Dexamethasone intravitreal implant for macular oedema and uveitis

Eye diseases
Vision impairment and blindness
Intravitreal injections of corticosteroid have been used to treat ophthalmic conditions such as macular oedema due to diabetic retinopathy or retinal vein occlusion and noninfectious uveitis for many years. An intravitreal implant that releases dexamethasone in a controlled manner over three to four months is now available to treat selected patients with these conditions.
Macular oedema is an accumulation of fluid within the central part of the retina (the macula). This can lead to loss of the normal architecture and function of the macula causing distortion and deterioration of central vision. Macular oedema results from a breakdown in the blood-retinal barrier, with fluid accumulating both interstitially and within the retinal glial cells (Müller cells). It can occur in patients with diabetic retinopathy, retinal vein occlusions or ocular inflammation (uveitis). Macular oedema is diagnosed clinically and monitored with optical coherence tomography (Box 1, Figure 1 and Figure 2).
{kind=link}
{kind=link}
{kind=link}
Intravitreal injections of corticosteroid have been used to treat patients with macular oedema caused by diabetic retinopathy or retinal vein occlusions and noninfectious posterior segment uveitis for many years. In diabetic retinopathy and uveitis, corticosteroids produce an anti-inflammatory effect through various mechanisms, including a decrease in synthesis of inflammatory mediators and vascular endothelial growth factor (VEGF).1 In retinal vein occlusion, their mechanism of action is thought to be upstream of VEGF by suppressing its expression.
However, intraocular corticosteroid treatment can have significant side effects, including elevated intraocular pressure, glaucoma and cataract. For this reason, patients with macular oedema caused by diabetic retinopathy or retinal vein occlusions are now commonly treated with intravitreal anti-VEGF as first-line therapy.
Nevertheless, intravitreal corticosteroids are regarded as second-line treatment for patients who are unresponsive to anti-VEGF therapy. They are also used as second-line therapy in those who have contraindications to anti-VEGF.
