The red eye – a practical management approach

Many of the common causes of red eye can be recognised and treated in primary care using a diagnostic framework that includes a few key questions and assessments. However, decisive referral for specialist ophthalmology assessment and treatment may be required.
Eye conditions are a relatively common presentation in Australian general practice, comprising 2% of all patient encounters.1 Of the eye conditions seen by general practitioners, most can present as ‘red eye’.2,3 The causes of red eye are many and range from acute to chronic, and self-limiting to sight-threatening. Most GPs have access to an ophthalmoscope, topical fluorescein and local anaesthetic drops to help with examination and diagnosis in patients with a red eye. This article aims to provide a simple diagnostic framework that helps GPs conceptualise the causes of red eye. The use of algorithms has been shown to improve diagnostic accuracy among primary care clinicians in patients with red eye.4,5 This diagnostic algorithm starts by considering whether the condition is bilateral or unilateral.
Bilateral red eye
Five simple questions combined with examination can help to differentiate between common causes of bilateral red eye.
- Did the symptoms start in one eye?
- Are the eyes itchy?
- Is there significant discharge?
- Are the symptoms worse later in the day?
- Are the symptoms worse in the morning?
Symptoms starting in one eye: viral conjunctivitis
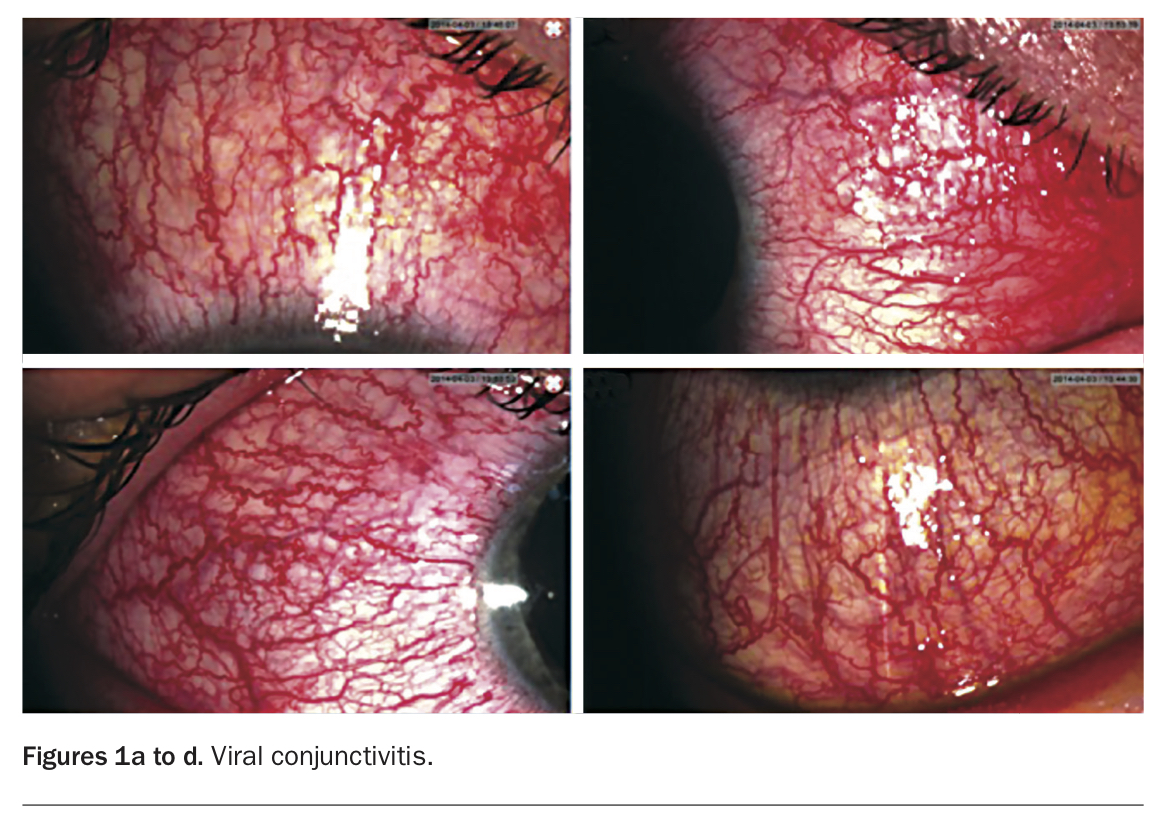
Viral conjunctivitis typically starts in one eye and involves the fellow eye a few days later. There is often an associated upper respiratory tract infection, and sometimes lymphadenopathy (preauricular or submandibular node). There is often a history of contact with an infected person. Most cases are self-limiting and can be managed with preservative-free eye lubricants and cool compresses for comfort, and careful personal hygiene. Viral conjunctivitis is highly contagious and the risk of transmission to others, including family and, in particular, contacts in childcare and school settings, must be discussed. General practice staff should also be aware of the contagious nature of the disease. Referral for specialist ophthalmology assessment is indicated for patients who have lost vision or have severe ongoing conjunctivitis (Figures 1a to d).
