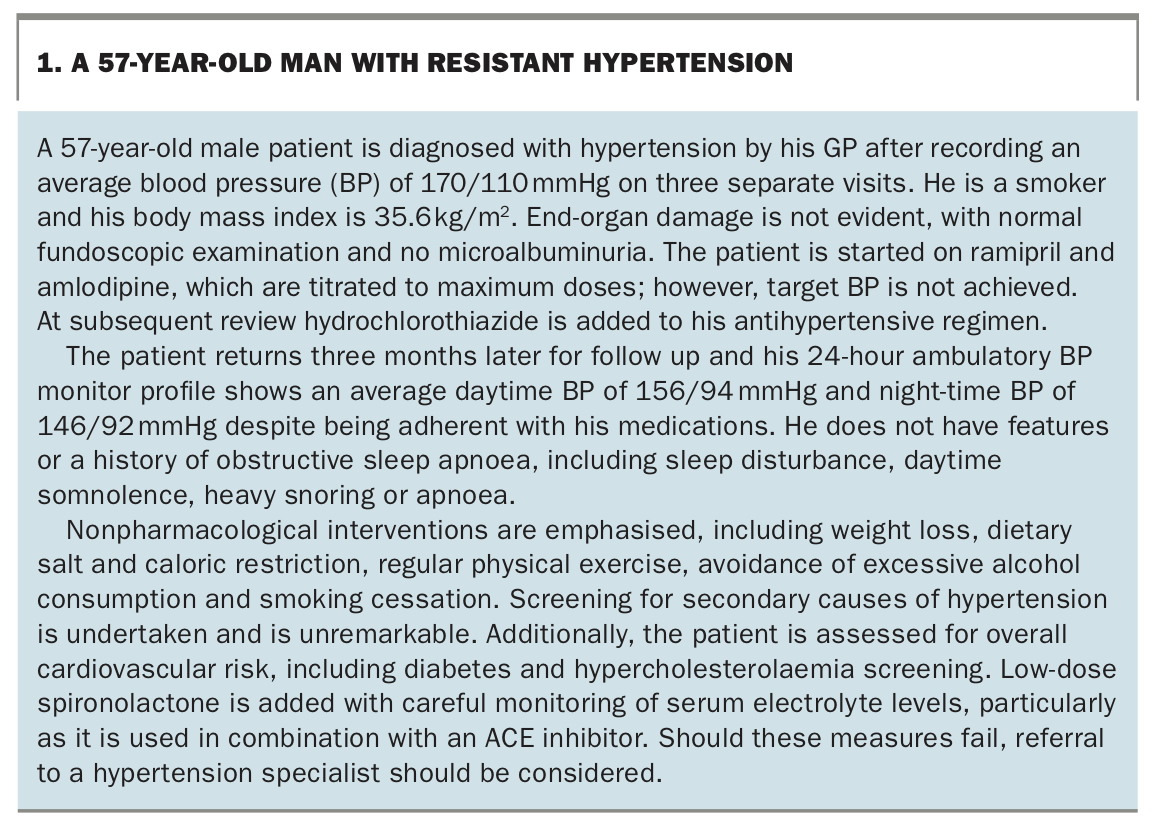
Successful management of poorly controlled hypertension requires careful distinction of true resistant hypertension from other causes such as poor adherence to hypertension medications, undiagnosed secondary hypertension and white-coat hypertension. An individualised approach that includes modifying lifestyle and diet and optimising pharmacotherapies is recommended for patients with suspected resistant hypertension.
- Resistant hypertension is present when blood pressure remains elevated despite adherence to three or more antihypertensive medications at optimally tolerated doses (including a diuretic) and lifestyle modification.
- White-coat hypertension and causes of secondary hypertension such as obstructive sleep apnoea and chronic kidney disease need to be excluded.
- Both 24-hour ambulatory and home blood pressure self-monitoring are important diagnostic and management tools in suspected resistant hypertension.
- Treatment of resistant hypertension comprises optimising lifestyle modifications such as lowering salt intake, weight loss and exercise, and using more aggressive pharmacotherapy with combinations of medications from different classes that also specifically include a diuretic. Specialist consultation may be required.
- Techniques to improve patient engagement such as app-based technologies and home blood pressure self-monitoring may improve adherence to medication and lifestyle modifications.
