Allergic rhinoconjunctivitis. Allergen-specific immunotherapy options in Australia

Dr Chan is Clinical Immunology and Allergy Registrar in the Department of Clinical Immunology and Allergy, The Royal Melbourne Hospital, Melbourne. Dr Nicholls is a Clinical Immunologist and Allergist in the Department of Clinical Immunology and Allergy, The Royal Melbourne Hospital, Melbourne; and an Immunopathologist at Dorevitch Pathology, Melbourne, Vic.
Rhinitis
Allergy
Allergen-specific immunotherapy (AIT) has traditionally been reserved for patients with moderate-to-severe allergic rhinoconjunctivitis that is refractory to maximal pharmacotherapy. However, there is mounting evidence that AIT should be considered not simply a symptom- control measure, but also a curative tool that may alter the course of allergic disease. Although specialist assessment is required to initiate treatment, GP familiarity with AIT administration, risks and benefits is crucial to maximising patient safety and satisfaction.
- Confirmation of sensitisation to a clinically relevant allergen is central to management of allergic rhinoconjunctivitis (ARC).
- Allergen-specific immunotherapy (AIT) should be considered for patients with moderate-to-severe ARC, particularly when nonallergen-specific pharmacotherapy has failed.
- AIT should be considered as a therapeutic option for managing asthma in allergen-sensitised patients and is particularly relevant for patients with a history of ‘thunderstorm asthma’.
- AIT is generally contraindicated in poorly controlled asthma and absolutely contraindicated in active or refractory autoimmune disease; AIT should not be initiated during pregnancy.
- Factors that may influence the choice of AIT include: allergen sensitisation and availability of a relevant allergen product; regulatory approval of products; cost; convenience of administration; and risk of adverse effects.
- The modality of AIT and specific allergen should be selected after thorough specialist assessment, according to the individual patient’s clinical features, pattern of allergen sensitisation and personal preference for therapy.
Allergic rhinoconjunctivitis (ARC) is often perceived to be a relatively benign and even trivial condition; however, it imposes a significant burden on the community and affected individuals. Allergic diseases are among the most common noncommunicable illnesses in Australia and worldwide, with a prevalence reported to be as high as 32% in Australia.1 The south-eastern states and Western Australia have higher rates than Queensland and the Northern Territory owing to the widespread distribution of temperate grasses in these areas, especially Lolium perenne (perennial rye grass).2
ARC has been shown to negatively impact on quality of life, quality of sleep and productivity at school and in the workplace. The subsequent presenteeism and absenteeism have major implications for the economy, as most people affected by allergic disease are 15 to 64 years of age. Furthermore, the prevalence of these diseases is projected to rise by about 70% by 2040.3 Although specific data on ARC medication expenditure are not available, it has been recognised that over a 10-year period from 2001 to 2010, spending at pharmacies in Australia on allergy medications doubled, from just over $100 million to over $226 million.2 In 2007, the cost of symptom-relief therapies for individuals with severe ARC was estimated to be more than $500 per year. In addition, allergic conditions pose a considerable financial burden on society, with indirect costs estimated in 2007 to exceed $1500 per individual per year.3
ARC is defined as the symptomatic response to immunoglobulin E (IgE)-mediated inflammation within the nasal and ocular mucosa, which is triggered by exposure to an aeroallergen in a sensitised individual. Clinical symptoms may include nasal obstruction, rhinorrhoea, sneezing, nasal and ocular itching and postnasal drip; however, similar symptoms may also be seen in some patients with nonallergic rhinitis or chronic rhinosinusitis, and therefore confirmation of sensitisation (through detection of specific IgE in the serum or positive skin prick tests) to a clinically relevant allergen is crucial to employing the correct management. Management may be targeted at three areas of the allergic process: minimising allergen exposure, managing symptoms with nonallergen-specific pharmacotherapy, or focused interruption of the allergic pathway with stimulation of tolerance to the allergen with the use of allergen-specific immunotherapy (AIT).
