Obstructive sleep apnoea and obesity

Weight loss should be recommended to all patients with overweight or obesity who have obstructive sleep apnoea, as it may reduce the severity of sleep apnoea or in rare cases even cure it. Weight loss also has positive impacts on sleep quality, quality of life and other obesity-related diseases such as type 2 diabetes and hypertension.
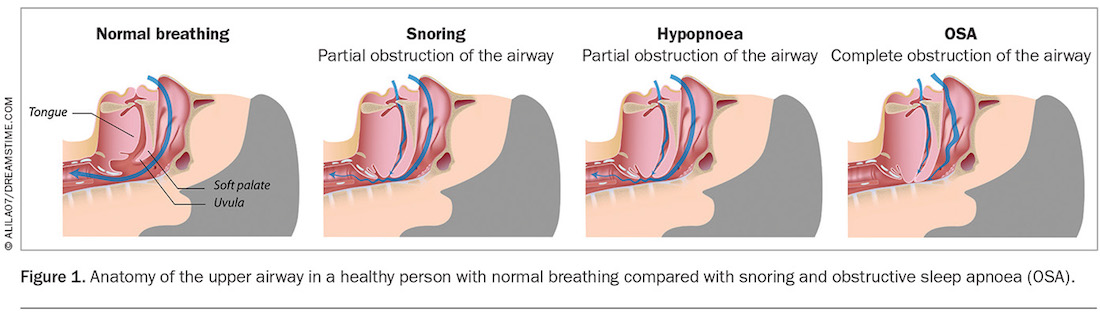
Obstructive sleep apnoea (OSA) is a sleep disorder in which there are episodes of partial (hypopnoea) or complete obstruction (apnoea) of the upper airway during sleep (Figure 1). These episodes lead to oxygen desaturation, increased respiratory effort, increased cortical arousal and sleep fragmentation. OSA is often underdiagnosed as it develops slowly and occurs predominantly during sleep or symptoms are misattributed to busy lives and chronic sleep deprivation.
{kind=link}
Patients with OSA typically present with snoring, witnessed apnoeas, choking episodes, unrefreshing sleep and significant daytime lethargy and somnolence. Mood changes, nocturia, impotence and insomnia may also be presenting symptoms. Many patients present late, or justify their symptoms of daytime lethargy and somnolence as due to busy lives, working long hours, children and other commitments. OSA is associated with significant health impacts, including hypertension, cardiac arrhythmias particularly atrial fibrillation, type 2 diabetes, heart failure, coronary artery disease, stroke and death.
The link between OSA and obesity
Obesity is strongly linked to the presence of OSA. In fact, obesity, particularly central obesity, is potentially one of the strongest risk factors for OSA with changes in weight in both directions having significant influences on prevalence and severity of sleep disordered breathing. Weight is also one of the only potentially modifiable risk factors. Other risk factors for OSA include family history of sleep apnoea and a narrow upper airway. Being male or a postmenopausal woman, increasing age, allergies, enlarged tonsils, alcohol intake, smoking and a blocked nose may also contribute to the risk of sleep apnoea.
With the prevalence of obesity and overweight increasing, it is expected that there will be a parallel significant increase in the prevalence of OSA. Weight gain increases the risk of OSA by increasing upper airway collapsibility during sleep. Upper airway fat deposits also narrow pharyngeal calibre and increase upper airway resistance. Resultant negative intrathoracic pressure shifts combine with increasing central obesity to increase the work of breathing during sleep and the risk of nocturnal hypoventilation. The combination of all of these factors predisposes patients with OSA to upper airway collapse during sleep. Obesity is also associated with a reduction in lung volumes, especially functional residual capacity (FRC), further contributing to increased work of breathing. FRC is linked to airway calibre through neural reflex mechanisms that additionally lead to decreases in upper airway size and increased airflow resistance.
OSA may also have an impact on obesity and cause weight gain, with sleep fragmentation, unrefreshing sleep, daytime lethargy and somnolence leading to reduced physical activity and energy expenditure.1 Lack of energy from unrefreshing sleep may also lead to patients craving a high-energy diet causing further weight gain.
Sleep deprivation has also been linked to obesity, particularly in paediatric populations.2 Chronic short sleep also seems to lead to adverse metabolic outcomes including insulin resistance or dyslipidaemia.3
Obesity is thought to explain 30 to 50% of the variance in apnoea–hypopnoea index (AHI).4 It is estimated that 41% of cases of mild OSA and 58% of cases of moderate to severe OSA in adults are due to obesity.5 Distribution of weight may also impact on severity with predominantly central obesity and increased neck circumference being the most likely associated with OSA.6
Longitudinal population-based studies have shown that a 10% weight gain predicted a 32% increase in AHI, whereas a 10% weight loss predicted a 26% decrease in AHI.7 The Sleep Heart Health Study similarly confirmed progression and regression of sleep-disordered breathing with weight gain and loss, respectively, but also demonstrated that the association was stronger for men than for women.8
Patient assessment
Simple screening questionnaires may be helpful in assessing the risk of sleep apnoea. Currently, there are multiple validated screening tools for OSA. The most commonly used in Australia include STOP-Bang, OSA50 and Berlin questionnaires, while the Epworth Sleepiness Scale (ESS) is often used to assess the severity of sleepiness present. Currently, the MBS funds home sleep studies for patients with a STOP-Bang score of 3 or more or an OSA50 score of 5 or more, in addition to an ESS score of 8 or more.9
These OSA screening questionnaires tend to have a high sensitivity but poor specificity. Most patients who have OSA will screen positive on these questionnaires; however, there will also be a large number of false-positive results.
Screening questionnaires alone are inadequate for diagnosing patients with OSA. Those who have a positive screening test should proceed to further evaluation with a diagnostic sleep study or clinical assessment by a sleep physician.