Hypertension is the strongest contributor to the burden of disease worldwide according to the World Health Organization and, as such, is a leading cause of preventable and premature death.1 Hypertension is highly prevalent in Australia, where at least 34% of adults are known to be hypertensive, and is associated with reduced productivity and poorer quality of life.2-4 Globally, rates of hypertension are rising due to ageing populations and lifestyle risk factors including poor diet, obesity and physical inactivity.5 Despite the compelling benefits of reduced morbidity and mortality by treating hypertension, up to 23% of Australian adults have uncontrolled hypertension with blood pressure above currently recommended targets.4
People with hypertension that appears resistant to therapy are increasingly encountered in primary care. GPs play a crucial role in both delineating true resistant hypertension from other causes of poorly controlled hypertension and in improving blood pressure (BP) control in this important group with high cardiovascular risk. This article discusses an exemplary case (Box 1), summarises clinical issues and provides an approach to diagnosis and management of resistant hypertension.
{kind=link}
Risk factors for resistant hypertension
Uncontrolled hypertension may have patient, clinician and environmental factors contributing. Patient factors cross biopsychosocial domains and include lifestyle factors (high salt diet, alcohol consumption, physical inactivity, obesity, smoking), poor medication adherence and secondary causes of hypertension. Clinician factors such as therapeutic inertia are also important and have been implicated in high rates of uncontrolled hypertension, both locally and internationally.6,7
Resistant hypertension is distinct from uncontrolled hypertension and is defined by the International Society of Hypertension as an office BP above 140/90 mmHg in patients treated with three or more antihypertensive agents at maximally tolerated doses and including a diuretic.