{kind=link}
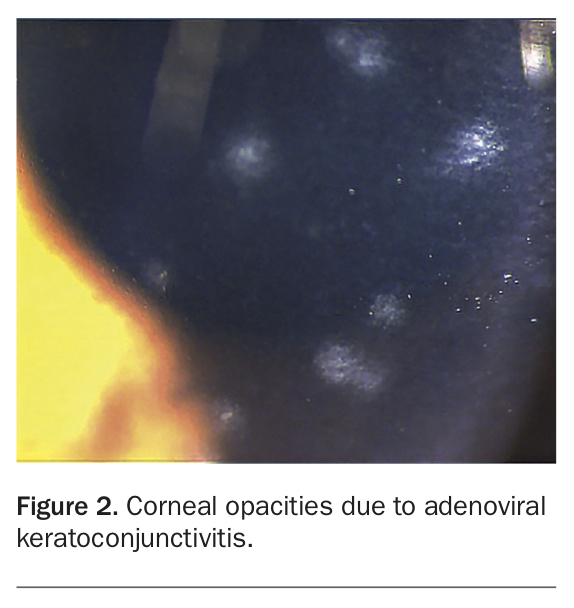
Adenoviral conjunctivitis can present with more severe inflammation, resulting in chemosis and pseudomembrane formation on the tarsal conjunctiva (internal surface of the eyelids). It can also progress to cause corneal opacities (Figure 2) and scarring of the conjunctiva.6 Topical corticosteroids may be used to treat adenoviral conjunctivitis; however, it is usually recommended they be avoided until after a slit lamp examination or until otherwise advised by an ophthalmologist. The main concerns with topical corticosteroid use include iatrogenic harm from worsening of an undiagnosed herpetic or fungal infection and development of corticosteroid-induced glaucoma.
{kind=link}
Itchy eyes: allergic conjunctivitis
Allergic conjunctivitis typically involves bilateral itchy eyes. It often occurs in patients with a known atopic background who may tend to rub their eyes. Quite often, symptoms are seasonal, with symptoms worsening in spring and summer. Everting the upper eyelid of a patient with allergic conjunctivitis often reveals bilateral papillae (small round inflammatory nodules; Figures 3a to d).
{kind=link}
Treatment with topical dual-action antihistamine/mast cell stabiliser (e.g. ketotifen or olopatadine, one drop both eyes, twice daily) and preservative-free eye lubricants, starting two weeks before allergy season, is adequate for many patients.7,8 If the symptoms are poorly controlled, patients may need topical corticosteroids or another adjunctive therapy such as topical ciclosporin (off-label use).9 In patients with severe and persistent symptoms, desensitisation therapy may be warranted.
Significant discharge: bacterial conjunctivitis
If there is significant bilateral discharge that is not hyperpurulent in character, the likely diagnosis is a bacterial conjunctivitis. In most patients, the condition will resolve without pharmacological treatment, and sight-threatening complications are uncommon.10,11 In routine primary care, use of topical antibiotics is unnecessary and is best avoided in uncomplicated bacterial conjunctivitis.12,13 However, if the patient has had a previous trabeculectomy, the infection can spread through the conjunctiva and scleral flap to involve the globe (endophthalmitis). Endophthalmitis is a sight-threatening complication and the patient can go blind within hours. It requires urgent ophthalmologist review and usually a vitreous tap and intravitreal injection of antibiotics, and sometimes urgent surgery. Patients with conjunctivitis who have had a previous trabeculectomy should be referred to an ophthalmologist for assessement.
Chlamydial conjunctivitis can cause a persistent, chronic stringy mucoid discharge that may partially respond to various treatments such as topical chloramphenicol or topical corticosteroids. For a persistent conjunctivitis, consider taking a conjunctival swab for chlamydia polymerase chain reaction (PCR) testing. Chlamydial infection responds to treatment with oral azithromycin.
Symptoms are worse later in the day: dry eye syndrome
Dry eye syndrome is a common ocular condition, and symptoms are often worse in the evening. Paradoxically, patients often present with watery eyes owing to increased tear production, caused by irritation, and poor-quality tears that do not adhere to the surface of the eye. Symptoms are typically worse in wind and airconditioning, and with prolonged reading or computer work.
