Idiopathic hypersomnia: more than usual sleepiness

Idiopathic hypersomnia presents with extreme daytime sleepiness, despite a longer than average duration of nocturnal sleep. Patients frequently sleep through life, can have long diagnostic delays and frequently face social stigma. Accurate diagnosis and treatment, including lifestyle modifications and pharmacological therapies, will help alleviate symptoms and improve quality of life.
- Idiopathic hypersomnia (IH) is characterised by an excessive need for sleep, persistent sleepiness when awake, unrefreshing sleep and naps and sleep inertia on waking.
- Patients may be young to middle aged, with impairment in day-to-day functioning that has often been present for years and attributed to other factors such as lifestyle or comorbidities.
- Patients reporting symptoms of IH in whom other causes cannot be identified should be referred for sleep physician assessment.
- Open-access ambulatory sleep studies are best validated for diagnosing obstructive sleep apnoea (OSA) in individuals assessed to be at high risk of moderate to severe OSA and may be normal in patients with IH.
- Medical therapy to improve vigilance and wakefulness for patients with diagnosed IH leads to improvements in symptoms, distress and quality of life.
Sleep is a universal human need and we can all relate to the tiredness that ensues when sleep is insufficient in time or quality. For most people, sleepiness is a transient state relieved by adequate sleep, and although many people report feelings of sleepiness, those in whom sufficient sleep does not resolve sleepiness will report to their GP for further investigation.1,2 These individuals describe challenges in functioning in their day-to-day life and work, and such patients are owed an explanation for their symptoms. Common causes of sleepiness include insufficient sleep through shift work or through conditions that reduce sleep quality, such as obstructive sleep apnoea. In patients without these explanations, some will have a central disorder of hypersomnolence, such as narcolepsy or idiopathic hypersomnia (IH).2 Narcolepsy is a familiar term to many and is often misused to describe all forms of sleepiness. Although less common than IH, many health professionals (and the public) are more familiar with narcolepsy. This article outlines an approach to diagnostic investigations, differential diagnoses and treatment options available for patients with sleepiness that is not relieved by adequate sleep.
What is idiopathic hypersomnia (IH)?
Idiopathic hypersomnia is defined as excessive daytime sleepiness (EDS; periods of the irrepressible need to sleep) and an excessive need to sleep (ENS; more than 10 hours of sleep in 24 hours) for at least three months which are not accounted for by other conditions.3,4 A diagnosis of IH is supported by laboratory-based sleep studies that exclude other sleep disorders such as sleep apnoea.4 Some patients experience repeated, rapid onset of sleep during a multiple sleep latency test, which measures EDS, whereas others may predominantly have symptoms of ENS, which are better quantified with sleep diaries or objective measures of sleep over days or weeks, such as actigraphy.4
Patients with IH often describe common symptoms, including sleep inertia on waking, when it is difficult to wake up, that can lead to compensatory rituals of using multiple alarm clocks and other special processes to get up. Once awake and out of bed, the day is characterised by persistent sleepiness, resulting in functional impairment that many patients label as ‘brain fog’.5 Patients may take regular daytime naps (scheduled and unscheduled), describing sleep as unrefreshing.
Patients with symptoms of hypersomnolence (i.e. EDS) are often subject to diagnostic delay.6 IH has a profound impact on patients’ lives, with patients reporting difficulty in keeping up with peers during their teenage years and maintaining employment and relationships in adulthood. Patients with IH also experience stigma and unfavourable presumptions.7 A first-hand account from a patient living with IH is outlined in the Box.