The strongest risk factors for resistant hypertension are obesity and older age.8 Obesity is associated with sympathetic overactivity, sustained activation of the renin-angiotensin-aldosterone system and an increase in cardiac output and vascular stiffness, which all contribute to the development of resistant hypertension.9 Older individuals are more likely to have heavily calcified or atherosclerotic arteries, contributing to this phenotype of resistant hypertension.
Secondary causes and pseudoresistance require exclusion
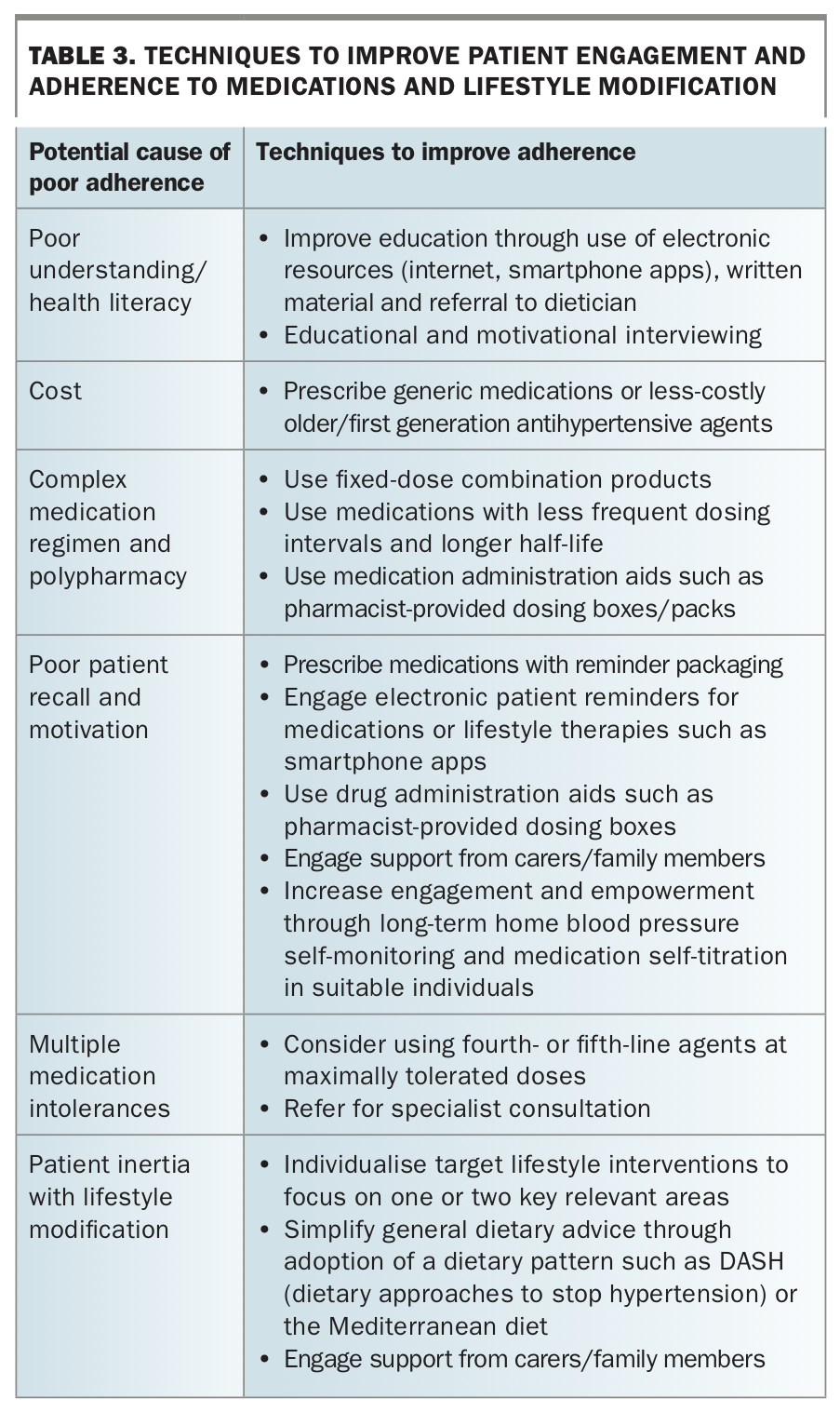
To diagnose resistant hypertension, clinicians must exclude pseudoresistance including white-coat hypertension (where BP is artificially elevated when measured in healthcare settings but is normal in a patient’s home environment), nonadherence to medications or lifestyle interventions, or errors in blood pressure measurement technique.10 Twenty four-hour ambulatory BP measurement or home BP self-monitoring can be useful tools for excluding these possibilities. A thorough assessment of patient adherence to lifestyle modifications and medications is essential. Lack of adherence can account for up to 50% of cases of apparent resistant hypertension.11 Addressing poor adherence due to intentional and nonintentional factors is vital to improving blood pressure control in apparent resistant hypertension. Improving poor adherence requires an individualised and patient-centred approach. Tools to improve patient engagement such as home BP self-monitoring and electronic resources that incorporate an array of behaviour change techniques have been shown to improve blood pressure control in various hypertensive patient populations and may be useful in certain individuals.12-14
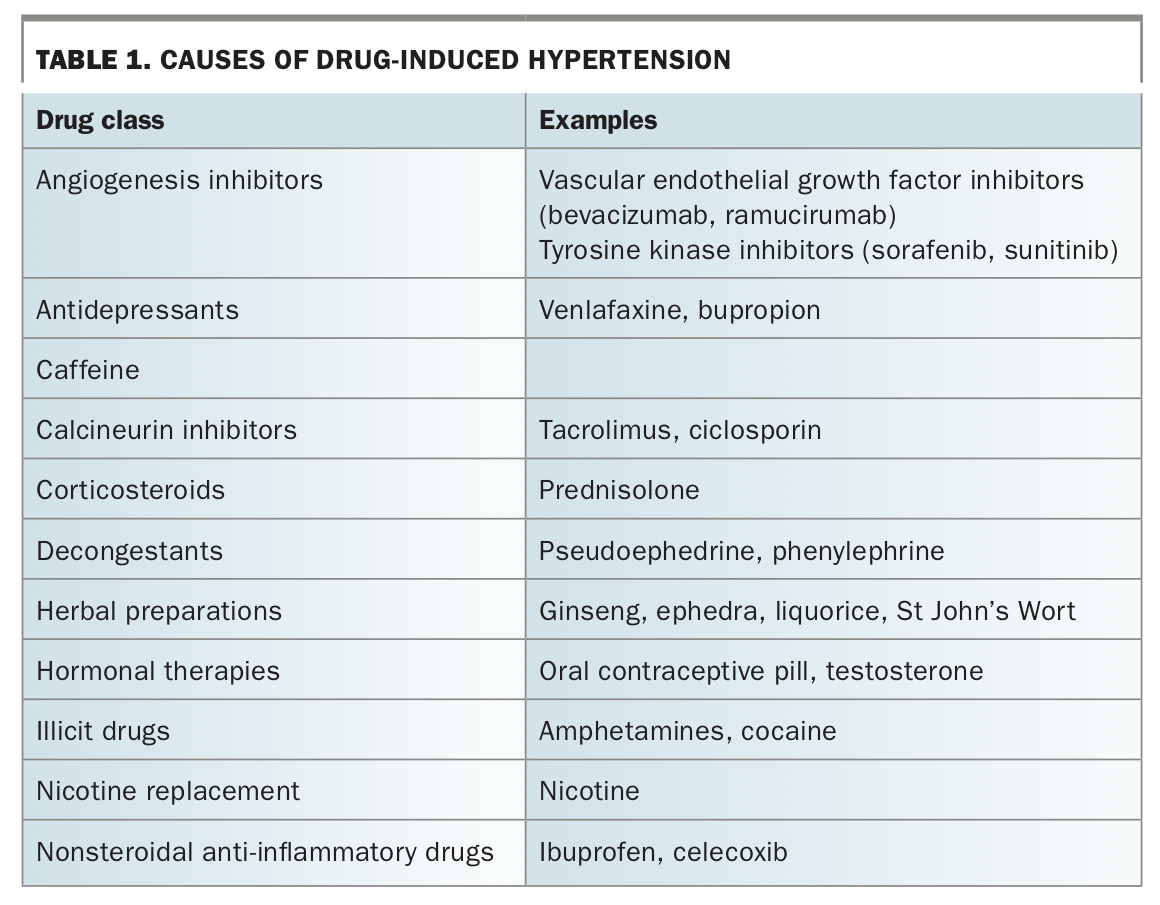
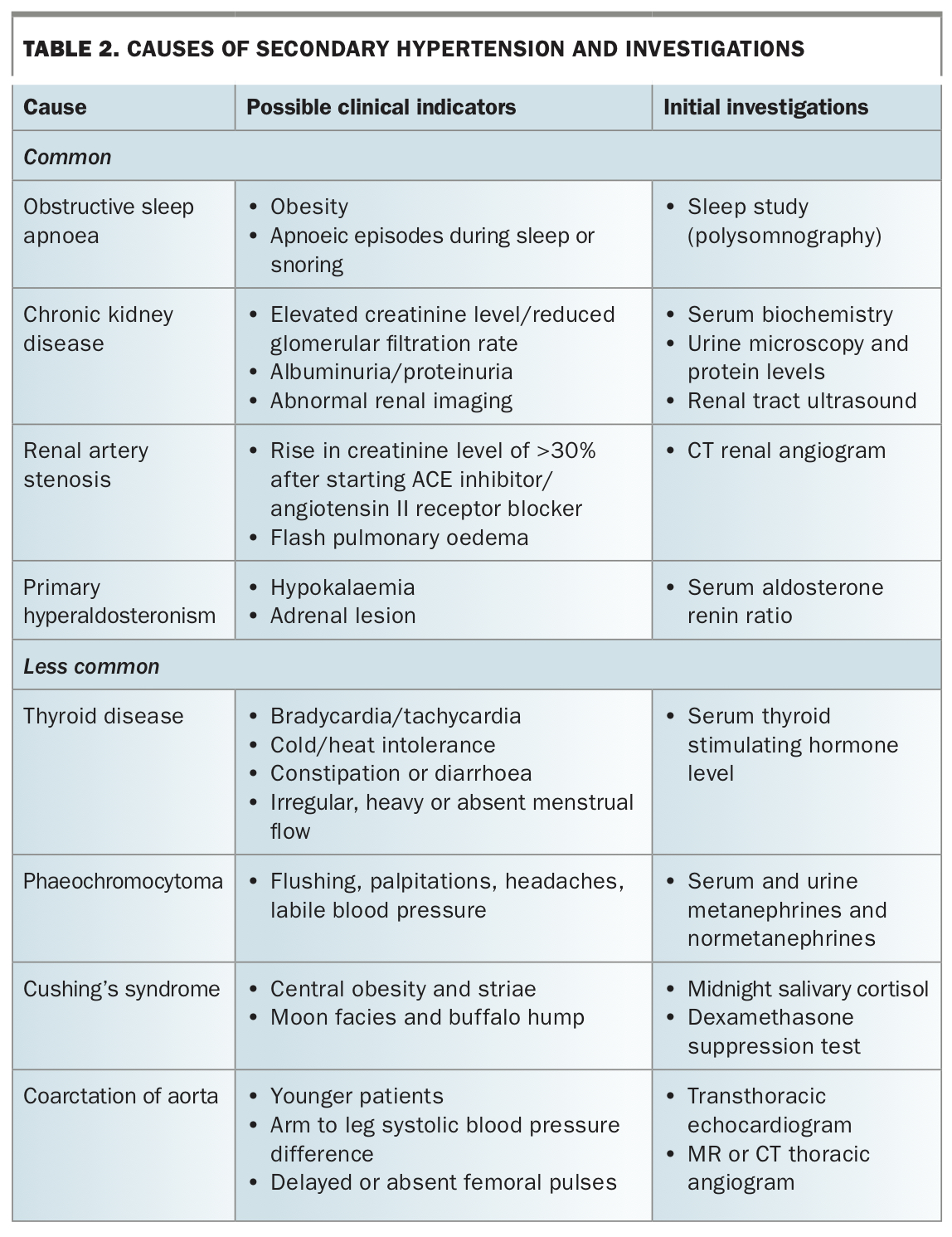
