Allergic rhinitis: the importance of medical therapy

Rhinitis
Allergy
Sinus surgery can provide some relief for patients with allergic rhinitis but medical treatment must be continued to ensure symptoms do not recur.
Case scenario
Monica, a 45-year-old patient, has suffered from allergic rhinitis throughout her life. About 12 years ago she underwent functional endoscopic sinus surgery (FESS) to improve drainage and assist her breathing and she was very happy with the result. However, she now presents to your practice complaining that she has been unable to breathe through her nose for some time now because of tissue swelling, rather than a build up of mucus. She has seen her original ENT surgeon but he told her that further surgery is unlikely to relieve her symptoms. She has tried many different nasal sprays and routines but says none of them help her. She is frustrated and feels there must be something that can be done to assist her.
What other options are likely to reduce the tissue swelling in Monica’s nose and assist her to breathe more freely through her nose?
Commentary
Allergic rhinitis, often referred to as ‘hay fever’, is a commonly underestimated inflammatory condition caused by a type 1 hypersensitivity reaction (IgE [immunoglobulin E]-mediated allergy) in response to common aeroallergens such as dust mite, animal dander, pollens and moulds. One in five people in Australia (almost 4.5 million people) suffered from allergic rhinitis in 2014-15.1
Allergic rhinitis considerably reduces quality of life with 50 to 80% of people with allergic rhinitis reporting their condition interferes with sleep, decreases alertness, and causes daytime fatigue, an inability to concentrate, depression and irritability.2 Allergic rhinitis is often underdiagnosed, undertreated and suboptimally managed.2 Patients with allergic rhinitis often consider it a ‘nuisance’ with no effective treatment but allergic rhinitis can effectively be managed.
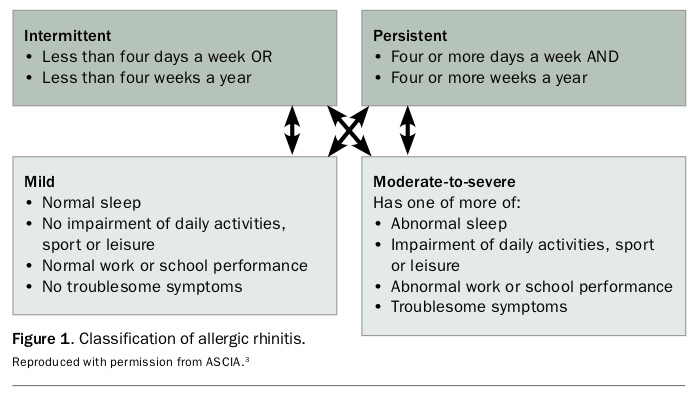
Before 2001, allergic rhinitis was classified according to the time and type of exposure to allergens, as either seasonal allergic rhinitis or perennial allergic rhinitis. Currently, allergic rhinitis is classified according to the duration of symptoms (intermittent or persistent) and the severity of symptoms (mild or moderate to severe; Figure 1).3
{kind=link}
Classic symptoms of allergic rhinitis are nasal itching, sneezing, rhinorrhoea and nasal congestion. Ocular symptoms also frequently present, with allergic conjunctivitis being associated with itching and redness of the eyes and tearing. Other symptoms include itching of the palate, postnasal drip and cough. Symptoms are often characterised either by nasal obstruction and rhinorrhoea or by pruritus and itchy symptoms. Nasal obstruction is the most complained about symptom and has the greatest impact on patients’ sleep and quality of life. Significant airway obstruction can also limit the delivery of appropriate medications, hampering treatment.
Course of Monica’s allergic rhinitis
Monica’s case is quite typical for patients presenting to allergists and rhinologists. Let’s analyse her disease course.
Monica has had a lifetime of symptoms. Up to 12.5% of children have allergic rhinitis, increasing to 25% of middle-aged adults in Australia.1 Allergic rhinitis is most prevalent during the middle years of life, between the ages of 15 and 59 years, and unlike with asthma most patients do not ‘grow out’ of allergic rhinitis.
Allergic rhinitis is also frequently associated with asthma, which is found in up to 40% of patients with allergic rhinitis, and nasal symptoms of rhinitis are present in up to 85% of patients with asthma. Allergic rhinitis is a major risk factor for developing asthma and it significantly increases the risk of having poor asthma control. The greater the severity of rhinitis, the greater the likelihood the patient will have asthma. The severity of rhinitis has also been shown to be a stronger predictor of poor asthma control than smoking or noncompliance with medications.4
As asthma and allergic rhinitis are upper and lower respiratory tract manifestations of the same inflammatory processes, this is often known as the united airway disease. Sinusitis is also part of the ‘united airway disease’.