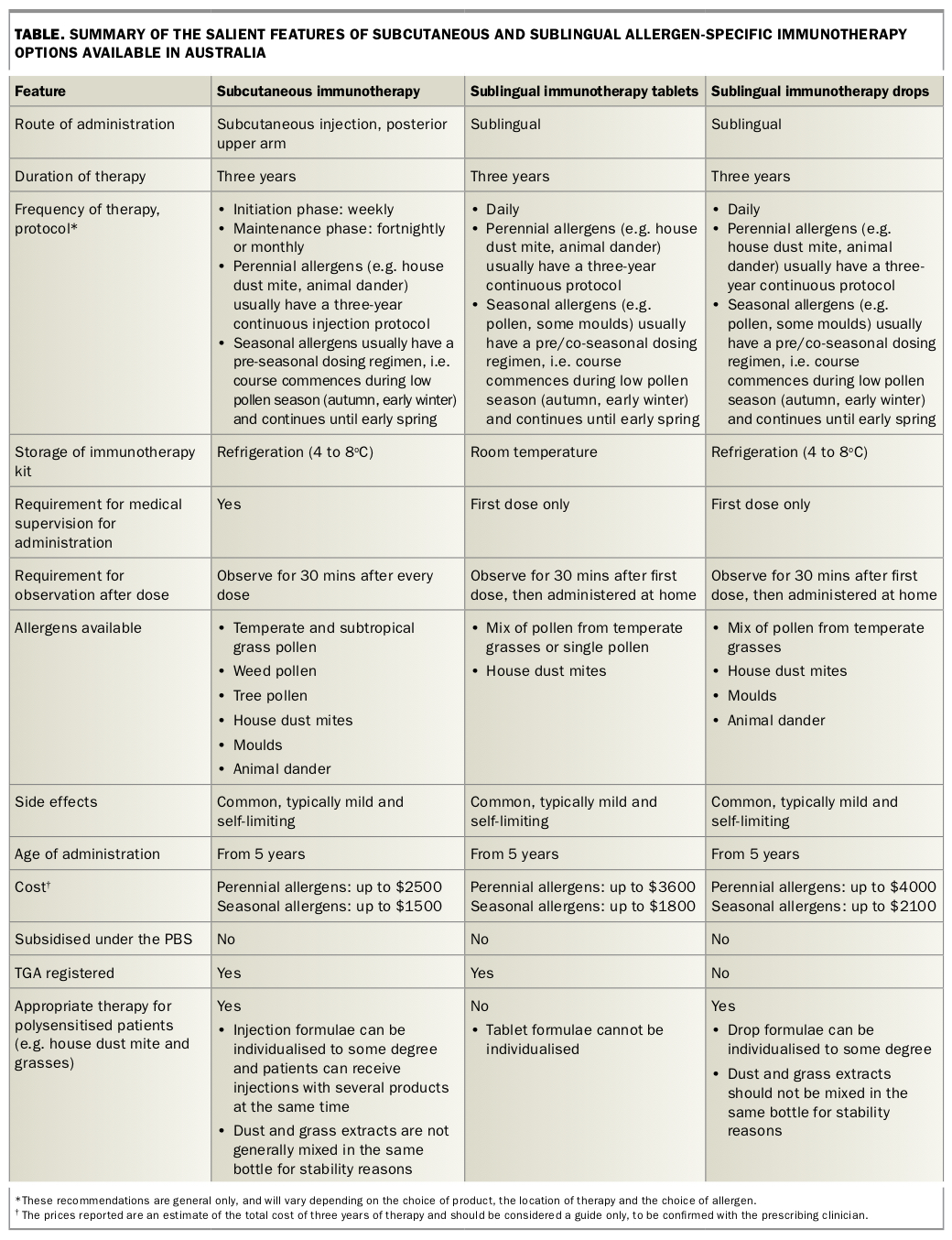
This article discusses recent advances in allergen-specific immunotherapy, with the aim of providing primary care physicians with a greater understanding of the available options (Table) and potential risks and benefits of these interventions. A more thorough overview of the ARC diagnostic process, allergen avoidance and nonallergen-specific pharmacotherapy can be found in the October 2014 issue of Medicine Today.4
{kind=link}
Allergen-specific immunotherapy
Despite the use of pharmacotherapy in more than 90% of patients with ARC, symptom burden is still high, with almost one-third of children and two-thirds of adults reporting incomplete relief of symptoms.5,6
Subcutaneous immunotherapy (SCIT) for grass pollen allergy was first reported in 1911 by Leonard Noon. Sublingual immunotherapy (SLIT) was first used for grass pollen allergy in 1936; however, SLIT initially demonstrated lower efficacy compared with SCIT.7 The use of SLIT, especially in Europe, has increased significantly over the past 25 years, with some of this shift triggered by safety concerns and the subsequent restricted availability of SCIT products.8
AIT aims to shift the immune response to a tolerant phenotype via induction of regulatory T cells. This is achieved by exposure to an initially increasing then constant level of allergen for three to five years. AIT attenuates symptoms and reduces medication requirements, with a sustained response for several years after discontinuation of therapy.9
Well-powered randomised placebo-controlled trials exploring the effects of SCIT and SLIT on ARC have demonstrated an average reduction in nasal and ocular symptoms of 32 to 36% with SCIT and 26 to 36% with SLIT. A recent Cochrane meta-analysis showed that SLIT decreased medication scores by 32% compared with placebo. SCIT reduced medication scores by 57% in patients receiving AIT for seasonal allergens; however, despite a reduction in symptom scores, there was no significant reduction in medication use in patients receiving AIT for perennial allergens.6
Choice of patient
International guidelines advise that AIT should be considered for patients with moderate to severe ARC, especially those in whom pharmacotherapy has failed.10 However, there is mounting evidence that AIT is not just an effective ARC treatment but may also alter the course of allergic disease development and reduce exacerbation frequency and severity in allergic asthma.11,12 There is increasing evidence that AIT has good efficacy and safety in patients with allergic asthma. Multiple randomised controlled trials have shown that judicious use of both house dust mite and pollen SCIT and SLIT may delay the development of asthma in individuals with ARC. To date, this preventive effect has been reported to persist for at least 10 years for some allergens, although the data are somewhat conflicting with regard to the size of this effect and further studies are required for clarification.11
As about 50% of patients with ARC also have asthma, it is important to note that AIT may also benefit those who already have allergic asthma. In patients with well-controlled, mild-to-moderate disease, AIT has a corticosteroid-sparing effect, improves quality of life and reduces allergen-specific airways hyper-reactivity.12 AIT should therefore be considered as a therapeutic option in the general framework of asthma management in allergen- sensitised patients. This is particularly relevant to patients with a history of ‘thunderstorm asthma’. It has been shown that seasonal ARC and sensitisation to perennial rye grass pollen were the most significant risk factors for susceptibility during the Melbourne thunderstorm asthma event of 2016.13