A thorough investigation of secondary causes of hypertension is also required. Secondary causes include substance or drug-induced hypertension from medications and over-the-counter supplements (Table 1), chronic kidney disease (CKD), renal artery stenosis, obstructive sleep apnoea, hypothyroidism, primary hyperaldosteronism, Cushing’s syndrome and phaeochromocytoma (Table 2). Secondary hypertension is more likely present in individuals who are younger (under 30 years of age), present with malignant hypertension, have features of end-organ damage, or have an acute rise in BP after previously stable readings.
{kind=link}
{kind=link}
Lifestyle modification and interventions require optimisation
Strong evidence supporting changes to diet and physical activity in the effective treatment of hypertension exists, and these are recommended in international guidelines.10,15-17 Specific lifestyle interventions proven to lower blood pressure in people with hypertension include:
reducing dietary salt consumption (read food labels and target foods with sodium content less than 150 mg per 100 g, or consume a total of less than 4 g of table salt per day)
- reducing alcohol intake (no more than one standard drink per day)
- smoking cessation
- weight loss
- regular exercise (30 to 40 minutes, at least three times per week if possible).
Although specific targets and thresholds exist for optimal blood pressure management in most hypertension guidelines, there is also supportive evidence that any degree of dietary salt reduction, alcohol reduction or weight loss will likely be beneficial in lowering blood pressure.10,15-17
Lifestyle factors are highly modifiable for most individuals; however, significant therapeutic nihilism and inertia exist. This may be in part because modifying diet and physical activity are among the most difficult therapeutic interventions for patients to adopt with consistent and lasting effects. Significant investment of time and effort from both clinicians and patients is required, and clinically overt benefit may take weeks to months to occur, whereas medication effects are seen within days to weeks. Despite these challenges, persistence is rewarded not only by improved blood pressure control, but by additional improvement for the individual and their household in other important health outcomes such as risk of developing type 2 diabetes and ischaemic heart disease.
