Drospirenone 4mg: a new progestogen-only pill

The drospirenone progestogen-only pill became available in Australia in August 2021. With similar efficacy to combined oral contraceptives, it offers another option for those who prefer an oral method and need or desire a method without oestrogen.
A progestogen-only pill (POP) that inhibits ovulation and has a similar efficacy to combined oral contraceptives (COCs) became available in Australia in August 2021. The new POP contains drospirenone 4 mg in a 24/4 regimen. It has many of the advantages of the traditional levonorgestrel 30 mcg and norethisterone 350 mcg POPs (‘mini-pills’) but has been developed to avoid some of their disadvantages. Practice points on the drospirenone POP are summarised in the Box.
{kind=link}
What is the drospirenone 4 mg pill?
The drospirenone 4 mg POP contains 24 tablets of 4 mg drospirenone and four inert tablets. Drospirenone is a fourth-generation progestogen derived from spironolactone that closely matches the pharmacological profile of progesterone. It has antigonadotrophic, antiandrogenic and antimineralocorticoid properties.1
The four-day hormone-free break is a departure from the traditional POP formulation of one active pill each day and was developed to induce a scheduled withdrawal bleed and reduce unscheduled troublesome bleeding. Unscheduled bleeding decreases with duration of use, and around 45% of users are amenorrhoeic by the ninth POP cycle.2
How does the drospirenone POP work?
The contraceptive effect of the drospirenone POP is primarily achieved by inhibition of ovulation through the antigonadotrophic effect of drospirenone, which suppresses luteinising hormone and inhibits follicular stimulation. Drospirenone also thickens the cervical mucus and thins the endometrium.3 Traditional levonorgestrel or norethisterone POPs act primarily by thickening the cervical mucus, with ovulation suppressed in only around 40% of cycles.4,5
The difference in primary mechanism of action between the drospirenone POP and the traditional POPs in Australia accounts for the difference in their missed pill windows. Although the traditional POPs have a narrow missed pill window of three hours, the drospirenone POP has a window of 24 hours and follows the same missed pill rules as the most recent COCs. A desogestrel POP that suppresses ovulation and has a 12-hour window for missed pills has been available in Europe and New Zealand for many years.
How effective is the drospirenone POP?
A pooled analysis of 14,329 cycles in European trials gave an overall Pearl Index (number of unintended pregnancies per 100 person years of exposure) for the drospirenone POP of 0.73. All the pregnancies were considered to be method failures.6
A smaller analysis of 5337 cycles in a US trial gave an overall Pearl Index of 2.7, although there was no indication as to how many of the pregnancies were considered method failures rather than user-related failures. This higher rate of failure in the US trial is similar to rates of failure seen in trials of COCs in this setting.7-9 There was no significant difference in Pearl Index in those with a body mass index of 30 kg/m2 or more compared with those with a BMI less than 30 kg/m2.10
Neither analysis showed a significant difference in Pearl Index in those aged 35 years or younger compared with the overall group.6,10 A small study of 102 young women aged 12 to 17 years, of whom 74 completed 12 months of use, had no unintended pregnancies, although participants were encouraged to use condoms.11
In practice, the effectiveness of the drospirenone POP is likely to be the same as that of COCs, at over 99% in perfect use and 93% in typical use because of the potential for pills to be missed, pill packs to run out and drug interactions. However, the longer missed pill window for the drospirenone POP compared with the traditional levonorgestrel and norethisterone POPs increases the allowable margin for taking a pill on time. Although this difference is likely to make the drospirenone POP more effective than the traditional POPs, comparison data are lacking.12
Return to fertility
In common with other oral methods, there is a rapid return to fertility after cessation of the drospirenone POP. Clinical trial data show a mean postcycle time to ovulation of 13.6 days.3
Safety profile
Venous thromboembolism and other vascular risks
The drospirenone POP has a good safety profile. Drospirenone in combination with ethinylestradiol appears to be associated with a higher risk of venous thromboembolism (VTE) than COCs containing levonorgestrel as the progestogen.13 However, drospirenone in a 24/4 formulation has been shown to lower the production of fibrin products and has no procoagulatory effects.14 Drospirenone is considered safe in relation to VTE risk. There were no reports of VTE in any of the large efficacy trials, nor of arterial thromboembolism, stroke or myocardial infarction.10,15
Breastfeeding
The drospirenone POP is considered safe during breastfeeding, with around 0.11% of the maternal dose passing to the breast milk.16
Bone density
The drospirenone POP maintains mean oestradiol levels comparable with those in people using the etonogestrel implant or the estradiol-nomegestrol acetate combined pill.3,17,18 The drospirenone POP is not expected to adversely impact bone density and can be used without restriction in young adolescents.