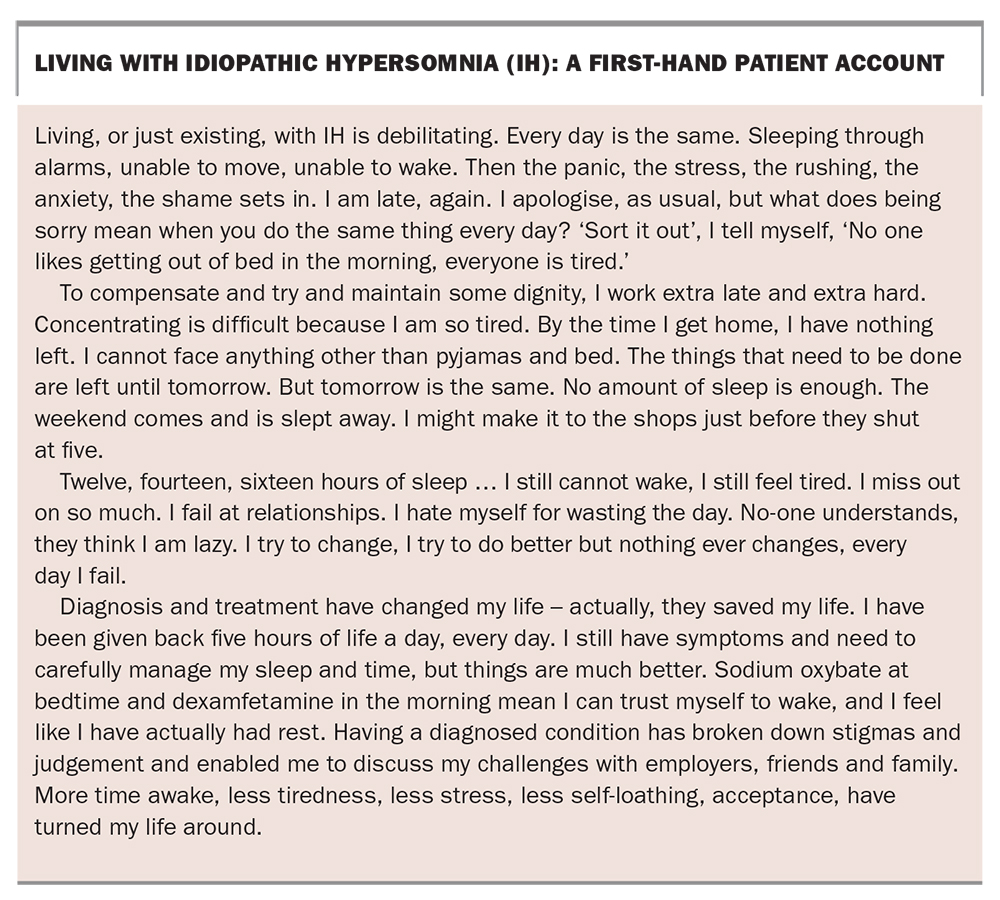{kind=link}
How does IH differ from narcolepsy?
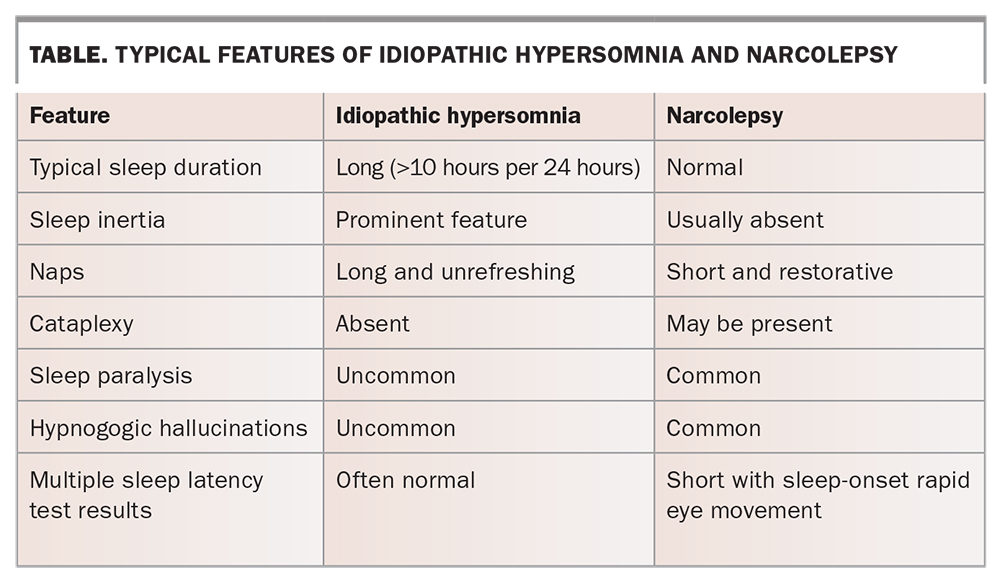
Narcolepsy is a rare neurological condition that presents with hypersomnolence, with additional features of cataplexy, hallucinations occurring at sleep onset or waking and sleep paralysis.3 The hallmark of narcolepsy is sleep-onset REM seen during laboratory-based diagnostic sleep studies. Some patients with narcolepsy describe additional symptoms of cataplexy, which is a sudden loss of muscle tone in the body triggered by strong emotion resulting in transient short periods of muscle weakness. People with narcolepsy often share the symptoms of EDS with those who have IH, but do not have symptoms of ENS and usually sleep for eight hours or less per 24 hours. They also do not have the same symptoms of sleep inertia and find naps refreshing (Table).3,4
{kind=link}
Differential diagnoses
Another diagnosis to consider is myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), which can have similar degrees of sleepiness as IH with additional post-exertional malaise, myalgia and dysautonomia.8 Distinguishing between fatigue and sleepiness can be difficult, as patients may use the words interchangeably. It is helpful to think of sleepiness as the tendency to fall asleep, especially in passive situations (EDS) or for periods of more than 10 hours per 24 hours (ENS), whereas fatigue often reflects a sense of exhaustion, inability to do any more or an overwhelming need to rest without a sense of sleepiness.