Some patients find relief with frequent use of lubricants, and ointments or gels at night. Preservative-free lubricants are preferable, particularly for regular use. The treatment goal is to reduce the symptoms to a manageable level while keeping the intervention burden low. Moderate to severe forms of this disease can have a major impact on quality of life. Systemic medications (commonly beta blockers and diuretics, although including a broad range of medications) can exacerbate this condition. Newer therapies including topical ciclosporin or lifitegrast may be beneficial for patients living with stubborn and persistent symptoms, so consultation with an ocular surface/cornea subspecialist could be considered.14-17
Symptoms are worse in the morning: blepharitis
Blepharitis is a prevalent, underdiagnosed chronic condition that is often present in patients with dry eye syndrome.18 Blepharitis symptoms include grittiness, irritation and ocular discomfort. Symptoms are often worse in the morning. Left untreated, blepharitis can be a reason for poor response to other dry eye interventions. Two subtypes (anterior and posterior) are described. Posterior blepharitis is associated with rosacea and with development of chalazia (meibomian cysts) when poorly controlled. Anterior blepharitis is associated with a dandruff-type material at the base of the lashes.
Treatment for blepharitis involves lid hygiene (heat, massage and lid scrubs) once or twice daily and lubricants. Although there is no cure, the condition can be alleviated with a combination of advanced dry eye treatments, systemic doxycycline and potentially by interventions such as thermal pulsation or intense pulsed light therapy.19,20
Unilateral red eye
Patient history and specific ocular signs are useful in determining the cause of unilateral red eye. The specific site involved is key to correct diagnosis.
Trauma
Corneal abrasions are common after ocular trauma and it is important for the GP to assess for a more serious injury. Assessment includes the following:
- visual acuity testing
- visual fields to confrontation testing
- full pupil assessment including reaction to light, reaction to accommodation and checking for a relative afferent pupil defect
- ocular motility testing
- checking for red reflex
- checking for a hyphaema (a fluid level of red cells in the anterior chamber that indicates significant intraocular trauma)
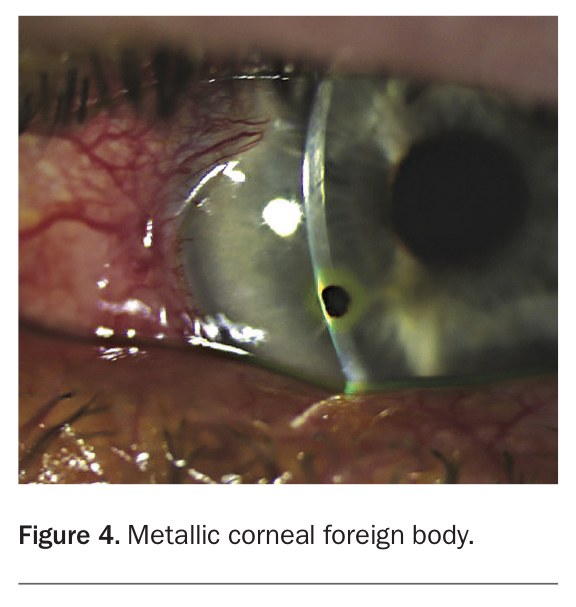
- checking for a foreign body (Figure 4)
- palpating the orbital rim for a fracture
- a Seidel test, which when positive indicates a penetrating eye injury.21,22 The test is positive when aqueous leaks through a wound and pushes fluorescein out of the way (like a waterfall), observed with the blue filter. Most direct ophthalmoscopes have a cobalt blue filter for this purpose; the red-free filter is a green filter which is used to view blood vessels, not fluorescein.
{kind=link}
Herpes simplex virus keratitis
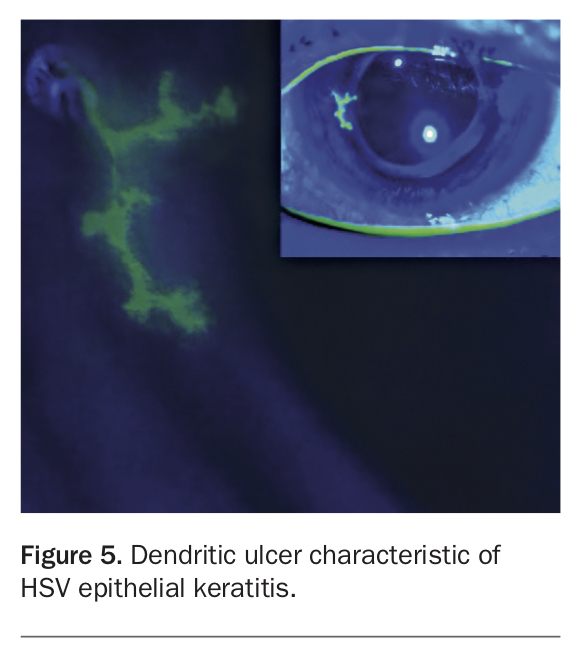
Autopsy studies on the trigeminal ganglia show that more than 90% of the population are infected with latent herpes simplex virus-1 (HSV-1) by the age of 60 years. The mean age of first occurrence of ocular herpes is 37 years.23 The annual incidence of ocular HSV keratitis is 12 people per 100,000 and about 40% of those will experience a recurrence.24 A typical recurrence of HSV keratitis causes a mild foreign-body sensation, which progressively worsens with associated increasing redness and light sensitivity. The classical clinical finding is a ‘dendritic’ (branching) ulcer, but this is not universally the case. This is seen with fluorescein dye, which stains areas where the epithelium is not intact, under a blue light. If a dendritic ulcer is visible, HSV epithelial keratitis is the likely diagnosis (Figure 5). Taking a swab of the lesion for PCR testing can be useful, although false negative results can occur with a small lesion.