Hyperkalaemia
There is a theoretical concern that the antimineralocorticoid activity of drospirenone could result in hyperkalaemia, although no clinically significant cases were reported in any of the clinical trials. It is therefore recommended to check serum potassium levels during the first treatment cycle in patients with renal insufficiency and a pretreatment serum potassium level in the upper reference range, and during concomitant use of potassium-sparing drugs.19
Tolerability and side effects
Drug acceptability was considered ‘excellent/good’ by over 82% of participants in a 13-cycle trial in 713 women aged 18 to 45 years.15 Adverse events were uncommon during the study and were mostly mild or moderate, although some led to study withdrawal (12.3%). The most frequent adverse events were acne (5.5%), abnormal bleeding (1.7%), headache (1.5%) and decreased libido (1.4%).15
Bleeding patterns
Troublesome bleeding and spotting are common reasons for discontinuing progestogen-only methods of contraception.20-22 The drospirenone POP differs from the traditional POPs in that it has been developed to induce a monthly scheduled withdrawal bleed during the hormone-free break with the aim of reducing unscheduled bleeding at other times in the cycle. In reporting of two of the large clinical trials, the difference between spotting and bleeding was not defined.10,23 In the other large trial, spotting was defined as ‘blood loss that did not require new use of any type of sanitary protection’.15 Overall scheduled and unscheduled bleeding and spotting decline and amenorrhoea increases over continued use, and patterns are acceptable to users. Around 3% of participants withdrew from studies because of abnormal bleeding.15,23
Scheduled blood loss
Scheduled blood loss was defined as occurring during or one day either side of the hormone-free interval and lasting up to eight days. Around 90% of users had a scheduled withdrawal bleed or spotting in cycle 1, decreasing to around 55% by cycle 9.23 The median number of scheduled bleeding and spotting days decreased from 2.9 to 2 over the course of 13 cycles.10
Unscheduled blood loss
The number of users with either unscheduled bleeding or spotting stayed reasonably stable over nine cycles at around 45%.23 However, the number of days on which either occurred decreased from 8.8 to 5.5 over 13 cycles.10
Amenorrhoea
Amenorrhoea increased from around 10% in cycle 1 to 45% in cycle 9.6
Prolonged bleeding
Prolonged bleeding, described in one study as an episode of more than 14 days of bleeding or spotting, occurred in 6.5% of participants during cycles 2 to 4, decreasing to 4.2% during cycles 11 to 13.15
Noncontraceptive benefits
The 75 mcg desogestrel POP available in the UK and New Zealand, which acts by the same mechanisms as the drospirenone pill, has been shown to have possible benefit in reducing headaches, migraine, dysmenorrhoea and post-endometriosis surgery-related pain.24-29 Whether the drospirenone POP has similar benefits is largely unknown, although a small study in adolescents showed a progressive reduction in dysmenorrhoea and use of pain medication to control it over 13 cycles.11
No overall clinical benefits have been shown from the antimineralocorticoid effect in relation to fluid retention, body weight or blood pressure (BP). However, a trial in 713 participants found a small decrease in both systolic and diastolic BP in those who had a systolic BP over 130 mmHg or a diastolic BP over 85 mmHg at trial entry but no change in those whose BP was below this level.30
Practical considerations
Eligibility
As for all progestogen-only methods of contraception, there are few contraindications and precautions and few serious risks associated with the drospirenone POP. It can provide an alternative choice for those who have contraindications to oestrogen but prefer an oral method.
In Australia, safety considerations regarding contraception options are guided by the Medical Eligibility Criteria (MEC) system of the UK Faculty of Sexual and Reproductive Health (FSRH).31 This system has four categories, ranging from MEC 1 (no contraindication) to MEC 4 (absolute contraindication).