Techniques to improve patient engagement and adherence to lifestyle interventions are numerous and require individualisation and effective use of available resources (Table 3). Electronic resources such as websites and smartphone apps have shown efficacy in promoting lasting positive diet and exercise changes in certain patient groups, particularly in relation to dietary salt restriction.18,19 These resources often focus on promoting behavioural change in patients through empowerment, increasing knowledge, increasing motivation and influence.20 This is an exciting and rapidly evolving area; however, ongoing caution is needed as currently only a portion of smartphone apps have been scientifically validated with clinically significant outcomes.
{kind=link}
Pharmacological treatment of resistant hypertension
Patients with resistant hypertension are already on three or more antihypertensive medications at the time of diagnosis. Ideally, these three agents should act through complementary mechanisms and typically include a combination of renin-angiotensin system (RAS) blockade with an angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker, a calcium-channel blocker and a thiazide-type diuretic. Medications should be titrated to maximally tolerated doses. However, in the presence of specific medical conditions such as concurrent heart disease, the initial therapeutic combination may be different and include medications such as beta-blockers.
Several therapeutic strategies should be considered before adding a fourth agent, including:
- combining all drugs into a single pill formulation to simplify the regimen and improve adherence
- modification of dose timing in order to include night-time dosing for at least one agent
- switching to a different type of diuretic.