{kind=link}
Aciclovir 3% ointment five times daily is the standard treatment.25 Specialised ophthalmology assessment needs to be sought for patients who do not respond to treatment, and for those with any corneal opacity, which indicates stromal involvement. HSV uveitis can be associated with HSV keratitis, and typically causes worse photophobia.
Herpes zoster keratitis
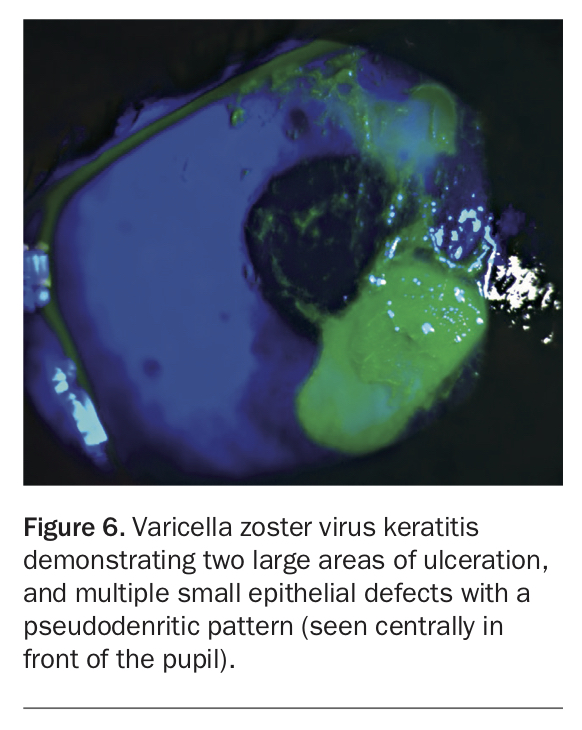
Varicella zoster virus (VZV) can also produce a keratitis without the typical skin lesions in the V1 distribution, although this is atypical. It is often very painful, and there may be a ‘pseudodendritic’ ulcer pattern with fluorescein (Figure 6). VZV can cause inflammation involving any part of the eye or periocular tissue.
{kind=link}
Management of herpes zoster keratitis is with valaciclovir 1 g orally three times daily for at least seven days, and typically the patient will require topical corticosteroids, which in some cases will need gradual tapering over months. Valaciclovir can rarely precipitate acute kidney injury, and hence should be used cautiously when the patient is at risk of dehydration, especially with concomitant use of other potentially nephrotoxic medicines such as NSAIDs and antihypertensives.26
Acute anterior uveitis
Acute anterior uveitis (AAU) is the most common form of uveitis, with an annual incidence of 15 to 20 per 100,000.27 As delayed treatment can result in permanent loss of vision, distinguishing AAU from the much more common presentations of conjunctivitis is vital.
AAU typically starts with an initially mild and progressively worsening light sensitivity, and redness in one eye. Pain can become severe as the disease progresses. This is particularly notable for objects of near regard, such as when reading, and is a key symptom for the GP to ask about. Blurred vision is common in the affected eye. Conjunctival inflammation may be predominantly around the limbus (circumciliary), but it may also be diffuse. A watery eye is common, but ocular discharge is not expected in AAU. Photophobia is typically moderate to severe when the patient presents.
It is uncommon but possible to have bilateral AAU. The pupil of an affected eye is likely to be constricted and may be ‘stuck down’ to the lens (posterior synechiae). Consensual photophobia is a useful clinical sign, which may be diagnostic. When a light is shone in the fellow eye, both pupils constrict, and in an eye with iritis (anterior uveitis) the pupillary constriction causes pain. This is often a much more reliable finding than looking for white cells with the slit lamp. If the episode is severe or prolonged, a hypopyon may develop (a fluid level of white cells in the anterior chamber).
There are many potential systemic associations of AAU, including HLA-B27-associated diseases such as ankylosing spondylitis, tuberculosis, syphilis, sarcoidosis and Behcet’s disease. These may provide historical clues to the diagnosis in the clinical assessment in primary care. All cases of AAU should be seen promptly by an ophthalmologist, and it is best to speak with the specialist to avoid any likelihood of delayed examination.
Typically, treatment will involve intensive use of topical corticosteroid drops (prednisolone or dexamethasone hourly) and dilating drops (homatropine three times daily, which is now largely unavailable; alternatives are atropine 1% once or twice daily or cyclopentolate 1% three times daily). Usually patients will be investigated for an underlying cause. Some causes are low probability (e.g. tuberculosis and syphilis) but important to rule out.