The only absolute (MEC 4) contraindication to the drospirenone POP is current breast cancer. MEC 3 conditions that require expert clinical judgment or referral include past breast cancer, decompensated cirrhosis, hepatocellular adenoma or malignant liver tumour, or ischaemic heart disease, stroke or transient ischaemic attack that develops during use. Unexplained vaginal bleeding that is suspicious for serious disease such as cervical cancer requires investigation but should not delay initiation of the drospirenone POP.31
Drug interactions
The efficacy of the drospirenone POP is affected by liver enzyme-inducing drugs such as antiretrovirals, some antiepileptics, rifampicin and St John’s wort. Switching to a hormonal or copper intrauterine device (IUD) or a depot medroxyprogesterone injectable is recommended for people taking liver-enzyme inducers long term.
Use across the reproductive life course
Adolescence
A small study of people aged 12 to 17 years showed the drospirenone POP was well tolerated and acceptable.11 No effect is expected on bone mineral density. However, as the drospirenone POP is not PBS-listed, the higher cost may be a deterrent for adolescents.
Postpartum
The drospirenone POP is considered safe to use immediately postpartum (off label) and during breastfeeding, with negligible amounts of the maternal dose passing into the breast milk.16
Perimenopause
Similar to the traditional low-dose POPs, the drospirenone POP can be continued beyond the age of 50 years until it is either no longer required or up to the age of 55 years. Given that amenorrhoea associated with the drospirenone POP cannot be distinguished from amenorrhoea due to menopause, individuals who have been amenorrhoeic for 12 months since turning 50 years of age can have a single measurement taken of follicle stimulating hormone (FSH) to aid clinical decision-making. If the FSH level is above 30 IU/L, the POP can be safely stopped after a further 12 months. If it is 30 IU/L or below, the measurement can be repeated 12 months later.
Notably, unlike the 52 mg levonorgestrel IUD, the drospirenone POP cannot be used to protect the endometrium as part of menopausal hormone therapy (MHT). However, for women experiencing vasomotor symptoms who still require contraception, it can be used alongside cyclical combined MHT.32
Initiation of the drospirenone POP
Each 28-day cycle consists of daily administration of one active tablet for 24 consecutive days followed by one inert tablet for four consecutive days.
The drospirenone POP is immediately effective if:
- started on days 1 to 5 of a regular menstrual cycle
- started less than 21 days postpartum
- started within five days of an abortion.
The recommendation to start on days 1 to 5 of a regular menstrual cycle is based on guidance for all progestogen-only methods from the FSRH.12 The product information advises starting on day 1 of a natural cycle for immediate effectiveness, with the additional use of condoms for seven days if started at any other time.19
The drospirenone POP can be initiated using the Quick Start method at any stage of the menstrual cycle starting with an active hormone pill, with the additional use of condoms for the first seven days of active pill taking.33 If pregnancy cannot be excluded, a pregnancy test is recommended four weeks after initiation.
Advice on switching to the drospirenone POP from other contraceptive methods is detailed in the Table.