Recently, a dexamethasone intravitreal implant was developed that can deliver dexamethasone locally in a slow and sustained manner. This implant has the potential to maximise treatment efficacy and safety and reduce the number of intravitreal injections the patient requires.
What is the dexamethasone implant?
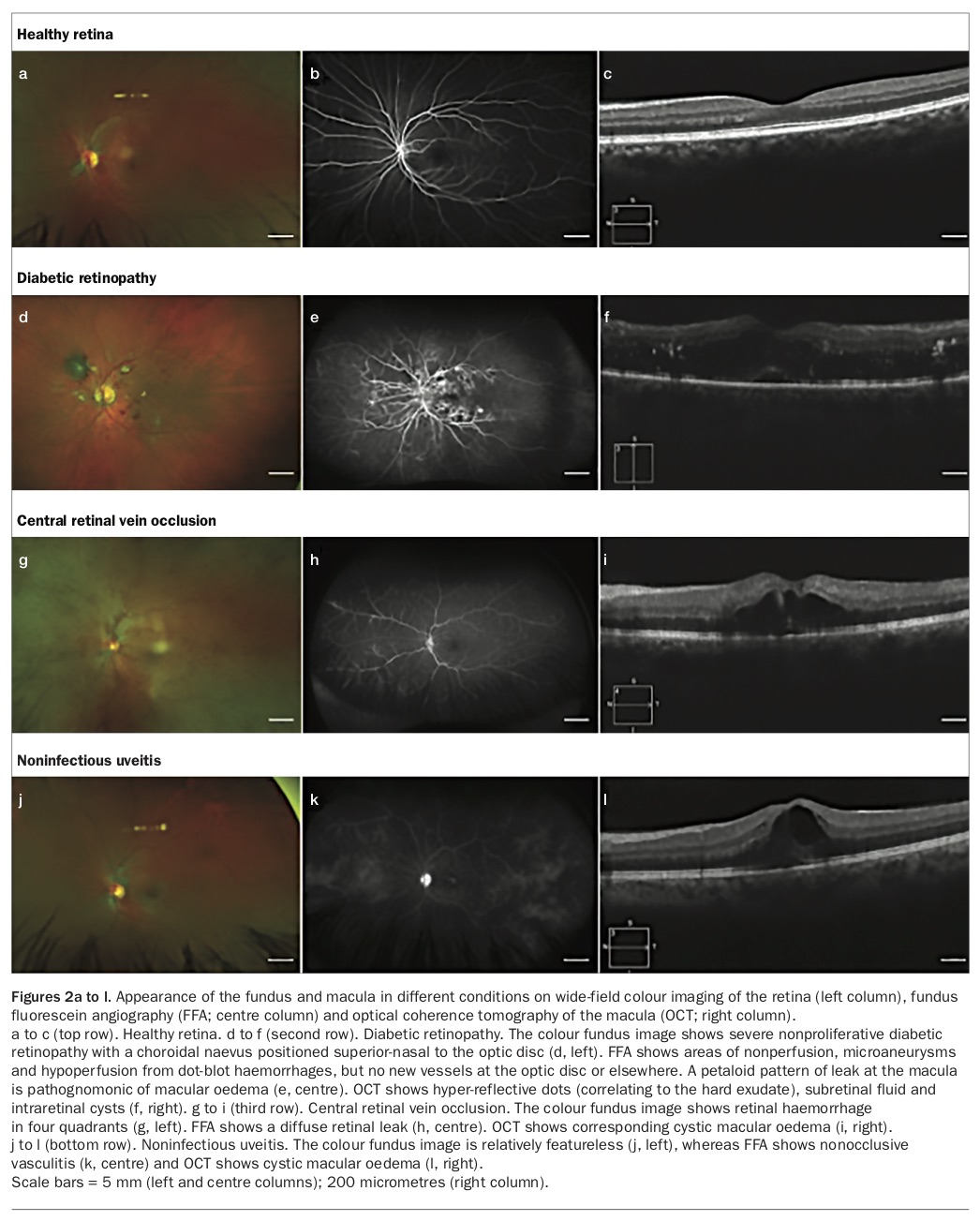
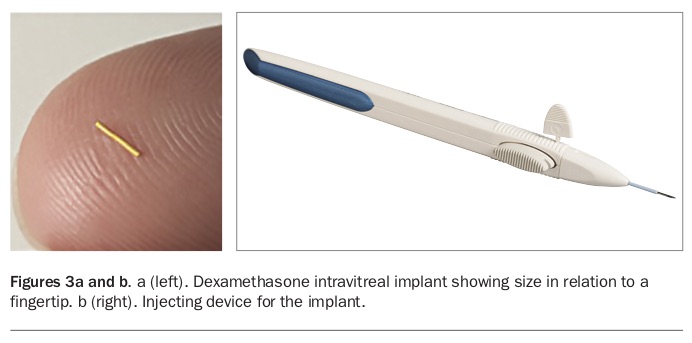
The dexamethasone intravitreal implant is a slow-release biodegradable implant that is placed inside the vitreous of the eye (Figures 3a and b). It contains 700 mcg dexamethasone in a solid polymer drug delivery system. This preservative-free polymer matrix of polyglactin releases dexamethasone in a controlled manner over three to four months.
{kind=link}
When is the dexamethasone implant used?
The dexamethasone implant is TGA approved for the treatment of diabetic macular oedema, macular oedema due to branch retinal vein occlusion or central retinal vein occlusion, and noninfectious uveitis affecting the posterior segment of the eye.
The dexamethasone implant is listed on the PBS for prescription by an ophthalmologist for the treatment of:
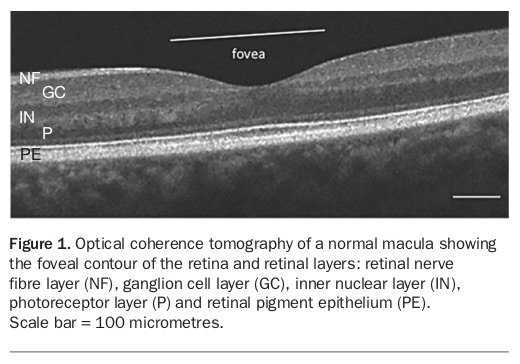
- patients with diabetic macular oedema (Figures 2d, e and f) who have already had cataract surgery or are scheduled to have cataract surgery and have failed to respond to a VEGF inhibitor or where it is unsuitable to use a VEGF inhibitor. Visual acuity must be between 6/9 and 6/48
- patients with macular oedema following branch retinal vein occlusion or central retinal vein occlusion (Figures 2g, h and i) who have failed treatment or have contraindications to VEGF inhibitor treatment. Visual acuity must be between 6/9 and 6/120
- patients with noninfectious posterior segment uveitis with documented visual impairment, defined as best corrected visual acuity score of approximate Snellen equivalent 6/12 or worse, secondary to vitreous haze or macular oedema, and unilateral, asymmetric uveitis or bilateral uveitis where systemic treatment is not clinically indicated (Figures 2j, k and l).