Episcleritis
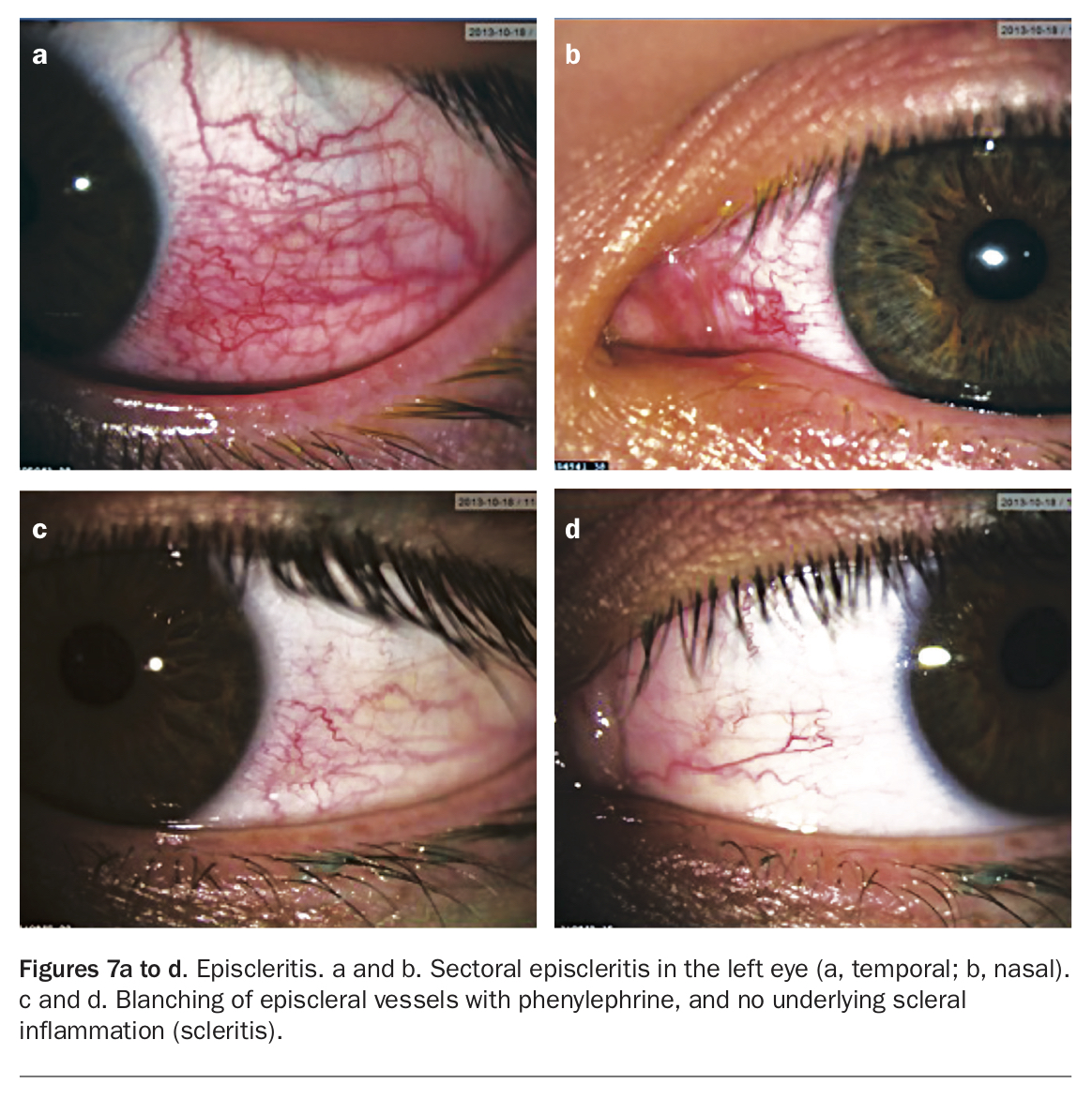
Episcleritis is a relatively common presentation in young patients. The episcleral tissue involved is deep to the conjunctiva and superficial to the sclera (hard collagenous shell of the eye). Episcleritis is generally not very painful or tender, and usually does not affect vision, which differentiates it from scleritis (see below). Using topical phenylephrine 2.5% drops can help distinguish episcleritis from scleritis; phenylephrine constricts the more superficial vessels, and in episcleritis, the uninflamed sclera is seen below it (Figures 7a to d). In most cases of episcleritis, it is not productive to investigate for an associated autoimmune condition, unless it is recurrent. Treatment is usually with topical or oral NSAIDs, or topical corticosteroids.