Choice of treatment
When compared with placebo, both SCIT and SLIT have been extensively shown to provide significant benefit for the symptoms of ARC, reduce medication use, improve quality of life and reduce progression from allergic rhinitis to asthma.14 Indirect comparisons by meta-analysis suggest that SCIT may be slightly more effective than SLIT; however, there is a paucity of head-to-head evidence. Similarly, no studies have directly compared the efficacy of drops and tablets in SLIT, and most comparison data have been drawn from large meta-analyses. In addition, the standardisation of allergen immunotherapy is complex, with descriptions of biological potency varying across manufacturers and products. Consequently, different products and routes of administration are not always directly comparable.
Factors that may influence the choice of AIT
Allergen sensitisation and availability of relevant allergen product
Choice of treatment should initially be dictated by the range of allergens to which an individual is sensitised and determination of the most clinically relevant allergens. SCIT offers the widest range of clinically relevant allergens available within Australia (Table). Reflecting the geographical variations in clinically relevant allergens and the fact that product research and design have largely been targeted at European populations, SLIT tablets do not yet cover key southern-hemisphere allergens such as subtropical grasses (including Bermuda, Bahia and Johnson grasses) or animal danders.
Regulatory approval of products
AIT products currently included on the Australian Register of Therapeutic Goods include SLIT tablets for house dust mite (Dermatophagoides farinae/D. pteronyssinus mix), mixed temperate grasses and Timothy grass (Phleum pratense), and also SCIT suspensions for various allergens, both single and mixed. All other AIT products can be prescribed only by clinicians granted authorised prescriber status by the TGA.
Cost
The PBS does not currently subsidise any of the available nonasthma allergy pharmaceuticals, including symptom-relief therapies and AIT. The total cost of AIT varies according to product and can range from about $750 to as much as $4000 for three years of therapy, depending on the allergens, administration protocol and route of administration. Although AIT is clearly more effective than standard care, this cost can present a significant burden for patients. There is some conflicting evidence regarding AIT’s cost-effectiveness in the long term compared with pharmacotherapy, and little direct evidence from Australia. International data suggest that AIT can be cost-effective in the longer term, particularly in patients with comorbid asthma.14,15
Convenience of administration
As there is a small but clinically significant risk of a systemic adverse reaction (such as anaphylaxis or acute asthma) with each dose of SCIT, all injections must be administered in a medical facility equipped to handle such an event. In addition, patients must remain under observation for at least 30 minutes after each injection. This can be impractical, particularly during the weekly updosing phase of the protocol (which can last for three weeks to three months).
In contrast, although the first dose of SLIT should be administered under the supervision of the prescribing clinician, all subsequent doses can be self-managed at home. As a result, many patients and clinicians view SLIT as the more convenient option.