Thiazide-type diuretics, such as hydrochlorothiazide, chlorthalidone or indapamide are equally considered as first-line diuretic choices in the management of hypertension. In patients with CKD with an estimated glomerular filtration rate (eGFR) of less than 30 mL/min/1.73m2, thiazide-type diuretics may still be used; however, caution is needed, noting greater variability in efficacy and need for closer monitoring for adverse effects.21,22 Loop diuretics (furosemide, bumetanide) are generally preferred first-line diuretic drugs in this group.
Aldosterone excess associated with sympathetic nervous system activation, sodium retention and fluid excess has been described as a key mechanism in the pathophysiology of resistant hypertension.23 The possibility of subclinical hypervolaemia should be considered in every patient with persistently elevated BP. In the case of uncontrolled resistant hypertension despite optimisation of triple therapy, low dose spironolactone (mineralocorticoid receptor antagonist [MRA]) is the preferred fourth-line treatment. This is strongly supported by a recent randomised, double-blind, cross-over trial – PATHWAY-2, which has been incorporated into the latest hypertension guidelines.24
Limitations of spironolactone and use of alternative antihypertensives
Despite its effectiveness, a number of important considerations are required when prescribing spironolactone because of its potential adverse effects that may limit clinical use. Spironolactone needs to be used with caution in patients with an eGFR below 45 mL/min/1.73m2 and/or potassium level above 4.5 mmol/L, as it may lead to a decline in renal function and hyperkalaemia.10,21,22 Furthermore, hormonal adverse effects of spironolactone, such as gynaecomastia and erectile dysfunction in men and menstrual irregularities in women, are frequently encountered. The newer generation aldosterone antagonist eplerenone does not confer the same gender-specific adverse effects but it is not currently available through the PBS for management of hypertension. Amiloride is an alternative potassium-sparing diuretic that reduces systolic BP at a similar magnitude to spironolactone and has a lower propensity for causing hyperkalaemia. Amiloride has recently become unavailable in Australia, and it is unknown if this is temporary or permanent.
Alternative and fourth-line antihypertensive agents are often required for patients with CKD or chronic bradycardia, or for those who experience adverse effects including peripheral oedema. Unfortunately, evidence guiding optimal therapy in these patient groups is often lacking. As an example, patients with CKD have been excluded from most clinical studies to date, such as the PATHWAY-2 trial on the treatment of resistant hypertension. In such patients, a pragmatic approach should be taken when considering any other available antihypertensive class not already in use.10 These include:
- cardioselective beta-blockers (e.g. bisoprolol, metoprolol and atenolol)
- alpha-blockers (e.g. prazosin)
- alpha-2 receptor agonists (e.g. methyldopa and clonidine)
- imidazoline receptor antagonist (e.g. moxonidine)
- vasodilators (e.g. hydralazine or minoxidil).
Novel oral potassium binders
The occurrence or fear of inducing hyperkalaemia has often led to premature discontinuation or suboptimal dosing of RAS blockers or MRAs. More recently, novel potassium binders such as patiromer and sodium zirconium (the latter is not currently available in Australia) have been shown to normalise hyperkalaemia and maintain normokalaemia with an acceptable safety and tolerability profile, as opposed to sodium polystyrene sulfonate which can cause sodium overload and lead to fluid retention. Patiromer is a nonabsorbed, sodium-free potassium binding polymer that exchanges calcium for potassium in the gastrointestinal tract, thereby facilitating potassium excretion and reducing serum potassium levels. The AMBER trial showed that, among patients with resistant hypertension and CKD (eGFR between 24 and 4 mL/min/1.73m2), patiromer enabled more persistent use of spironolactone and reduced the risk of hyperkalaemia by nearly 50% compared with placebo.25 These agents represent an attractive future strategy to circumvent RAS blocker/MRA discontinuation or dose reduction due to hyperkalaemia, although novel potassium binders are currently neither recommended in guidelines nor available through the PBS in Australia.
Interventional treatments for resistant hypertension
The past decade has seen the emergence of interventional endovascular treatments as alternatives or as an adjunct to pharmacotherapy in the management of resistant hypertension. These include catheter-based renal sympathetic denervation, carotid baroreceptor stimulation and carotid body ablation. Current guidelines still exclude device-based therapies for routine treatment of resistant hypertension. Device therapy for true resistant hypertension is an active field of clinical research and may emerge in the next few years as a therapeutic option for carefully selected patients.