{kind=link}
Scleritis
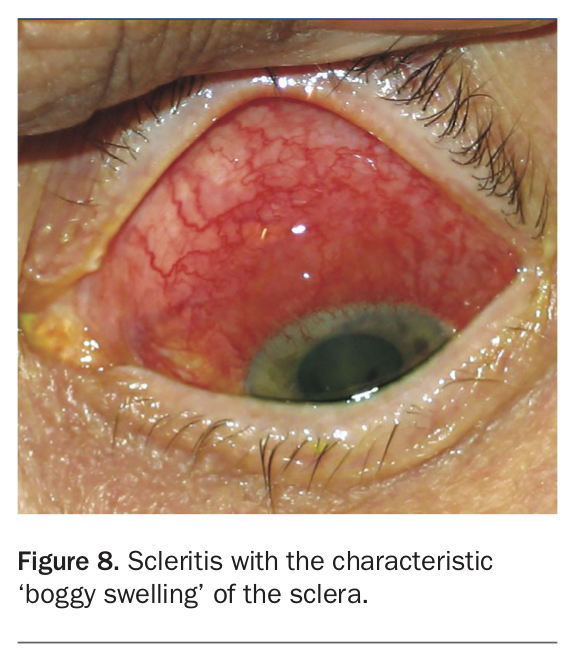
Scleritis causes severe pain (a deep boring pain at night) and is often exquisitely tender. Scleritis is both a sight and life-threatening emergency, as there is usually an underlying autoimmune condition; an episode of scleritis indicates that control of that disease is suboptimal. The sclera often looks boggy (Figure 8). Using topical phenylephrine in this situation will not cause blanching or constriction of the involved vessels. This condition usually requires urgent review by an ophthalmologist and rheumatologist/immunologist. Patients will typically require systemic immunosuppression to control the disease.
{kind=link}
Pterygium
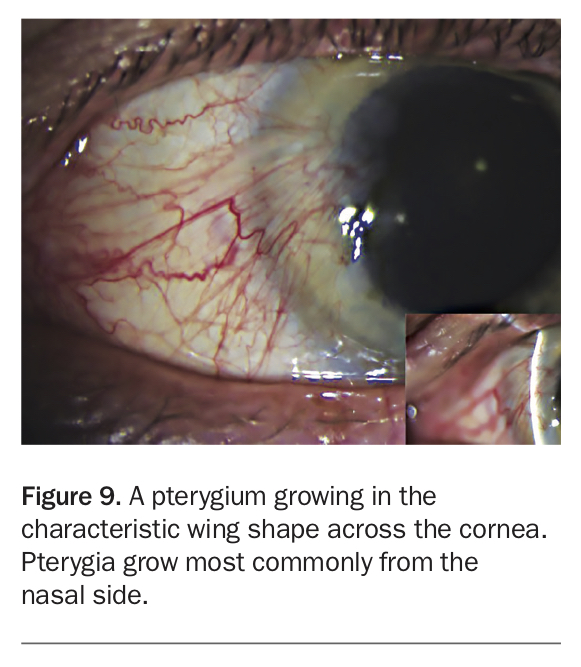
Pterygia appear as a characteristic wing-shaped growth across the cornea (Figure 9). It is a common ocular condition in Australia, due to our outdoor lifestyle and the fact that many people do not wear UV (ultraviolet) lightblocking spectacles with good side protection. UV damage accumulates from childhood and therefore it is important that children wear good UV protection for their eyes. Most sunglasses do not provide protection from UV light from the sides, and hence many sunglasses can give patients false reassurance about being appropriately protected. When exposed to UV, pterygia become inflamed, which promotes further growth. It is important to recognise that UV exposure is also a risk factor for ocular surface squamous neoplasia and eyelid BCC, SCC and melanoma. Pterygia often respond to topical medical therapy initially, but if sight is affected and inflammation persists then surgery should be considered.
{kind=link}
Urgent conditions
Red eye is also a symptom of four sight-threatening diagnoses that should not be missed, and which require urgent referral to an ophthalmologist and treatment. It is important to ask or note the following four things:
- Does the patient have a severe headache?
- Does the patient wear contact lenses?
- Is there a purulent discharge?
- Has the patient recently undergone eye surgery?
Severe headache: acute angle closure
Along with red eye, the four major features of acute angle closure (formerly called acute glaucoma) are progressively worsening severe eye pain, which can become a generalised headache, blurred vision, seeing haloes around lights and gastrointestinal symptoms (nausea and vomiting). Elevated intraocular pressure (IOP) can result in the eyeball feeling firm when balloted through the upper eyelid, compared with the fellow eye, and can cause corneal oedema. Corneal oedema produces blurred, foggy vision and haloes around lights. The pupil is often fixed and mid-dilated due to iris ischaemia. It is more likely to happen in older, long-sighted people who have not had cataract surgery (the natural lens is significantly thicker at 4 to 5 mm than artificial lenses at around 1 mm). It can be precipitated by a range of medications including sympathomimetics (e.g. salbutamol, phenylephrine), anticholinergics (e.g. amitriptyline, citalopram, atropine) and other drugs (e.g. 3,4-methylenedioxymethamphetamine [MDMA/ecstasy], acetazolamide, topiramate).