The most potent treatment for non-infectious posterior segment uveitis is a systemic corticosteroid. However, many patients do not tolerate high-dose systemic corticosteroids, and their long-term use results in serious side effects, including diabetes, hypertension and osteoporosis. For this reason, local corticosteroids, including the dexamethasone intravitreal implant, are often used in combination with systemic cortico-steroids to minimise the systemic treatment dose when posterior noninfective uveitis involves only one eye or involves one eye more than the other, with the local corticosteroids used in the worst eye.2
The dexamethasone implant can also be used to treat macular oedema in patients who have contraindications to anti-VEGF, such as pregnant women, and in those who have recently had a stroke or acute coronary syndrome as the safety of intravitreal anti-VEGF treatment in patients at high risk of cardiovascular events is still debated.3
How is the dexamethasone implant used?
The dexamethasone implant is injected into the vitreous cavity of the eye via a stepped incision using a 23-gauge needle on the end of a pen-like applicator (Figure 3b). The implant is introduced under aseptic conditions, with regional anaesthesia with subconjunctival lignocaine. The procedure can be performed in the ophthalmologist’s office or a hospital procedure room. It is not necessary to use an operating theatre for placement of the implant.4
Treatment frequency is less than for intravitreal anti-VEGF treatments. The slow-release drug delivery system exerts a therapeutic effect over three to four months.2,5 Some patients need only a single dexamethasone implant to control macular oedema, but a new implant can be placed if or when required.
Expected outcomes
After insertion of a dexamethasone implant, patients can expect an improvement in vision and corresponding decrease in macular oedema over the next few weeks. The therapeutic effect lasts longer than for anti-VEGF treatments, and most patients do not require repeat dosing for at least three to four months, as described above.
Adverse effects
Adverse effects of the dexamethasone intravitreal implant are summarised in Box 2. Use of corticosteroids, including the dexamethasone implant, in and around the eye can cause raised intraocular pressure, glaucoma and cataract. It will also promote the progression of any active intraocular infection and increase its severity. It is crucial that infective posterior segment uveitis is excluded before regional ocular corticosteroids are used, especially intraocular corticosteroids such as the dexamethasone implant.
{kind=link}
Patients need to be warned about the progression of cataract with intraocular corticosteroids and should undergo screening for elevated intraocular pressure and clinical features of glaucoma before using the dexamethasone implant. A recent prospective study of 40 patients with macular oedema secondary to retinal vein occlusions found that the dexamethasone implant had a better safety profile in regard to cataract progression and requirement for glaucoma treatment compared with intravitreal triamcinolone acetonide.6
The dexamethasone implant is subject to the same warnings regarding intra-vitreal injection as any other intravitreal treatment. Common adverse effects after an intravitreal injection include eye discomfort and subconjunctival haemorrhage.7 Topical ocular lubricants are recommended for two to three days after the injection to treat these effects. Particular risks after an intravitreal injection include postinjection infective endophthalmitis, increased eye inflammation, retinal detachment and increased intraocular pressure.
Patients should be monitored closely by their ophthalmologist for complications and educated about when to return for urgent review. Important postinjection symptoms that require urgent review include a sudden decrease in vision, sensitivity to light or an increase in eye pain.
Contraindications
An important precaution is that the dexamethasone implant must not be inserted:
- in the presence of an ocular or periocular infection
- in an eye with uncontrolled or advanced glaucoma
- in a single chamber eye (aphakia; where the crystalline lens has been removed without replacement by an intraocular lens implant).
Conclusion
The dexamethasone implant is a slow-release intravitreal implant approved to treat macular oedema in patients with diabetic retinopathy, retinal vein occlusions or noninfectious uveitis. It can be used as first-line or adjunctive treatment in patients with noninfectious posterior uveitis, minimising the systemic effects of other forms of immunosuppression.
The implant is a useful second-line treatment for macular oedema secondary to diabetic retinopathy or retinal vein occlusions that is poorly responsive to anti-VEGF treatment. It is also a useful alternative when anti-VEGF treatment is contraindicated, such as during pregnancy or after a cerebral or cardiac ischaemic event. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.