Weight loss as a treatment of OSA
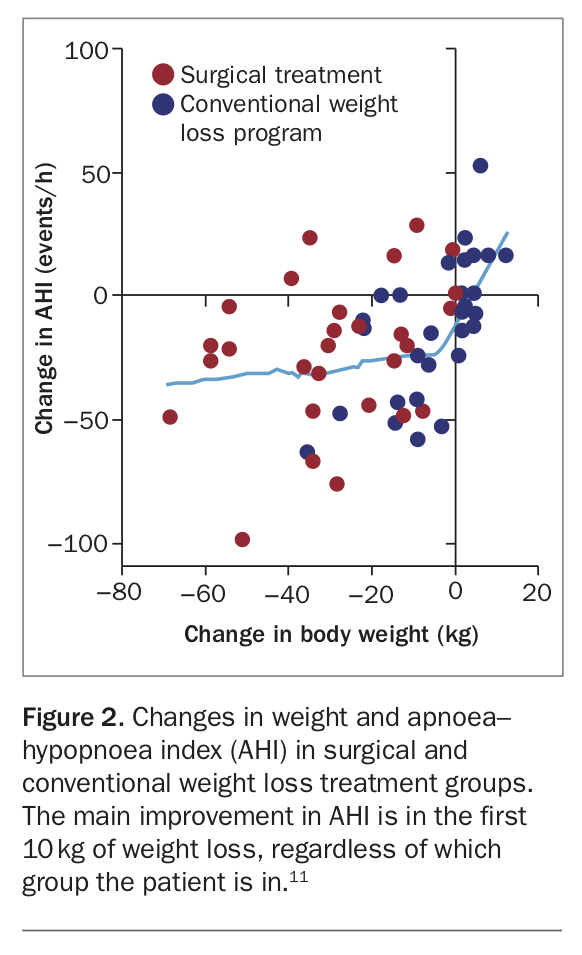
Weight loss is often recommended as a treatment modality for patients with all severities of OSA. Multiple methods of weight loss are suggested, such as lifestyle modification, medication, very low-calorie diets and bariatric surgery. Despite the method of weight loss used, weight loss has a significant but variable effect on severity of OSA.10 The main effect on severity of OSA is seen in the first 8 to 10% or 10 kg weight loss across all severities of OSA.11
In patients with mild to moderate OSA, meta-analyses have shown that weight loss via lifestyle interventions caused improvements in AHI, oxygen desaturation and symptoms. However, substantial heterogeneity between studies was present.12
In patients with severe OSA, meta-analyses that compared medical versus surgical weight loss showed high heterogeneity between studies.10 Most of the benefits of weight loss on severity of sleep apnoea appeared to be in the first 8 to 10% or 10 kg of weight loss regardless of whether by medical or surgical means, and great interpersonal variability was present.11 Despite the improvements in weight loss and sleep apnoea, in most patients, ongoing significant OSA was present and still required treatment.
In a randomised controlled study that compared surgical versus medical weight loss, there was a large heterogeneity in the effects of weight loss on severity of OSA in both groups (Figure 2).11 Heterogeneity was high across all outcomes. One participant even lost 55 kg with no change in AHI.12
{kind=link}
Despite improvements in symptoms and severity of OSA with weight loss, ongoing objective assessment of sleep apnoea with polysomnography is required in all patients. It is likely that significant OSA will persist and will require ongoing treatment with other modalities such as CPAP or a mandibular advancement splint.
Weight loss itself may also improve sleep quality and quality of life, in addition to reducing the severity of OSA.13,14 Therefore improvements in symptoms may not always predict improvements in OSA severity.
Studies have shown that obesity itself may cause sleep disruption in the absence of sleep apnoea.13 After weight loss, improvements in symptoms may therefore be due to a combination of improvements in sleep apnoea, sleep quality and quality of life.13,14
Does CPAP therapy assist with weight loss?
Continuous positive airways pressure (CPAP) blows air into the upper airway during sleep and pneumatically splints the upper airway open, preventing partial or complete upper airway obstruction. CPAP is an effective treatment for snoring and for all severities of OSA.
Despite significant improvements in symptoms of daytime lethargy and somnolence, and increased energy levels with starting treatment with nasal CPAP, there is no evidence that starting treatment with nasal CPAP promotes weight loss. Data actually suggest that patients gain a small amount of weight when they start CPAP.15
Patients with significant OSA require appropriate treatment to reduce the metabolic risk factors of sleep apnoea, improve quality of life and reduce the symptoms of unrefreshing sleep and significant daytime lethargy and somnolence.
Conclusion
Obesity is a significant risk factor for the development of OSA. Weight loss itself and not the method of weight loss confers the improvements in OSA. The greatest improvements in sleep apnoea with weight loss appear to be with the first 8% to 10% or 10 kg of weight loss.11 However, marked heterogeneity in the effects of weight loss on OSA are present.
Despite potential significant improvements in OSA severity with weight loss, it is unlikely that OSA will completely resolve (AHI less than 5 events per hour). Ongoing monitoring and treatment of OSA is required to minimise the long-term risks of OSA. Ongoing long-term monitoring is also needed as severity of OSA is likely to increase over time if weight gain recurs after weight loss or even if weight is stable.
Weight loss should be recommended for all patients with overweight or obesity who have OSA regardless of the severity, as it may reduce the severity of sleep apnoea or in rare cases even cure it, and also has positive impacts on sleep quality, quality of life and other obesity-related diseases such as type 2 diabetes, and hypertension. Despite the potential improvements in severity of OSA with weight loss, marked heterogeneity is present, and treatment of OSA is required with follow up to make sure that it is adequately controlled. MT
COMPETING INTERESTS: None.