GPs should telephone an ophthalmologist about initiating treatment; sometimes sending the patient immediately to a specialist speeds up treatment. Urgent treatment usually involves rapidly acting IOP-lowering drops such as brimonidine or combination timolol/brimonidine, pilocarpine 2% drops (which can help relieve angle closure by constricting the pupil and opening the angle, but repeated use can increase pupil block) and oral or intravenous acetazolamide. Timolol is a nonselective beta-blocker and is contraindicated in patients with chronic airways limitation and bradyarrhythmias. Laser peripheral iridotomies or cataract surgery are the definitive treatments for preventing another episode of angle closure.
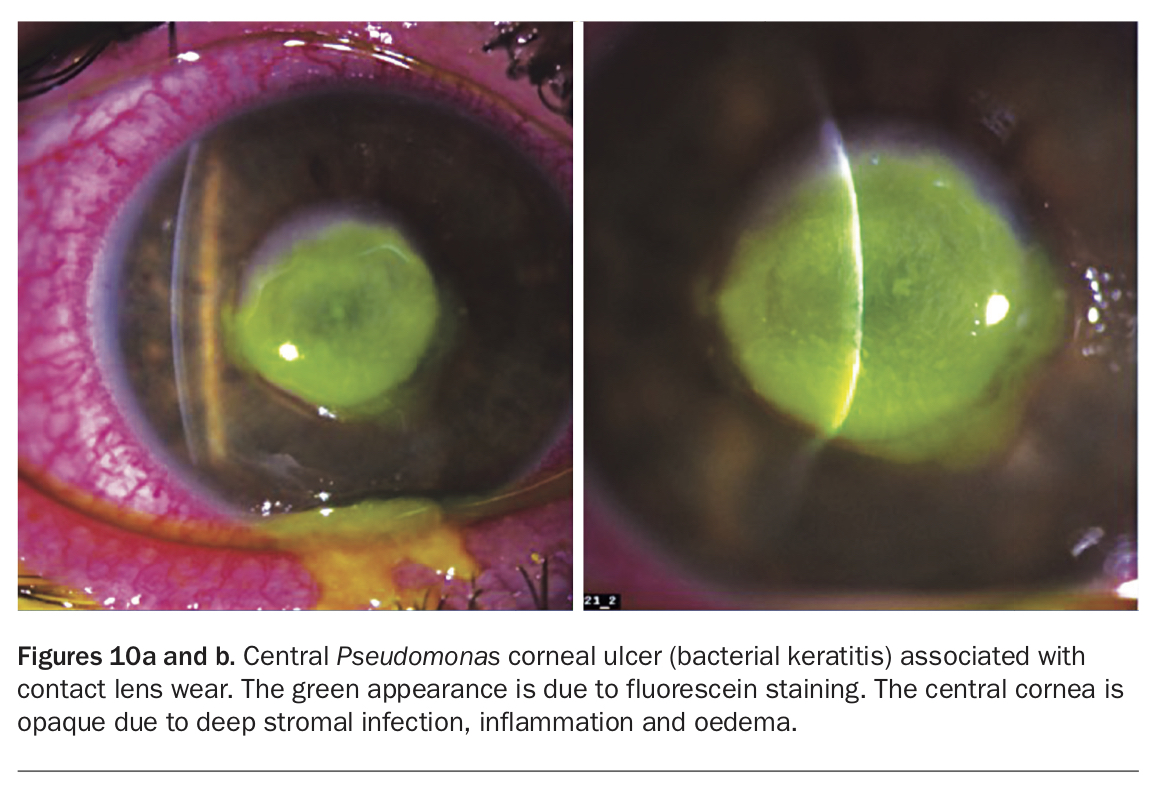
Contact lenses: contact lens-associated keratitis
Any contact lens wearers presenting with a red eye should be presumed to have a contact lens-associated corneal infection (keratitis), until proven otherwise. They should be referred for prompt examination. If there is a focal opacity, it will often be scraped for microbiological testing before starting antibiotics. Pseudomonas aeruginosa is the most common causative agent and infection can progress rapidly (Figures 10a and b). Infection with other organisms such as Acanthamoeba species and fungi are less common but difficult to eradicate, especially if definitive treatment is delayed, for example, due to a trial of topical chloramphenicol. GPs can play an important preventive role through patient education about contact lens hygiene, which is understandably suboptimal for many people. Patients should be advised not to sleep, swim or shower while wearing their contact lenses, and not to extend the duration of contact lens use beyond the disposal date.