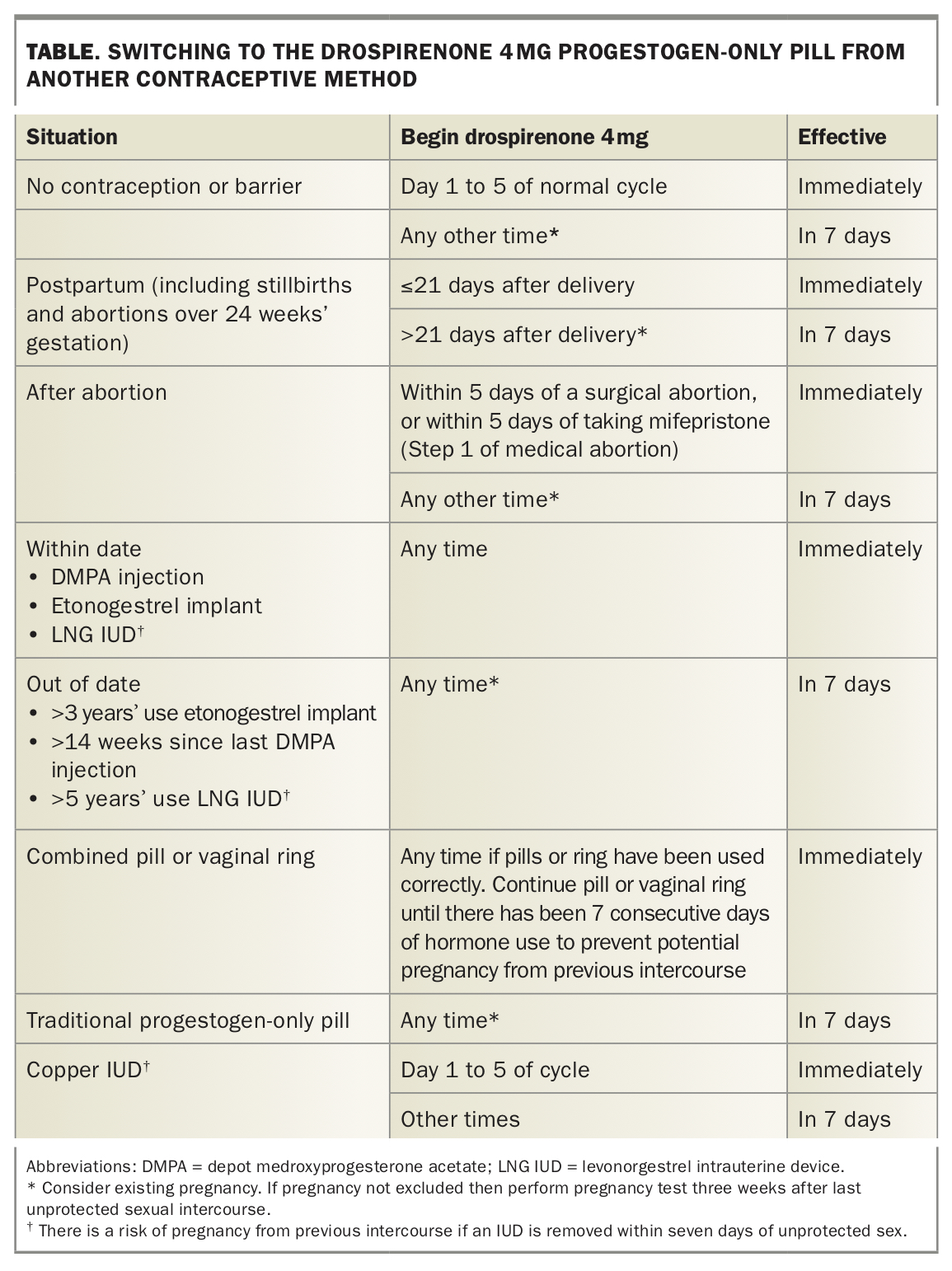{kind=link}
Missed pill advice
A study that involved four fixed scheduled delayed intakes of 24 hours each on day 3, 6, 11 and 22 of the 24 active pills over two cycles followed by a double dose the following day found that inhibition of ovulation was maintained.34 As a result the missed pill advice is the same as that for the newer COCs on the market (Flowchart).
Conclusion
The drospirenone POP offers an additional contraceptive choice for individuals who prefer an oral method of contraception and either need or desire a method without oestrogen. It is not listed on the PBS. The primary mechanism of action of the drospirenone POP as a reliable anovulant results in a longer missed pill window than for traditional POPs. This attribute, together with its good safety profile in relation to VTE and other vascular risks, and increasing rates of amenorrhoea with longer duration of use, may make it a suitable option for women across the reproductive life course. MT
COMPETING INTERESTS: Associate Professor Bateson has received support to present at educational conferences and attend advisory committees on behalf of Family Planning NSW from Bayer Healthcare, MSD and Mayne Pharma Women’s Health. Dr McNamee has received sponsorship from Bayer Australia and New Zealand to attend an educational event on behalf of Family Planning Victoria. Family Planning Victoria was paid for consultative advice given by Dr McNamee to MSD. Family Planning NSW and Family Planning Victoria receive funding for educational courses and training from Bayer Australia and New Zealand and MSD Australia.