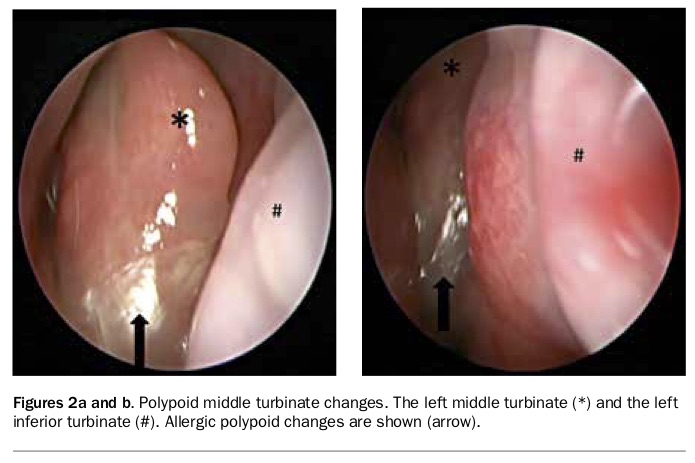
Although part of the same process, the incidence of allergic rhinitis is not any greater in patients with chronic rhinosinusitis than in the normal population. Allergic rhinitis can aggravate chronic rhinosinusitis so that patients with both chronic rhinosinusitis and allergic rhinitis often have worse quality of life or seem more difficult to treat; however, there is limited evidence to suggest that allergic rhinitis plays a substantial role in the aetiology of chronic rhinosinusitis. A subset of patients who present with nasal polyps and moderate-to-severe persistent allergic rhinitis may have such severe inflammation in the nasal airway that they develop oedema of the middle turbinates, which when severe can become polypoid and cause secondary obstruction of the sinuses (Figures 2a and b). This is now described as ‘central compartment atopic disease’.5
{kind=link}
Monica has undergone FESS, so her sinuses have been ‘opened’ but not necessarily her airway. Often surgeons focus on secondary obstructive changes in the sinuses rather than the inflammation of the nasal airway that led to them. Most patients with allergic rhinitis who fail appropriate medical treatment and complain of persistent nasal obstruction will benefit from nasal surgery addressing the inferior turbinates with or without addressing the septum. Septoplasty is only required if there is a significant mechanical obstruction from a deviated septum. However, FESS is seldom required in patients with allergic rhinitis.
Nasal surgery improves airflow and facilitates better delivery of medications but does not eliminate the allergic rhinitis. The patients all remain ‘allergic’ after the surgery, with no change to the pathophysiology of the disease. However, when patients no longer feel ‘blocked’ or if their rhinorrhoea improves significantly they do get the false impression that they have been ‘cured’ and often stop medical management.
Further complicating this is the additional benefit gained from some of the newer turbinate surgery techniques including a medial flap inferior turbinoplasty. This technique lifts the medial surface of the inferior turbinate to preserve it and removes the vertical part of the underlying inferior turbinate bone, allowing for significant improvement in the airway. It also damages the parasympathetic nerves that run along the inferior branch of the sphenopalatine turbinate artery and, as many allergy symptoms are mediated along the parasympathetic pathway, this gives patients an allergy ‘holiday’ with fewer allergic symptoms, but this effect is always temporary. Patients tend to get excellent initial results regardless of the surgical technique employed but eventually their symptoms return if an ongoing medical plan is not restarted.
Treatment
Monica has enjoyed the benefits of the initial surgery but neglecting ongoing care of her allergy has resulted in recurrent symptoms. Surveys have shown that patients in Australia tend to use poly-pharmacy and are usually frustrated by persistent nasal symptoms, and the failure of the treatments to act fast and help ocular symptoms.2,6
The recommended first-line treatment for patients with moderate-to-severe symptoms of allergic rhinitis is combination therapy with intranasal corticosteroids and an intranasal antihistamine. This provides rapid symptom relief and a sustained improvement of symptoms. Several studies have confirmed the synergistic effect of combining topical intranasal corticosteroids and topical intranasal antihistamines.7,8
Monica should start to use a combination spray after being shown how to administer it correctly to minimise adverse effects. She should be encouraged to continue this treatment in the long term. The Allergy Diary App can assist patients in monitoring their progress, remind them to take their medications, allow a full -picture of their symptoms using visual analogue scales to measure daily symptoms and track their progress (www.allergydiary.com/allergy-diary-app).9
Once Monica has established a routine and compliance with her medications has been improved, further investigations can be considered if her symptoms are still troublesome. Confirmation of the diagnosis using skin prick tests or immunoassay for serum-specific IgE to aeroallergens is useful and allows assessment of her suitability for immunotherapy. Immunotherapy can be highly effective and is the only treatment that can modify the natural history of allergic rhinitis and offer the potential for long-term disease remission. Immunotherapy can be offered as a subcutaneous injection or sublingual tablets or drops. Compliance issues can occur due to the cost, adverse effects and long treatment course required for initial symptom improvement (three to six months) and a full course (at least three years). However, if appropriate medical management has failed then immunotherapy is an option to consider.
Adjuvant therapies such as saline rinses may give marginal additional symptom relief for patients with allergic rhinitis. Occasionally, oral corticosteroids can be used briefly and always in combination with a topical intranasal corticosteroid for severe nasal obstruction or uncontrolled symptoms despite combination topical intranasal therapy (recommend 0.5 mg/kg in the morning after food for five to seven days).
Finally, depending on the initial surgeon’s approach, occasionally there is a role for revision surgery. Referral to an ENT surgeon with subspecialty interests in rhinology is recommended. Often revision surgery will address the inferior turbinates using a more effective approach, such as the medial flap inferior turbinoplasty discussed above. However, a more complete nasal airway assessment is always performed and other areas including the external valve, internal valve, septal deviation and polypoid middle turbinates need to be assessed and persistent sinusitis and nonallergic rhinitis excluded.
Conclusion
Most patients with allergic rhinitis will respond well when the above plan is initiated. Patient education, appropriate medical therapy, confirmation of disease, immunotherapy and revision surgery are all options for Monica. MT