{kind=link}
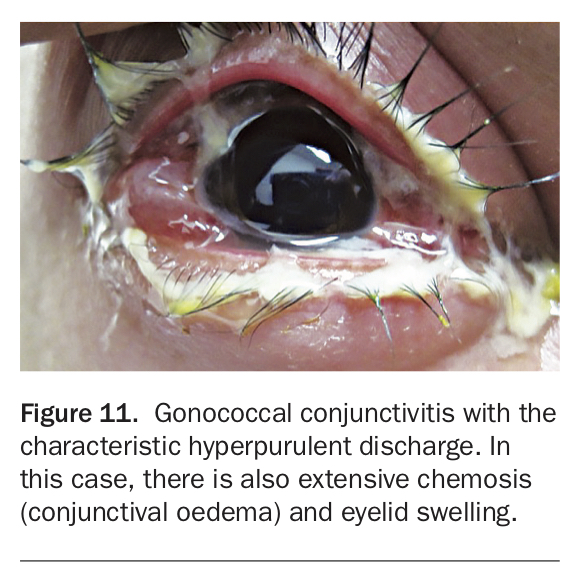
Purulent discharge: gonococcal conjunctivitis
Gonococcal conjunctivitis produces a copious hyperpurulent discharge, which quickly reaccumulates (Figure 11). The infection can progress to involve the cornea, leading to corneal melt, perforation and loss of the eye. Typically, there is a sexual contact history, and the patient may have an associated genital infection and other sexually transmitted infections.28 Bathing the eyes in urine is an alternative health practice that significantly increases risk.29 This condition requires hospital admission for intravenous antibiotic and intensive topical antibiotic therapy. Delay to definitive treatment due to trialling topical chloramphenicol can result in worsened patient outcomes.
{kind=link}
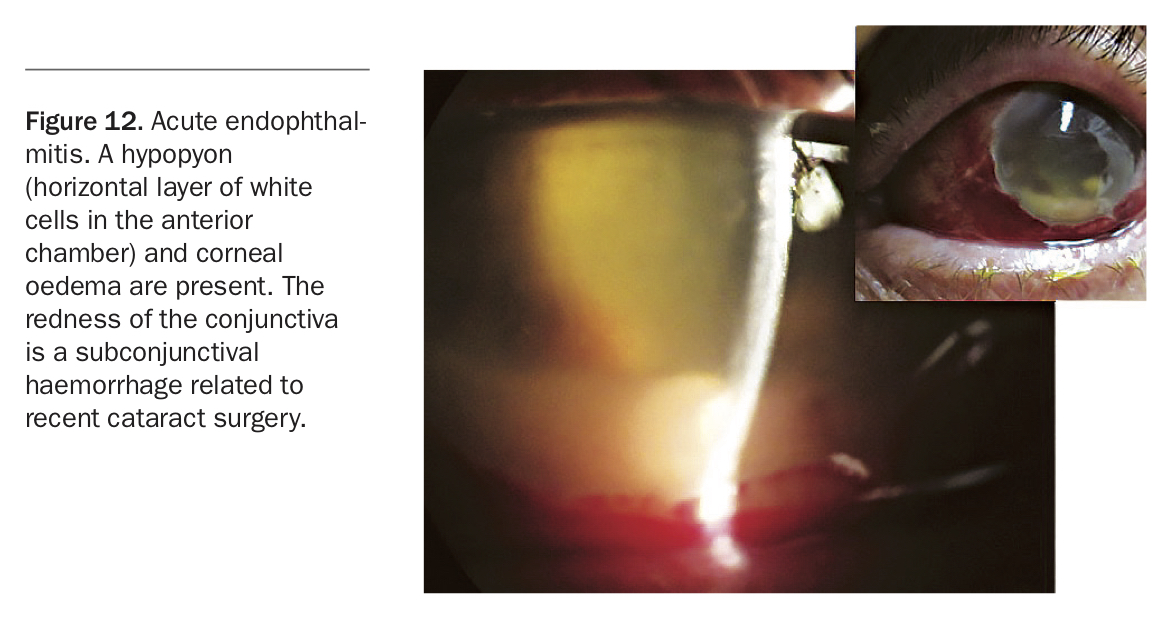
Recent eye surgery or injection: endophthalmitis
Recent eye surgery such as cataract surgery or intravitreal injection (for age-related macular degeneration or diabetic macular oedema) carries a small but real risk (less than one in 1000 chance) of infection. Infection is most likely to occur within two weeks of a procedure. This presents as a red eye with increasing pain and photophobia, and there may be a hypopyon (a fluid level of white cells in the anterior chamber) (Figure 12). Vision is typically poor, often at the level of counting fingers or hand movements only, unless the patient presents early. As above, a patient with a previous trabeculectomy is at risk of endophthalmitis if they have bacterial conjunctivitis. Any patient with suspected endophthalmitis must be urgently seen by an ophthalmologist. Treatment involves a vitreous tap (for microbiological testing) and intravitreal injection of antibiotics.
{kind=link}
Conclusion
A basic algorithm such as the one suggested here provides a simple approach to diagnosing the cause of red eye. Some useful general resources for GPs are noted in the Box. Advice from an ophthalmologist should be sought at any time if you are concerned about a patient, with referral being urgent if a sight-threatening emergency is suspected. MT
{kind=link}