Conclusion
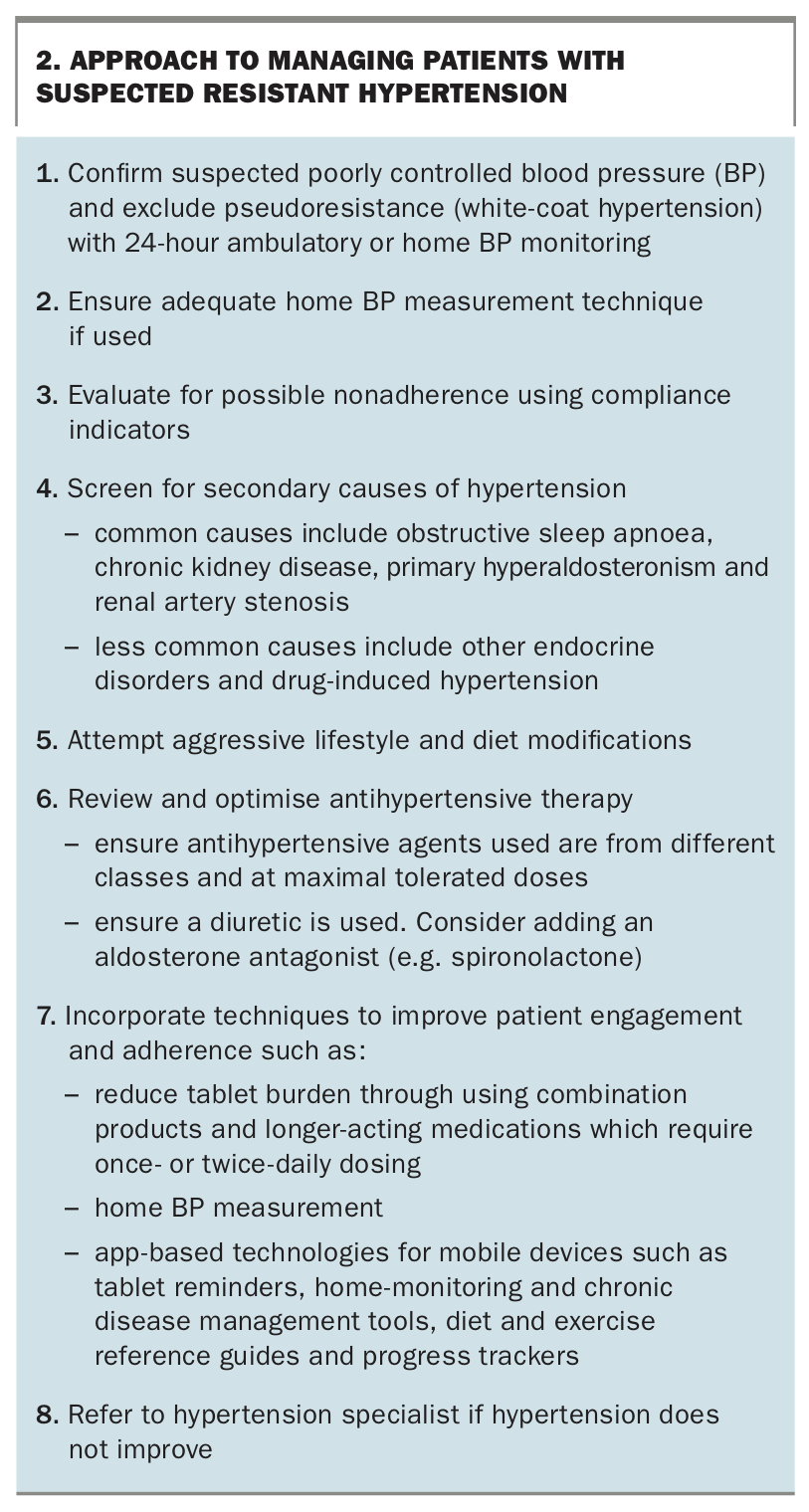
Hypertension is a complex disorder with genetic, physiological and environmental factors at play in each individual. Resistant hypertension must be differentiated from poorly controlled hypertension, pseudoresistance and medication nonadherence before consideration of escalating pharmacological treatment. Any secondary causes of hypertension should be identified and strict lifestyle strategies should be emphasised. An effective approach to the management of resistant hypertension is summarised in Box 2. MT
{kind=link}