Other conditions that should be considered include prodromal autoimmune conditions, diabetes, liver disease, primary adrenal insufficiency and, in patients with exertional symptoms, cardiac failure.9,10 Mental health conditions that alter sleep quality and structure, such as anxiety, depression or post-traumatic stress disorder, can also be associated with hypersomnia.11 Patients who have suffered a head injury are at risk of hypersomnolence.12 The symptoms of idiopathic hypersomnolence can change over time, reflecting the uncertain disease process. As such, spontaneous remission is possible.
Evaluations and tests to diagnose IH
Physical examination and neuroimaging results in patients with IH are typically normal, but a comprehensive assessment to exclude other diagnoses is essential.13 The role of pathology tests in primary care is primarily aimed at excluding conditions that can result in fatigue or sleepiness, such as low iron stores, low haemoglobin level, abnormal thyroid function, chronic inflammatory disorders or malabsorptive syndromes.
Distinguishing between mental illness, ME/CFS and IH is often challenging, and patients should be referred to a specialist sleep physician if factors causing fatigue or somnolence cannot be found, or if symptoms persist despite these factors being addressed. Sleep studies are an important part of investigating IH and narcolepsy; however, open access ambulatory sleep studies alone have low diagnostic yield in patients without a moderate to high pretest probability of obstructive sleep apnoea.14 Hence, sleep physician assessment, followed by laboratory-based sleep tests that directly assess somnolence, are preferable.4,14
Causes of IH
The mechanisms that cause IH are unknown, although many potential neurochemical triggers have been proposed. One research group showed altered gamma-aminobutyric acid receptor modulators in the cerebrospinal fluid of patients with hypersomnolence; however, clinical response to treatments to modify these with flumazenil have been inconsistent.15,16 Furthermore, response to medical treatment for IH is varied, which suggest causes of IH may be varied.17
Treatment for IH
Lifestyle factors are an important consideration in patients with IH. Scheduled naps and pacing can mitigate symptom severity. Cognitive behavioural therapy can empower patients to manage their condition and improve self-efficacy while minimising the adjustment reaction common to the condition.18 Linking patients to support groups such as Hypersomnolence Australia is also an important part of helping them develop a sense of self-efficacy.19
Patients should be warned about the impact of their condition on fatigue-sensitive tasks such as driving. Subjective assessments of the severity of hypersomnolence using the Epworth sleepiness scale should be also be performed.
Pharmacological treatments for hypersomnia aim to improve daytime alertness. Randomised controlled trials support the efficacy of wakefulness-promoting drugs, including modafinil and the longer acting preparation armodafinil.17,20-22 In patients who do not respond to modafinil, use of stimulant-based therapies, such as dexamphetamine or methylphenidate, can be considered.23
Medications such as pitolisant, solriamfetol and sodium oxybate can be helpful in managing EDS but are not yet registered in Australia.22 In a recent clinical trial, sodium oxybate was shown to reduce sleep inertia, total sleep time and daytime sleepiness in people with IH.24 Lack of access to these treatments in Australia (and the cost associated with sourcing them) is problematic for patients with an incomplete response or unacceptable side effects to stimulants or modafinil.23 Other approaches to treatment, including the use of experimental gamma-aminobutyric acid antagonists such as clarithromycin, have a limited evidence base and inconsistent results and should not be used outside of a trial setting.17,25
Conclusion
Idiopathic hypersomnia is characterised by hypersomnolence (i.e. ENS), EDS and symptoms such as sleep inertia and unrefreshing naps. Although these symptoms can occur as part of other physical or mental health disorders, if they persist despite the absence or optimal treatment of these conditions, a diagnosis of IH should be considered. Patients can be referred to a sleep physician for clinical assessment, laboratory-based sleep testing, including a multiple sleep latency test, and long-term sleep monitoring. Support and medical therapy to improve vigilance and wakefulness are available for patients with diagnosed IH, which in most cases leads to improvements in symptoms, distress and quality of life. MT
References
with 153 patients. J Clin Sleep Med 2016; 12: 1389-1394.
J Clin Sleep Med 2020; 16: 2047-2062.