If both SLIT and SCIT are available for the relevant allergen, the route of administration should be chosen in close consultation with the patient. The importance of involving patients in product choice is highlighted by the high frequency of noncompliance with AIT, with 22 to 93% of patients ceasing SLIT and 11 to 77% ceasing SCIT over a three-year course of therapy.16 Noncompliance with SCIT is largely due to inconvenience and side effects, whereas for SLIT cessation of therapy is more likely to result from laxity of self-administration and its significantly greater short-term cost.
Risk of adverse effects
Local adverse effects from AIT are common. Up to three in four patients receiving SLIT experience itching and swelling of the lips and oral cavity and about 80% of those receiving SCIT report swelling at the injection site.6,8 Premedication with antihistamines may attenuate these reactions. Adverse reactions to SLIT peak during the initial 10 to 14 days of therapy and are usually self-limiting. Fewer than 5% of patients discontinue SLIT because of adverse reactions.17 Dose adjustment may be necessary for those with large local reactions to SCIT.18
The risk of systemic adverse effects with SLIT is lower than with SCIT, with an average of 0.056% systemic allergic reactions per SLIT dose, compared with 0.1 to 0.2% for SCIT, and severe systemic reactions occur in about one per million injections.8,19 To date, no fatalities have been reported with SLIT use, and only a single fatality was reported with SCIT use between 2008 and 2012.19 AIT is a safe and well-tolerated treatment.
Risk factors for severe systemic effects with SCIT include poorly controlled asthma and administration of pollen SCIT at the height of pollen season.8 Severe adverse reactions with SLIT are generally not related to poorly controlled asthma.
Special considerations
Asthma
AIT is generally contraindicated in patients with poorly controlled asthma (defined as a forced expiratory volume in 1 second [FEV1] of less than 70% predicted) as the risk of severe systemic adverse effects is considered unacceptably high, particularly for SCIT. However, individuals with a history of asthma that is under good but incomplete control may receive SCIT safely provided their asthma is closely monitored throughout the duration of therapy. This cohort should undergo respiratory function testing before treatment initiation, have their asthma control assessed before every injection and be observed for at least 30 minutes after every injection under the supervision of a physician competent in anaphylaxis management. Because SLIT has a lower rate of systemic adverse effects than SCIT, some groups recommend sublingual over subcutaneous therapy if asthma control is a concern. SLIT has demonstrated better safety profiles in patients with asthma; however, it remains prudent to assess asthma control (e.g. FEV1 >70% predicted) before commencement to reduce the risk of adverse events.
Children
The vast majority of AIT trials to date have focused on adults. However, the volume of literature on AIT use in children is increasing, with tolerability and effectiveness demonstrated in children as young as 3 years of age.8
Pregnancy
Owing to the potential for systemic allergic reactions with immunotherapy, AIT should not be initiated during pregnancy. However, if a patient becomes pregnant while stable on the maintenance phase of AIT, therapy may be continued.20
Medications
It is recommended that beta blockers (all forms including oral and eye drops), ACE inhibitors and angiotensin II receptor blockers are withheld for 24 hours before AIT, as these agents increase the risk of a poor outcome in the event of anaphylaxis. If temporary cessation of these medications is of concern (for example, in patients with poorly controlled atrial fibrillation), then the risk-benefit balance must be carefully evaluated on a case-by-case basis.
Autoimmune disease
It has been postulated that patients with autoimmune disease may have aberrant responses to AIT as a result of immune dysregulation. Data in this area are lacking, but most guidelines agree that active or refractory autoimmune disease is an absolute contraindication to commencing AIT. In patients with well-controlled autoimmune disease, the decision to trial immunotherapy should be made on a case-by-case basis, with careful consideration of the potential risks and benefits.
Missed doses or management of acute illness
AIT should be deferred in the event of acute illness, particularly if there are concerns regarding asthma stability. With SLIT, up to seven doses can be missed without increasing the risk of side effects. When patients are on maintenance therapy, SCIT doses can be spaced up to six weeks apart before dose reduction needs to be considered. Specialist advice should be sought in the event of patients missing more than the above doses.
Conclusion
ARC is a leading cause of noncommunicable disease in Australia and carries significant psychosocial morbidity and financial burden, both individually and at a community level. It is well established that AIT is a safe and effective treatment option for patients in whom conventional pharmacotherapy is insufficient. There is also an increasing body of evidence that the judicious use of AIT can prevent or delay the development of asthma, as well as improve the control of allergic asthma in certain cohorts. The modality of AIT and the specific allergen should be selected after thorough specialist assessment, according to the individual patient’s clinical features, pattern of allergen sensitisation and personal preference for therapy. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.